Download as pptx, pdf, or txt
You might also like
- Electrolyte ImbalanceDocument76 pagesElectrolyte ImbalanceSarah Racheal Akello100% (2)
- DIALYZERDocument2 pagesDIALYZERassilamor100% (1)
- Anticoagulation On DialysisDocument52 pagesAnticoagulation On DialysisFey100% (1)
- Differential Diagnosis of JaundiceDocument4 pagesDifferential Diagnosis of JaundiceVirag PatilNo ratings yet
- HyponatremiaDocument42 pagesHyponatremiaAbdu Raheem100% (1)
- 4 - Stroke FinalDocument74 pages4 - Stroke FinalSamir SkejicNo ratings yet
- Glomerulonephritis-1 (Dr. Soffa)Document58 pagesGlomerulonephritis-1 (Dr. Soffa)Rahmailla Khanza Diana FebriliantriNo ratings yet
- DialyzerDocument10 pagesDialyzerfatima rasheedNo ratings yet
- DIALYZERDocument13 pagesDIALYZERParthibarajan Pandiarajan100% (1)
- Renal DisordersDocument77 pagesRenal Disorderslorelee_espaldon100% (1)
- Long Case PresentationDocument3 pagesLong Case PresentationAkshat WaranNo ratings yet
- Colloids and CrystalooidsDocument42 pagesColloids and Crystalooidsلؤي زعيترNo ratings yet
- GlomerulonephritisDocument58 pagesGlomerulonephritisJosa Anggi Pratama0% (1)
- Cleaning and Disinfecting Hemodialysis Machines and StationsDocument14 pagesCleaning and Disinfecting Hemodialysis Machines and Stationsarun melepurackalNo ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
- Case Study JatDocument45 pagesCase Study JatHSEINNo ratings yet
- Intradialytic ComplicationsDocument5 pagesIntradialytic Complicationskane1978No ratings yet
- Pathophysiology of Atherosclerosis, Thrombosis and EmbolismDocument4 pagesPathophysiology of Atherosclerosis, Thrombosis and EmbolismKeshant Samaroo100% (1)
- HemodialysisDocument22 pagesHemodialysisAlyssa Agravante100% (3)
- Blood Transfusion Reactions: Dr. Madhuvan GuptaDocument42 pagesBlood Transfusion Reactions: Dr. Madhuvan GuptaDr. Madhuvan GuptaNo ratings yet
- Renal Replacement TherapyDocument50 pagesRenal Replacement TherapyMalueth Angui100% (1)
- Types of IV FluidsDocument6 pagesTypes of IV Fluidsharrisburrrg100% (1)
- Cardiogenic ShockDocument2 pagesCardiogenic ShockChristine QuironaNo ratings yet
- Liver Cirrhosis (VD)Document56 pagesLiver Cirrhosis (VD)HannaTashiaClaudiaNo ratings yet
- Diabetic NephropathyDocument198 pagesDiabetic Nephropathyapi-3824046100% (2)
- Renal System Practice Quiz: D. Reversal of The Oliguria Occurs With Fluid ReplacementDocument5 pagesRenal System Practice Quiz: D. Reversal of The Oliguria Occurs With Fluid Replacementمحمد حسينNo ratings yet
- Anemia 130809044630 Phpapp01Document21 pagesAnemia 130809044630 Phpapp01Siddharth Das100% (1)
- Lect15&16 Fluids&ElectrolytesDocument77 pagesLect15&16 Fluids&Electrolyteskhurram na100% (1)
- Anti Hypertensive Drugs - DiureticsDocument49 pagesAnti Hypertensive Drugs - DiureticsApurba Sarker Apu100% (1)
- Congestive Heart Failure PDFDocument49 pagesCongestive Heart Failure PDFVerinice NañascaNo ratings yet
- Polycythemia: (Primary & Secondary)Document16 pagesPolycythemia: (Primary & Secondary)Vanessa Camille DomingoNo ratings yet
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocument44 pagesPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarNo ratings yet
- Hemodialysis: By: Liana Lee SenciónDocument14 pagesHemodialysis: By: Liana Lee SenciónKavidu KeshanNo ratings yet
- Anemia IntroductionDocument15 pagesAnemia IntroductionNitesh Kotian100% (1)
- Chronic Renal FailureDocument46 pagesChronic Renal Failurestepharry08100% (1)
- Hyponatremia Algorithm: Onset Rapid ( 48 Hours) : 3% Onset Rapid ( 48 Hours) : May Consider 3% Nac LDocument2 pagesHyponatremia Algorithm: Onset Rapid ( 48 Hours) : 3% Onset Rapid ( 48 Hours) : May Consider 3% Nac Lmina000005100% (1)
- 1 Principles of HemodialysisDocument5 pages1 Principles of HemodialysisZaid Alfaathih100% (2)
- Peritoneal DialysisDocument56 pagesPeritoneal DialysisVanet100% (1)
- Esophageal VaricesDocument14 pagesEsophageal VaricesKarla So MejiaNo ratings yet
- Chronic Renal FailureDocument28 pagesChronic Renal FailuremarshmalouNo ratings yet
- Complication of Blood TransfusionDocument61 pagesComplication of Blood Transfusionতৌহিদ তপুNo ratings yet
- Kidney Anatomy PhysiologyDocument26 pagesKidney Anatomy PhysiologyAlexandra Demian CrisanNo ratings yet
- Enterocutaneous FistulaDocument34 pagesEnterocutaneous FistulaAkram ChalidNo ratings yet
- Anal Canal: Fissure in Ano HaemorrhoidsDocument37 pagesAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaNo ratings yet
- SyncopeDocument28 pagesSyncopeDurgesh PushkarNo ratings yet
- Complication of Peptic Ulcer: Department of Surgery S. S. Medical College Rewa and Associate GMH and SGMH RewaDocument76 pagesComplication of Peptic Ulcer: Department of Surgery S. S. Medical College Rewa and Associate GMH and SGMH RewaBrajesh MouryaNo ratings yet
- Renal TransplantationDocument33 pagesRenal TransplantationRohini Rai100% (1)
- Nutri WopsDocument4 pagesNutri WopsRizzy Ugay100% (1)
- Complications During Hemodialysis2007Document40 pagesComplications During Hemodialysis2007Gumarbio Setiadi ZakariaNo ratings yet
- Acute and Chronic CholecystitisDocument10 pagesAcute and Chronic Cholecystitisissam_1994No ratings yet
- GOUT Case StudyDocument3 pagesGOUT Case StudySunshine_Bacla_42750% (1)
- Renal Replacement TherapyDocument19 pagesRenal Replacement Therapyayuwulandari100% (1)
- AnemiaDocument32 pagesAnemiaSherina Christo100% (3)
- TypesDocument3 pagesTypesProser Faith TabaculdeNo ratings yet
- Case Study Liver CirrhosisDocument20 pagesCase Study Liver CirrhosisFate ZephyrNo ratings yet
- Hyperosmolar Hyperglycemic State (HHS)Document21 pagesHyperosmolar Hyperglycemic State (HHS)Malueth AnguiNo ratings yet
- Gouty ArthritisDocument12 pagesGouty ArthritisManoj KandoiNo ratings yet
- Acute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAcute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Membrane Materials and ModulesDocument23 pagesMembrane Materials and Modulesm_alodat6144No ratings yet
- Renal Tumors: DR. Mohamed ElgendyDocument27 pagesRenal Tumors: DR. Mohamed ElgendyDani DanyNo ratings yet
- Management of Pediatric Patients With Oxygen in The Acute SettingDocument10 pagesManagement of Pediatric Patients With Oxygen in The Acute SettingDani DanyNo ratings yet
- Renal Tubulointerstitial DiseasesDocument13 pagesRenal Tubulointerstitial DiseasesDani DanyNo ratings yet
- Diabetic NephropathyDocument43 pagesDiabetic NephropathyDani DanyNo ratings yet
- Renal DiseaseDocument85 pagesRenal DiseaseDani DanyNo ratings yet
- Yousaf Khan Renal Dialysis Lecturer Ipms-KmuDocument14 pagesYousaf Khan Renal Dialysis Lecturer Ipms-KmuDani DanyNo ratings yet
- Renal Disease in PregnancyDocument19 pagesRenal Disease in PregnancyDani DanyNo ratings yet
- End Stage Renal Disease (ESRD)Document21 pagesEnd Stage Renal Disease (ESRD)Dani DanyNo ratings yet
- Hypertension and Kidney: DR - Suresh KumarDocument15 pagesHypertension and Kidney: DR - Suresh KumarDani DanyNo ratings yet
- Type of Dialyzers, Clearance and BiocompatibilityDocument53 pagesType of Dialyzers, Clearance and BiocompatibilityDani DanyNo ratings yet
- History of Dialysis: DR Manjunath JDocument65 pagesHistory of Dialysis: DR Manjunath JDani Dany100% (1)
- Complications of Hemodialysis: DR Ashok Bhat Consultant Nephrologist KMC Hospital Ambedkar Circle MangaloreDocument32 pagesComplications of Hemodialysis: DR Ashok Bhat Consultant Nephrologist KMC Hospital Ambedkar Circle MangaloreDani DanyNo ratings yet
- BSC MLT Syllabus 2020 - SeptemberDocument70 pagesBSC MLT Syllabus 2020 - SeptemberDani DanyNo ratings yet
- Dialysis Adequacy - DemystifiedDocument24 pagesDialysis Adequacy - DemystifiedDani DanyNo ratings yet
- Basics of HemodialysisDocument43 pagesBasics of HemodialysisDani Dany100% (1)
- Plasma P Here SisDocument24 pagesPlasma P Here SisDani DanyNo ratings yet
- MD (Med) DM (Neph) DNB (Neph) - Associate Professor - KMC MangaloreDocument1 pageMD (Med) DM (Neph) DNB (Neph) - Associate Professor - KMC MangaloreDani DanyNo ratings yet
- Ditty Dominic Appointment LetterDocument1 pageDitty Dominic Appointment LetterDani DanyNo ratings yet
- Sanitary Engineering Lec.: November 2015Document110 pagesSanitary Engineering Lec.: November 2015Dynamo DSNo ratings yet
- Dte Named SeriesDocument4 pagesDte Named Seriesdhavit wijayantoNo ratings yet
- Caracksil Acrylic PasteDocument3 pagesCaracksil Acrylic PasteHaradhon DattaNo ratings yet
- Thin Film Deposition TechniquesDocument67 pagesThin Film Deposition TechniquesOmar Bin Harun TalhaNo ratings yet
- Structure Factor PDFDocument28 pagesStructure Factor PDFAndrea EspinosaNo ratings yet
- Oxygen and Silver Nanoparticle Aerosol Magnetohydrodynamic Power CycleDocument13 pagesOxygen and Silver Nanoparticle Aerosol Magnetohydrodynamic Power CyclealooNo ratings yet
- Lecture-1 - Introduction and Course PolicyDocument25 pagesLecture-1 - Introduction and Course PolicySibasish RoutNo ratings yet
- Preparation and Melting/Freezing Characteristics of Cu/Paraffin Nanofluid As Phase-Change Material (PCM)Document5 pagesPreparation and Melting/Freezing Characteristics of Cu/Paraffin Nanofluid As Phase-Change Material (PCM)Anan DhiNo ratings yet
- Lec19 PDFDocument8 pagesLec19 PDFrigobertoguerragNo ratings yet
- Coker DrumsDocument33 pagesCoker DrumsJosNo ratings yet
- Test 1 RevDocument6 pagesTest 1 RevSAYAN BAGCHINo ratings yet
- COMTECH LIU Upto 144FDocument4 pagesCOMTECH LIU Upto 144Fparth mendirattaNo ratings yet
- CH311 - Experiment 6 - Sterol Extraction From Sea WaterDocument2 pagesCH311 - Experiment 6 - Sterol Extraction From Sea WaterNarelle IaumaNo ratings yet
- Development of A Virtual Wiredrawing Tool For Process Analysis and OptimizationDocument7 pagesDevelopment of A Virtual Wiredrawing Tool For Process Analysis and OptimizationPhani KumarNo ratings yet
- ASTM D 5383 - 02 R03 LightfastnessDocument6 pagesASTM D 5383 - 02 R03 LightfastnessJohnNo ratings yet
- Agard Ag 304Document68 pagesAgard Ag 304greatsteelNo ratings yet
- PI - Technicoll - 9260 - GB - TDS PVAcDocument2 pagesPI - Technicoll - 9260 - GB - TDS PVAcThịnh HuỳnhNo ratings yet
- Student Design Lab Report Comparison of Different Types of WeldsDocument26 pagesStudent Design Lab Report Comparison of Different Types of WeldsSylvester WafulaNo ratings yet
- Safor MR200 PDFDocument41 pagesSafor MR200 PDFevolussem0% (1)
- Bending Stresses & Direct Stresses CombinedDocument12 pagesBending Stresses & Direct Stresses Combinedvsathees2350% (2)
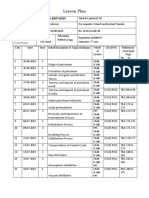
- Lesson Plan: Course Start Date Subject: Code/NameDocument3 pagesLesson Plan: Course Start Date Subject: Code/Nameanon_348923763No ratings yet
- Typical Grade of Cellulose EthersDocument25 pagesTypical Grade of Cellulose EthersDang Chi Cong0% (1)
- Rock Blasting 12Document39 pagesRock Blasting 12Anthoni Mansilla100% (1)
- Safety Data Sheet: 1. Product and Company IdentificationDocument4 pagesSafety Data Sheet: 1. Product and Company Identificationmohamed AdelNo ratings yet
- Widest Selection of Grouting Equipment in The WorldDocument6 pagesWidest Selection of Grouting Equipment in The Worldjet toledoNo ratings yet
- 263 269 JMTR Oct16Document7 pages263 269 JMTR Oct16Taniadi SuriaNo ratings yet
- Vacuum Coating of Plastic OpticsDocument15 pagesVacuum Coating of Plastic OpticsSasiKumar PetchiappanNo ratings yet
- Compressed Gas Cylinders Safety ChecklistDocument4 pagesCompressed Gas Cylinders Safety Checklistfathul syaafNo ratings yet
- Manganese Oxidation StatesDocument4 pagesManganese Oxidation StatesxbokyxNo ratings yet