Download as pptx, pdf, or txt
You might also like
- SEM (Scanning Electron Microscope)Document47 pagesSEM (Scanning Electron Microscope)devikaNo ratings yet
- Advancement in Diagnostic Aids For Oral Premalignant Lesions: A ReviewDocument5 pagesAdvancement in Diagnostic Aids For Oral Premalignant Lesions: A ReviewAl RawdhaNo ratings yet
- Early Diagnosis Oral CancerDocument27 pagesEarly Diagnosis Oral Cancermy_scribd_account11No ratings yet
- s41405 020 0030 ZDocument7 pagess41405 020 0030 ZkcsaputraNo ratings yet
- Assessment of Clinical Examination Validity in Oral Cancer Risk PatientsDocument7 pagesAssessment of Clinical Examination Validity in Oral Cancer Risk PatientsVera Radojkova NikolovskaNo ratings yet
- The Ocular Microbiome: Molecular Characterization of A Unique and Low Microbial EnvironmentDocument24 pagesThe Ocular Microbiome: Molecular Characterization of A Unique and Low Microbial EnvironmentOkta Kurniawan SaputraNo ratings yet
- Artifacts in CytopathologyDocument25 pagesArtifacts in Cytopathologysamuel adagaNo ratings yet
- Histopath Lec - Week 2 - Topic 2Document11 pagesHistopath Lec - Week 2 - Topic 2Juren LasagaNo ratings yet
- Chairside Diagnosis For Plaque AssociatedDocument7 pagesChairside Diagnosis For Plaque AssociatedMohammed NabeelNo ratings yet
- JCytol324253-2196445 060604Document8 pagesJCytol324253-2196445 060604SunilNo ratings yet
- COMPLETEPAPER Ready To Pub - PYOGENIC GRANULOMADocument6 pagesCOMPLETEPAPER Ready To Pub - PYOGENIC GRANULOMAolanrewajuoduolaNo ratings yet
- Ce SasaDocument16 pagesCe SasaKoasNo ratings yet
- Ijmm 47 5 4916 PDFDocument15 pagesIjmm 47 5 4916 PDFAlinaNo ratings yet
- Cervical CytologyDocument9 pagesCervical CytologyAezel Cruz100% (1)
- Lesson-21 Exfoliative Cytology PDFDocument4 pagesLesson-21 Exfoliative Cytology PDFSasa AbassNo ratings yet
- 3.podoplanin Antibody MainDocument6 pages3.podoplanin Antibody MainNitin KhanduriNo ratings yet
- E.C - Nithya - HistoryDocument3 pagesE.C - Nithya - HistoryJeyachandran MariappanNo ratings yet
- Histopath 1Document15 pagesHistopath 1AnonymoussssssNo ratings yet
- CD Final PDFDocument19 pagesCD Final PDFfarzanasulaiman07No ratings yet
- Deep Learning Model For Tongue Cancer Diagnosis UsDocument10 pagesDeep Learning Model For Tongue Cancer Diagnosis UsDaniel PancuNo ratings yet
- Early Detection Oral CDocument13 pagesEarly Detection Oral CMuhammad Ikhsan ChaniagoNo ratings yet
- Journal Reading - Ulya Jihan Muna - G4A020040Document14 pagesJournal Reading - Ulya Jihan Muna - G4A020040jihan ulNo ratings yet
- Metabolomics Approaches in Oral Leukoplakia: A Mini ReviewDocument6 pagesMetabolomics Approaches in Oral Leukoplakia: A Mini ReviewAlif YansyahNo ratings yet
- Velscope: Shedding Light On Its Ideal Application: AcronymsDocument7 pagesVelscope: Shedding Light On Its Ideal Application: AcronymsSaraswita Gabriellah SaetikhoNo ratings yet
- Precancerous Lesions of Oral CavityDocument119 pagesPrecancerous Lesions of Oral CavityigakalaNo ratings yet
- Metabolomics and Lipidomics Approaches in Human TeDocument15 pagesMetabolomics and Lipidomics Approaches in Human TeanxNo ratings yet
- 2022 Dentaldefects Environmental EHP10208Document12 pages2022 Dentaldefects Environmental EHP10208Senussi IbtisamNo ratings yet
- Lesson 1Document3 pagesLesson 1Krizza UrmazaNo ratings yet
- Evaluation of Various Oral Cancer Diagnostic TechniqueDocument13 pagesEvaluation of Various Oral Cancer Diagnostic TechniqueSelvaArockiamNo ratings yet
- Journal Reading - Ulya Jihan Muna - G4A020040Document15 pagesJournal Reading - Ulya Jihan Muna - G4A020040jihan ulNo ratings yet
- Diagnostic CytologyDocument32 pagesDiagnostic Cytologyclaw foreSK TeamNo ratings yet
- An Objective Approach To DED Severity Sullivan Et Al IOVS 12-2010Document6 pagesAn Objective Approach To DED Severity Sullivan Et Al IOVS 12-2010Meyva HannaNo ratings yet
- Velscope Oral PremalignancyDocument5 pagesVelscope Oral PremalignancySusanaSanoNo ratings yet
- Antibacterial EffectsDocument8 pagesAntibacterial EffectsElliot AldersonNo ratings yet
- Neoplasia OcularDocument18 pagesNeoplasia OcularRaul DiazNo ratings yet
- Histopathological Variations in Ameloblastoma - Cases in A Tertiary Care Center of NepalDocument7 pagesHistopathological Variations in Ameloblastoma - Cases in A Tertiary Care Center of NepalDinesh YadavNo ratings yet
- 7.review On Strategies and Technologies For Exosome Isolation and Puri CationDocument18 pages7.review On Strategies and Technologies For Exosome Isolation and Puri Cationsnow silverNo ratings yet
- Kemiii OoooDocument17 pagesKemiii Oooosgfdjwwt88No ratings yet
- GRAEFES D 11 00688reviewedDocument41 pagesGRAEFES D 11 00688reviewedSayoki ghosgNo ratings yet
- The Incipient Caries: January 2013Document6 pagesThe Incipient Caries: January 2013Ramya ReddyNo ratings yet
- Animal Cytology (Compatibility Mode)Document13 pagesAnimal Cytology (Compatibility Mode)AdarshBijapurNo ratings yet
- Editorial: Odontogenic TumorsDocument2 pagesEditorial: Odontogenic TumorsEdison CadenaNo ratings yet
- Investigations of Oral Cancer Revised 2022Document32 pagesInvestigations of Oral Cancer Revised 2022elle70503No ratings yet
- Dart CICDocument1 pageDart CICcherruskaNo ratings yet
- Diseases of The Vitreo-Macular InterfaceDocument126 pagesDiseases of The Vitreo-Macular InterfaceCarlos OrtegaNo ratings yet
- TissuesDocument27 pagesTissuesAngela Nicole Udan100% (1)
- Evaluation of Biodentine PulpotomyDocument6 pagesEvaluation of Biodentine PulpotomygiselaNo ratings yet
- 2018 Management Update of Potentially Premalignant Oral Epithelial LesionsDocument9 pages2018 Management Update of Potentially Premalignant Oral Epithelial LesionsEmiliaAndreeaBalanNo ratings yet
- Histology Lecture 2017 HandoutDocument11 pagesHistology Lecture 2017 HandoutqNo ratings yet
- Smear LayerDocument14 pagesSmear Layersandra del pilarNo ratings yet
- Imprint CytologyDocument3 pagesImprint Cytologyhimanshusolanki1016No ratings yet
- PIIS2212440318300920Document12 pagesPIIS2212440318300920EmiliaAndreeaBalanNo ratings yet
- Magnetic Bead-Based Salivary Peptidome Profiling For Periodontal-Orthodontic TreatmentDocument8 pagesMagnetic Bead-Based Salivary Peptidome Profiling For Periodontal-Orthodontic TreatmentMárcio LMSNo ratings yet
- Archives of Oral Biology 102 (2019) 122-127Document6 pagesArchives of Oral Biology 102 (2019) 122-127fghdhmdkhNo ratings yet
- Bmri2022 2739869Document21 pagesBmri2022 2739869saifulmangopo123No ratings yet
- Salivary Biomarkers in The Detection of Oral Cancer. 07 OCT BienDocument5 pagesSalivary Biomarkers in The Detection of Oral Cancer. 07 OCT BienKevin FossNo ratings yet
- Lesson 21 PDFDocument4 pagesLesson 21 PDFShirmayne TangNo ratings yet
- Early Diagnosis and Treatment in Two Cases of Microinvasive Squamous Cell Carcinoma On The PalateDocument2 pagesEarly Diagnosis and Treatment in Two Cases of Microinvasive Squamous Cell Carcinoma On The Palatefatimah nurNo ratings yet
- Ameloblastoma Arising in A Dentigerous Cyst: Report of Three CasesDocument6 pagesAmeloblastoma Arising in A Dentigerous Cyst: Report of Three Casessantos eddyNo ratings yet
- Caac172 PDFDocument4 pagesCaac172 PDFTaufiqurrahman Abdul DjabbarNo ratings yet
- Department of Oral Medicine & Radiology: Click Here To RegisterDocument1 pageDepartment of Oral Medicine & Radiology: Click Here To RegisterdevikaNo ratings yet
- Oral Manifestation of Anemia 1Document2 pagesOral Manifestation of Anemia 1devikaNo ratings yet
- Nextdecadefacetoface Finalversion 12 Jan 2020Document12 pagesNextdecadefacetoface Finalversion 12 Jan 2020devikaNo ratings yet
- State Conference 21Document6 pagesState Conference 21devikaNo ratings yet
- CS0005873Document1 pageCS0005873heryantoNo ratings yet
- Reno Hells Angel Troy Regas DetailsDocument34 pagesReno Hells Angel Troy Regas Detailsapi-3787993100% (2)
- Apache Airflow Fundamentals Study GuideDocument7 pagesApache Airflow Fundamentals Study GuideDonNo ratings yet
- Motorola Moto E4 Plus - Schematic Diagarm PDFDocument59 pagesMotorola Moto E4 Plus - Schematic Diagarm PDFRoger Ardila0% (1)
- FBI Special Agent in Charge Eric W. Sporre Request Criminal Prosecution Foreclosure FRAUDDocument101 pagesFBI Special Agent in Charge Eric W. Sporre Request Criminal Prosecution Foreclosure FRAUDNeil GillespieNo ratings yet
- Principles of Marketing Eighth Edition Philip Kotler and Gary ArmstongDocument17 pagesPrinciples of Marketing Eighth Edition Philip Kotler and Gary ArmstongAnonymous p0bBEKNo ratings yet
- Sterling Selections Corp v. LLDA GR 171427, 2011Document12 pagesSterling Selections Corp v. LLDA GR 171427, 2011doora keysNo ratings yet
- NCKH ĐỊNH TÍNHDocument75 pagesNCKH ĐỊNH TÍNHnguyennguyen.31221022808No ratings yet
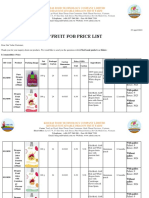
- 1.kim Hai Fob Price List 2019 (New)Document6 pages1.kim Hai Fob Price List 2019 (New)Khanh QuocNo ratings yet
- BBA Project Guidelines-2016Document38 pagesBBA Project Guidelines-2016vntkhatri100% (1)
- Migrate DHCP Scope(s) To Windows Server 2022 - PeteNetLiveDocument6 pagesMigrate DHCP Scope(s) To Windows Server 2022 - PeteNetLiveYudy KurniawanNo ratings yet
- Bescom Public Grievance Redressal System (PGRS) : User ManualDocument13 pagesBescom Public Grievance Redressal System (PGRS) : User Manualgurt sityNo ratings yet
- Jameco Part Number 838680: Distributed byDocument20 pagesJameco Part Number 838680: Distributed byAlan FuentesNo ratings yet
- 400kv DC (Quad) Padghe (PG) - Kharghar Line Check Survey Updated TS - 19.04.2023Document11 pages400kv DC (Quad) Padghe (PG) - Kharghar Line Check Survey Updated TS - 19.04.2023Akd DeshmukhNo ratings yet
- Capital MArket MCQDocument11 pagesCapital MArket MCQSoumit DasNo ratings yet
- FBI Mandalay Bay FOIA Production 2Document15 pagesFBI Mandalay Bay FOIA Production 2NoloContendere100% (4)
- Check User's Sign-In Activity Logs Log On AAD Portal Active Directory Activity Sing inDocument3 pagesCheck User's Sign-In Activity Logs Log On AAD Portal Active Directory Activity Sing inGauriNo ratings yet
- Gas Velocity CalculatorDocument5 pagesGas Velocity CalculatoresutjiadiNo ratings yet
- Customer Engagement - A Literature Review: October 2016Document7 pagesCustomer Engagement - A Literature Review: October 2016Nlke NzkeNo ratings yet
- Tax Structure in IndiaDocument33 pagesTax Structure in IndiaVinayak Saxena100% (1)
- Beam Design Detail Report: Material and Design DataDocument33 pagesBeam Design Detail Report: Material and Design DataazwanNo ratings yet
- Berger Paints ProfileDocument35 pagesBerger Paints ProfileVimal JainNo ratings yet
- LKS1Document34 pagesLKS1Vijay SarojNo ratings yet
- DigiIvy Products US 052814Document1 pageDigiIvy Products US 052814akiridino0% (1)
- Listado JM Motors Jun-2020Document291 pagesListado JM Motors Jun-2020OliverNo ratings yet
- New Salary Scales Updated February 2023 NAC ExtendedDocument2 pagesNew Salary Scales Updated February 2023 NAC ExtendedIon NNo ratings yet
- Matrix Review of Winnipeg Police ServiceDocument347 pagesMatrix Review of Winnipeg Police ServiceJames TurnerNo ratings yet
- Impact of GT, SFD and EIRP On System DesignDocument18 pagesImpact of GT, SFD and EIRP On System DesignExtreme DaysNo ratings yet
- GP Medium CorrectDocument2 pagesGP Medium CorrectJimmy JoeNo ratings yet
- Blank - Gold Maintenance Contract India PDFDocument5 pagesBlank - Gold Maintenance Contract India PDFJaganath PaniNo ratings yet