Download as ppt, pdf, or txt
You might also like
- Dispensing, Incompatibilities, and Adverse Drug Reactions Answer Key-PINK PACOPDocument78 pagesDispensing, Incompatibilities, and Adverse Drug Reactions Answer Key-PINK PACOPBilly Vince AlquinoNo ratings yet
- 7 Drug StudyDocument17 pages7 Drug StudyMa. Mechile MartinezNo ratings yet
- Update in Acute Ischemic Stroke Treatment: Aldy Safrudddin RambeDocument33 pagesUpdate in Acute Ischemic Stroke Treatment: Aldy Safrudddin RambeEdwin DestraNo ratings yet
- Advances in Acute Stroke Treatment 2020Document6 pagesAdvances in Acute Stroke Treatment 2020ayman shomanNo ratings yet
- Kegawatan Respirasi Pada Keganasan Rongga ToraksDocument57 pagesKegawatan Respirasi Pada Keganasan Rongga ToraksChristian HarnatNo ratings yet
- Vas OpressorDocument41 pagesVas Opressorstevanus handrawanNo ratings yet
- Peer Review Version: ManuscriptDocument37 pagesPeer Review Version: ManuscriptQui Nguyen MinhNo ratings yet
- Khorsand 2023 Not All Shock States Are Created EqualDocument25 pagesKhorsand 2023 Not All Shock States Are Created EqualLê Huy HoàngNo ratings yet
- Adjunctive Therapies For Ventricular Arrhythmia ManagementDocument10 pagesAdjunctive Therapies For Ventricular Arrhythmia ManagementsaikrishnaNo ratings yet
- Respiratory Failure in Acute Heart Failure Workshop SingkatDocument35 pagesRespiratory Failure in Acute Heart Failure Workshop SingkatYun ZhaNo ratings yet
- Sinusitis Complications - DR - AnupDocument33 pagesSinusitis Complications - DR - AnupDr. Janarthanan VNo ratings yet
- Estados de ChoqueDocument25 pagesEstados de ChoqueKarina Moreno PalacioNo ratings yet
- Neurocritical Care For Patients With Ischemic.6Document30 pagesNeurocritical Care For Patients With Ischemic.6psukezNo ratings yet
- Prevention of DVT & PE-1Document12 pagesPrevention of DVT & PE-1arongeremewNo ratings yet
- Pulmonary EmbolismDocument61 pagesPulmonary Embolismjhk0428No ratings yet
- Treatment of Acute Ischemic StrokeDocument25 pagesTreatment of Acute Ischemic StrokeLauraGutierrezNo ratings yet
- Akut Limb IskemikDocument31 pagesAkut Limb IskemikLaluMuhammadSabarSetiawanNo ratings yet
- Kuliah Kriris HTDocument29 pagesKuliah Kriris HTDiska irmadhaniNo ratings yet
- Jha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseDocument5 pagesJha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseProdi Bedah SarafNo ratings yet
- Cardioversion of Atrial Fibrillation and AtrialDocument13 pagesCardioversion of Atrial Fibrillation and AtrialLabontu IustinaNo ratings yet
- Management of Acute Ischemic Stroke Specific Focus.21Document11 pagesManagement of Acute Ischemic Stroke Specific Focus.21Marina SolansNo ratings yet
- PDF Acute Stroke Care James Grotta Ebook Full ChapterDocument53 pagesPDF Acute Stroke Care James Grotta Ebook Full Chapteranne.oconnor830100% (6)
- EPISTAXIS - RifkiDocument21 pagesEPISTAXIS - RifkiIta Aprilia SaktiNo ratings yet
- RUG Tudy: Medicatio N Action Indication Contraindication Adverse Effects Nursing Considerati ONDocument4 pagesRUG Tudy: Medicatio N Action Indication Contraindication Adverse Effects Nursing Considerati ONGiselle EstoquiaNo ratings yet
- Cardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureDocument13 pagesCardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureGian CarloNo ratings yet
- Anti PlateletsDocument11 pagesAnti PlateletsMuhammed AhmedNo ratings yet
- Reconstructive Endovascular Treatment For Basilar Artery Trunk Aneurysms: Complications and Clinical and Angiography OutcomesDocument7 pagesReconstructive Endovascular Treatment For Basilar Artery Trunk Aneurysms: Complications and Clinical and Angiography OutcomesRafika Ayu NadiaNo ratings yet
- Stroke Program Education May2022Document22 pagesStroke Program Education May2022Laura VelaNo ratings yet
- Electrical Storm 2020Document13 pagesElectrical Storm 2020Aníbal José Arroyo RodríguezNo ratings yet
- Sensors 19 02533Document16 pagesSensors 19 02533priyaNo ratings yet
- Aneurysmorrhaphy (Eng)Document14 pagesAneurysmorrhaphy (Eng)Harlan IdrisNo ratings yet
- Acute Ischaemic Stroke: Recent Advances in Reperfusion TreatmentDocument11 pagesAcute Ischaemic Stroke: Recent Advances in Reperfusion TreatmentJose MartinezNo ratings yet
- Hypertensive Crisis: Management ofDocument45 pagesHypertensive Crisis: Management ofAz RifkiNo ratings yet
- Bmjspcare 2021 003427.fullDocument5 pagesBmjspcare 2021 003427.full5qp2gphgkyNo ratings yet
- Role of CT and MRI in Stroke DiagnosisDocument51 pagesRole of CT and MRI in Stroke DiagnosisBokuma KuciNo ratings yet
- Vasoactive Therapy in Shock - 2021 - BjaeDocument8 pagesVasoactive Therapy in Shock - 2021 - BjaeJojo PutriNo ratings yet
- Esc 2023 CutDocument16 pagesEsc 2023 CutalitrnfbNo ratings yet
- 2022 Perioperative Complications of Transvenous Embolization of Ruptured Intracranial Arteriovenous MalformationsDocument7 pages2022 Perioperative Complications of Transvenous Embolization of Ruptured Intracranial Arteriovenous MalformationsstaseaditNo ratings yet
- The Golden Hour: Acute Ischemic StrokeDocument9 pagesThe Golden Hour: Acute Ischemic StrokeKanliajie Kresna KastiantoNo ratings yet
- Musallam 2018Document7 pagesMusallam 2018Koup NuNo ratings yet
- 1 s2.0 S0735109720344909 MainDocument13 pages1 s2.0 S0735109720344909 MainIndira Ulfa DunandNo ratings yet
- Overview of Mechanical Thrombectomy TechniquesDocument8 pagesOverview of Mechanical Thrombectomy Techniquesjaknews adminNo ratings yet
- Ekran Resmi 2024-03-03 - 11.14.29Document74 pagesEkran Resmi 2024-03-03 - 11.14.29mryozdmr123No ratings yet
- Fluidoterapia - Critical CareDocument26 pagesFluidoterapia - Critical CareMario M. Marchand GonzalesNo ratings yet
- BALILI- DRUG STUDYDocument4 pagesBALILI- DRUG STUDYMary Ann BaliliNo ratings yet
- 2022 The Intensive Care Management of Acute Ischaemic StrokeDocument9 pages2022 The Intensive Care Management of Acute Ischaemic StrokeOmar Alejandro Agudelo ZuluagaNo ratings yet
- Managing Anticoagulation and Dual Antiplatelet Therapy in Patients With Active Bleed or Upcoming Procedure A Scoping Review 1Document12 pagesManaging Anticoagulation and Dual Antiplatelet Therapy in Patients With Active Bleed or Upcoming Procedure A Scoping Review 1Edward ElBuenoNo ratings yet
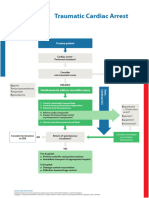
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteDocument1 pagePoster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteangelologrilloNo ratings yet
- 109890management StrokeDocument33 pages109890management StrokeAndleeb GanaieNo ratings yet
- Rios Navarro2019Document19 pagesRios Navarro2019Pratama InsaniNo ratings yet
- Atrial Fibrillation: Clinical PracticeDocument9 pagesAtrial Fibrillation: Clinical PracticeenesNo ratings yet
- Cardiovascular DisordersDocument15 pagesCardiovascular DisordersAzielle Joyce RosquetaNo ratings yet
- Ischaemic Stroke FMDocument137 pagesIschaemic Stroke FMDina AlOtaibiNo ratings yet
- Case Series: Radiofrequency Cathether Ablation of Atrioventricular Nodal Reentrant Tachycardia in OctogeneriansDocument5 pagesCase Series: Radiofrequency Cathether Ablation of Atrioventricular Nodal Reentrant Tachycardia in OctogeneriansAttilio Del RossoNo ratings yet
- Effects of Continuous Hypertonic Saline Infusion On Perihemorrhagic Edema EvolutionDocument8 pagesEffects of Continuous Hypertonic Saline Infusion On Perihemorrhagic Edema Evolutionwe sagara dewiNo ratings yet
- JJK s3Document7 pagesJJK s3achurocks561No ratings yet
- 01 Cir 72 6 1321Document6 pages01 Cir 72 6 1321YabesNo ratings yet
- Overview of Stroke - Knowledge at AMBOSSDocument19 pagesOverview of Stroke - Knowledge at AMBOSSandimija16No ratings yet
- Journal Reading Transcatheter Aortic Valve Replacement Under Monitored Anesthesia Care Versus General Anesthesia With IntubationDocument23 pagesJournal Reading Transcatheter Aortic Valve Replacement Under Monitored Anesthesia Care Versus General Anesthesia With IntubationTomy SandriyaNo ratings yet
- Limb Ischemia VascularDocument6 pagesLimb Ischemia Vascularalbadrimohammed1997No ratings yet
- Penyakit Kardiovaskular Yang Sering DijumpaiDocument121 pagesPenyakit Kardiovaskular Yang Sering Dijumpaiandikaagus13No ratings yet
- Hypertension Control in African-American Patients With Chronic Kidney DiseaseDocument3 pagesHypertension Control in African-American Patients With Chronic Kidney Diseaseandikaagus13No ratings yet
- Panic DisorderDocument10 pagesPanic Disorderandikaagus13No ratings yet
- Panic DisorderDocument10 pagesPanic Disorderandikaagus13No ratings yet
- Stem Cells For Myocardial Repair: Oren Caspi and Lior GepsteinDocument12 pagesStem Cells For Myocardial Repair: Oren Caspi and Lior Gepsteinandikaagus13No ratings yet
- Linfoma Non HodgkinDocument5 pagesLinfoma Non Hodgkinandikaagus13No ratings yet
- Conversion of Units of Volume and Capacity: WorkedDocument1 pageConversion of Units of Volume and Capacity: WorkedPaul TurnerNo ratings yet
- K01 Group 5Document42 pagesK01 Group 5Miss MichelleNo ratings yet
- Oxygen ToxicityDocument11 pagesOxygen ToxicityDavid Rendra MahardikaNo ratings yet
- Acp CBC 1Document52 pagesAcp CBC 1Danny R. SalvadorNo ratings yet
- Construction Sites Fatalities and Injuries: Eng - Ey BN Mnbass Al-AdailehDocument7 pagesConstruction Sites Fatalities and Injuries: Eng - Ey BN Mnbass Al-AdaileheyassadailehNo ratings yet
- Personal FinanceDocument32 pagesPersonal FinancePrincess MogulNo ratings yet
- Certificate IV in Commercial Cookery Sit 40516Document13 pagesCertificate IV in Commercial Cookery Sit 40516Tikaram GhimireNo ratings yet
- Ich Guidelines For Stability Testing of New Drug Substance and Drug ProductsDocument39 pagesIch Guidelines For Stability Testing of New Drug Substance and Drug ProductsRahul LakhaniNo ratings yet
- Pbl-Gin Urine Test (Feme)Document11 pagesPbl-Gin Urine Test (Feme)KarthigaRamanNo ratings yet
- Nagpur Metro Region PlanDocument627 pagesNagpur Metro Region PlanReddycoke100% (1)
- MRXBOXAB-ECO (3 5) - AESW - MVHR For Wall MountingDocument12 pagesMRXBOXAB-ECO (3 5) - AESW - MVHR For Wall MountingDan RotariNo ratings yet
- 07 Gyproc Eas-Fill COSHH Ass'tDocument2 pages07 Gyproc Eas-Fill COSHH Ass'tphil.jacksonNo ratings yet
- Scope and Sequence - Cookery - 10Document1 pageScope and Sequence - Cookery - 10JP AballeNo ratings yet
- Introduction To Petroleum Engineering - Lecture 3 - 12-10-2012 - Final PDFDocument19 pagesIntroduction To Petroleum Engineering - Lecture 3 - 12-10-2012 - Final PDFshanecarlNo ratings yet
- BasuhTanganDenganBetul BIDocument1 pageBasuhTanganDenganBetul BIAdnan ShamsudinNo ratings yet
- Family Neisseriaceae: Joy P. Calayo, RMT, MSMT UST Faculty of Pharmacy Dept. of Medical TechnologyDocument18 pagesFamily Neisseriaceae: Joy P. Calayo, RMT, MSMT UST Faculty of Pharmacy Dept. of Medical Technologypixholic100% (1)
- (Class 6) Fun With Magnets & Seperation of SubstancesDocument4 pages(Class 6) Fun With Magnets & Seperation of SubstancesSnigdha GoelNo ratings yet
- UNIT 3 Animal ProductionDocument15 pagesUNIT 3 Animal ProductionCarla Angela AngwasNo ratings yet
- Calamities in PhilippinesDocument44 pagesCalamities in PhilippinesMic BaldevaronaNo ratings yet
- Notice of Non Consent LiabilityDocument3 pagesNotice of Non Consent LiabilityandrewmmwilmotNo ratings yet
- Parasitology Table ProtozoaDocument10 pagesParasitology Table ProtozoaMae Rose Charlene MendozaNo ratings yet
- Global Stem Cell Therapy Market IHealthcareAnalyst, IncDocument2 pagesGlobal Stem Cell Therapy Market IHealthcareAnalyst, InciHealthcareAnalyst, Inc.No ratings yet
- Site OrientationDocument2 pagesSite OrientationHitesh VaghasiyaNo ratings yet
- 1 Introduction To Management Copy 2Document21 pages1 Introduction To Management Copy 2Angelica Camille B. AbaoNo ratings yet
- ICU PendnatDocument8 pagesICU PendnatTH HMNo ratings yet
- Earthquake Preparedness: Emergency Plan: What To Do Before An Earthquake - Be Prepared!Document16 pagesEarthquake Preparedness: Emergency Plan: What To Do Before An Earthquake - Be Prepared!Lenaj EbronNo ratings yet
- Answer To Case Study 1 - PASION, MARIA GIE-ANNELYN H.Document4 pagesAnswer To Case Study 1 - PASION, MARIA GIE-ANNELYN H.MARIAGIEANNELYNMANNYLYN PASIONNo ratings yet
- Mild Cognitive ImpairmentDocument13 pagesMild Cognitive ImpairmentFranz MiguelNo ratings yet
- Swc5-Ld: Specified PerformanceDocument1 pageSwc5-Ld: Specified PerformanceBenjamin MillerNo ratings yet