Download as pptx, pdf, or txt
You might also like
- How To Read People Like A BookDocument165 pagesHow To Read People Like A Bookraihan223588% (8)
- Endodontic MCQ PDFDocument17 pagesEndodontic MCQ PDFYousef Hussain Ghannam89% (66)
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationDocument6 pagesKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)No ratings yet
- Clinical Face Sheet: G3P2, Pregnancy Uterine (PU), 37 Weeks and 5 Days AOG, Previous CS IIDocument14 pagesClinical Face Sheet: G3P2, Pregnancy Uterine (PU), 37 Weeks and 5 Days AOG, Previous CS IICezanne CruzNo ratings yet
- Gene Therapy - PresentationDocument19 pagesGene Therapy - PresentationElectRon ShajalNo ratings yet
- Communication: (Verbal and Non Verbal)Document18 pagesCommunication: (Verbal and Non Verbal)Dr. Honeylou Az. OpondaNo ratings yet
- Handout # 3 Mid 100 - 2020Document3 pagesHandout # 3 Mid 100 - 2020Ram AugustNo ratings yet
- Presentation Speaking Material Plus Sequences of Points We Will Be Discussing One After T6he OtherDocument13 pagesPresentation Speaking Material Plus Sequences of Points We Will Be Discussing One After T6he Otheratiqagha313No ratings yet
- Non-Verbal Communication 1st GroupDocument15 pagesNon-Verbal Communication 1st Groupmjtkd100% (1)
- Non Verbal Communication: by Dr. Nadia BassuoniDocument38 pagesNon Verbal Communication: by Dr. Nadia Bassuoniاسامة محمد السيد رمضانNo ratings yet
- Non-Verbal Communication: by V P BhagatDocument14 pagesNon-Verbal Communication: by V P BhagatSat SharmaNo ratings yet
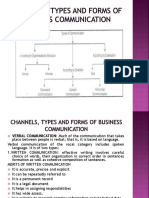
- Channels, Types and Forms of Business Communication PDFDocument36 pagesChannels, Types and Forms of Business Communication PDFGazala KhanNo ratings yet
- Non-Verbal ImmediacyDocument24 pagesNon-Verbal Immediacyf223192No ratings yet
- ProxemicsDocument15 pagesProxemicsDivia RainaNo ratings yet
- Doc-20221015-Wa0001 221109 000711Document21 pagesDoc-20221015-Wa0001 221109 000711PakcjcNo ratings yet
- CamileDocument42 pagesCamilebabypauNo ratings yet
- CommunicationDocument89 pagesCommunicationChristine LeroyNo ratings yet
- ProxemicsDocument9 pagesProxemicsMaria Cristina ChiruNo ratings yet
- Communication Is The Activity of Conveying Meaningful: InformationDocument6 pagesCommunication Is The Activity of Conveying Meaningful: InformationSridher BashattyNo ratings yet
- 05 NVCDocument42 pages05 NVCAkash KatariyaNo ratings yet
- Nonverbal 321 LectDocument8 pagesNonverbal 321 Lectapi-224355946No ratings yet
- Proxemics: BodyDocument38 pagesProxemics: BodyAbraham PanakalNo ratings yet
- Proxemics - WikipediaDocument10 pagesProxemics - WikipediaJared Cuento TransfiguracionNo ratings yet
- Advance Social Psychology AssignmentDocument21 pagesAdvance Social Psychology AssignmentDinesh Kumar GuptaNo ratings yet
- Sem1 NVCDocument7 pagesSem1 NVCdhrjmjnNo ratings yet
- English Language III TheoryDocument17 pagesEnglish Language III TheorycookinglikeNo ratings yet
- Ge 5 Module 4 Non Verbal CommunicationDocument5 pagesGe 5 Module 4 Non Verbal Communicationbyata pausanosNo ratings yet
- Language and Culture Kinesics-090330143118-Phpapp02Document117 pagesLanguage and Culture Kinesics-090330143118-Phpapp02عبداللہNo ratings yet
- Nonverbal CommunicationDocument13 pagesNonverbal Communicationwajidnawaz1No ratings yet
- Coms Revision: Models of CommunicationDocument11 pagesComs Revision: Models of Communicationjaya1816No ratings yet
- Reading 8.1.2 (Non-Verbal Communication)Document10 pagesReading 8.1.2 (Non-Verbal Communication)MohammedNo ratings yet
- I Can Read You Like A BookDocument7 pagesI Can Read You Like A BookNur Azizah RahmanNo ratings yet
- PROXEMICDocument11 pagesPROXEMICairaNo ratings yet
- Purposive Comminucation Chapters 1 5 1Document67 pagesPurposive Comminucation Chapters 1 5 1Dummy AccountNo ratings yet
- Speech CommunicationDocument3 pagesSpeech CommunicationDigna Burac-CollantesNo ratings yet
- Capitolul 8Document3 pagesCapitolul 8Alex PavelNo ratings yet
- Verbal and Non Verbal Communication 2019Document29 pagesVerbal and Non Verbal Communication 2019Russel Jil Gonzales100% (2)
- Non-Verbal Communication KinesicsDocument10 pagesNon-Verbal Communication Kinesics8005Girish Kumar DasNo ratings yet
- Non-Verbal Communication: Dr. Ravi ShankerDocument38 pagesNon-Verbal Communication: Dr. Ravi ShankerbattlestrokerNo ratings yet
- Social PerceptionDocument5 pagesSocial PerceptionAarzu KaurNo ratings yet
- Nonverbal Communication: Nonverbal Communication Is Usually Understood As The Process of Communication Through SendingDocument4 pagesNonverbal Communication: Nonverbal Communication Is Usually Understood As The Process of Communication Through SendingJawad ZafarNo ratings yet
- Animal and Human LanguageDocument33 pagesAnimal and Human LanguageAwu LupVaNo ratings yet
- Non-Verbal Communication Final 11Document14 pagesNon-Verbal Communication Final 11Sat SharmaNo ratings yet
- Non Verbal SymbolsDocument27 pagesNon Verbal SymbolsKelly magtotoNo ratings yet
- Communication Skills ReportDocument11 pagesCommunication Skills ReportDivyansh NandwanaNo ratings yet
- Final Report I Regional Research Congress "Forming Seeds": President of The CongressDocument11 pagesFinal Report I Regional Research Congress "Forming Seeds": President of The Congressronald palominoNo ratings yet
- Levels of CommunicationDocument3 pagesLevels of CommunicationMark Louise PacisNo ratings yet
- Speech Acts Assignment - 3Document4 pagesSpeech Acts Assignment - 3RabwianNo ratings yet
- Nature and Elements of CommunicationDocument23 pagesNature and Elements of Communicationybon MendozaNo ratings yet
- 1.the Concept of CommunicationDocument28 pages1.the Concept of CommunicationMADDUMAGE SAMPATHNo ratings yet
- Lesson 3 - Non Verbal CommunicationDocument47 pagesLesson 3 - Non Verbal Communicationjudel ArielNo ratings yet
- Speaking BasicsDocument52 pagesSpeaking BasicsnjcumartinNo ratings yet
- Communication Models: Lesson 1Document60 pagesCommunication Models: Lesson 1Tin PortuzuelaNo ratings yet
- Non-Verbal CommunicationDocument3 pagesNon-Verbal CommunicationAbhisha WhavalNo ratings yet
- NonverbalDocument5 pagesNonverbalapi-26784854No ratings yet
- Philosophical ReflectionDocument5 pagesPhilosophical Reflectionjonas davidNo ratings yet
- Kinesics of Body LanguageDocument117 pagesKinesics of Body LanguageShalvv100% (1)
- Module 3 - SOCIAL PERCEPTIONDocument18 pagesModule 3 - SOCIAL PERCEPTIONksnitya4No ratings yet
- The Nonverbal Factor: Exploring the Other Side of CommunicationFrom EverandThe Nonverbal Factor: Exploring the Other Side of CommunicationNo ratings yet
- Beyond Symptoms: A Guide to Dispel the Fear of the Human Body and FunctionsFrom EverandBeyond Symptoms: A Guide to Dispel the Fear of the Human Body and FunctionsNo ratings yet
- Handout # 10 Part 4Document5 pagesHandout # 10 Part 4Ram AugustNo ratings yet
- Competency Performance Checklist: Tagoloan Community CollegeDocument2 pagesCompetency Performance Checklist: Tagoloan Community CollegeRam AugustNo ratings yet
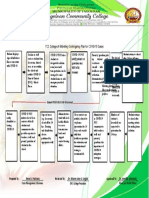
- TCC College of Midwifery Contingency Plan For COVID-19 CasesDocument1 pageTCC College of Midwifery Contingency Plan For COVID-19 CasesRam AugustNo ratings yet
- Health Informatics Qualifications and Ehealth Literacy: Week # 9-10 HandoutDocument2 pagesHealth Informatics Qualifications and Ehealth Literacy: Week # 9-10 HandoutRam AugustNo ratings yet
- EDD & AOG Computation: Expected Date of Delivery & Age of GestationDocument3 pagesEDD & AOG Computation: Expected Date of Delivery & Age of GestationRam AugustNo ratings yet
- Republic Act No. 7392 An Act Revising Republic Act No. 2644, As Amended, Otherwise Known As The Philippine Midwifery ActDocument6 pagesRepublic Act No. 7392 An Act Revising Republic Act No. 2644, As Amended, Otherwise Known As The Philippine Midwifery ActRam AugustNo ratings yet
- Handout # 10Document22 pagesHandout # 10Ram August100% (1)
- Handout # 3 Mid 100 - 2020Document3 pagesHandout # 3 Mid 100 - 2020Ram AugustNo ratings yet
- BPE Introduction To AnatomyDocument7 pagesBPE Introduction To AnatomyRam AugustNo ratings yet
- Note: Refer To The Structures Above and Familiarize The Functions of Each PartsDocument2 pagesNote: Refer To The Structures Above and Familiarize The Functions of Each PartsRam August100% (1)
- Descripción PVF Xistencias: Desc%Document18 pagesDescripción PVF Xistencias: Desc%Nelly NoemiNo ratings yet
- EHS Groin Hernia ClassificationDocument4 pagesEHS Groin Hernia ClassificationbogdanotiNo ratings yet
- Uspi LomotilDocument8 pagesUspi LomotilhaiduvnNo ratings yet
- RX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelDocument6 pagesRX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelntootNo ratings yet
- Radiological Chest SignsDocument15 pagesRadiological Chest SignsEzekiel ArtetaNo ratings yet
- All Things MoringaDocument40 pagesAll Things MoringaAnjee SugatriNo ratings yet
- Pharmacotherapy of TB - Handout (Final) 4-08Document3 pagesPharmacotherapy of TB - Handout (Final) 4-08Ahmedshaker21No ratings yet
- 3i T3 Implant Surgical Manual - CATMT3 - ENDocument67 pages3i T3 Implant Surgical Manual - CATMT3 - ENSalem RawashdahNo ratings yet
- Antifungal Catheter Lock Therapy 1Document8 pagesAntifungal Catheter Lock Therapy 1Dakota YamashitaNo ratings yet
- Experience The Power of Bio Active Protein: ReecureDocument2 pagesExperience The Power of Bio Active Protein: ReecureNirav HiinguNo ratings yet
- Diabetes, Sports and ExerciseDocument8 pagesDiabetes, Sports and ExerciseMateus AssisNo ratings yet
- ASPEN Critical Care - Susan BrantleyDocument44 pagesASPEN Critical Care - Susan BrantleyVitoria SilvaNo ratings yet
- Chapter 7 Cystic FibrosisDocument9 pagesChapter 7 Cystic FibrosisMariana DariiNo ratings yet
- Cambridge English For Nursing Grammar Practice Pre Intermediate Unit7Document2 pagesCambridge English For Nursing Grammar Practice Pre Intermediate Unit7Jorge CampiNo ratings yet
- Medicinal Chemistry 2 - AssignmentDocument6 pagesMedicinal Chemistry 2 - AssignmentRA TanvirNo ratings yet
- Chapter 2 - Components of Physical FitnessDocument9 pagesChapter 2 - Components of Physical FitnessMerynette Pangilinan VillaNo ratings yet
- Hypertension & Diabetis MellitusDocument51 pagesHypertension & Diabetis MellitusSuma_Ramesan_5373100% (1)
- Child Health Nursing NotesDocument9 pagesChild Health Nursing NotesBindhu RaniNo ratings yet
- Pregnancy Induced HypertensionDocument13 pagesPregnancy Induced HypertensionSally JaneNo ratings yet
- Enrichment Activities C1: Grade Level: Six Quarter: First Subject: MAPEH-HealthDocument11 pagesEnrichment Activities C1: Grade Level: Six Quarter: First Subject: MAPEH-HealthARLENE MARASIGAN100% (1)
- Obat UperioDocument5 pagesObat UperioAnonymous Aa6VAStNo ratings yet
- Manuver Head Tilt-Chin Lift-Jaw ThrustDocument6 pagesManuver Head Tilt-Chin Lift-Jaw ThrustKevin CindarjoNo ratings yet
- Lilyasari2019 Article EconomicEvaluationOfSildenafilDocument9 pagesLilyasari2019 Article EconomicEvaluationOfSildenafilNajib Al FatinNo ratings yet
- Pricelist November2021Document20 pagesPricelist November2021Apotek C 8No ratings yet
- Ipgme&r Opd ScheduleDocument8 pagesIpgme&r Opd Schedulean o nymousNo ratings yet
- Antidiuretic HormoneDocument1 pageAntidiuretic HormoneFalaq2No ratings yet
- Association Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenDocument6 pagesAssociation Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenHarun joel tatipataNo ratings yet