Download as pptx, pdf, or txt
You might also like
- Admiralty Quick Guide To ENC Symbols PDFDocument1 pageAdmiralty Quick Guide To ENC Symbols PDFMayankdeep Singh100% (3)
- CER Thuasne Knees 4Document12 pagesCER Thuasne Knees 4Mohammed HammedNo ratings yet
- Q3 Reading and Writing 11 Module 1Document26 pagesQ3 Reading and Writing 11 Module 1Bella Lauron100% (8)
- Safety Management System Structure: What Is A SMS?Document8 pagesSafety Management System Structure: What Is A SMS?Sayed AbbasNo ratings yet
- Ms. Andres - PHC Case StudyDocument48 pagesMs. Andres - PHC Case StudyJBLMGH EMPLOYEESCLINICNo ratings yet
- Subject Area No. 24 Safety Culture ImprovementDocument5 pagesSubject Area No. 24 Safety Culture ImprovementHarman SandhuNo ratings yet
- Free From Harm Final Report ResumenDocument4 pagesFree From Harm Final Report ResumenMiguel Armando Zúñiga OlivaresNo ratings yet
- Quality ImprovementDocument16 pagesQuality ImprovementNaufal HanifNo ratings yet
- BBS Pax ManualDocument189 pagesBBS Pax ManualorazaldlanorNo ratings yet
- Paradigm Shift To Safety Culture - May 2018 - YTDocument39 pagesParadigm Shift To Safety Culture - May 2018 - YTroxalNo ratings yet
- Safety Audit - An OverviewDocument26 pagesSafety Audit - An OverviewmaneeshNo ratings yet
- Domains Slide Pack QI Patient Safety Final v2Document36 pagesDomains Slide Pack QI Patient Safety Final v2Joel John Dela MercedNo ratings yet
- Safety Management SystemDocument7 pagesSafety Management SystemzombieNo ratings yet
- Behavior Based SafetyDocument20 pagesBehavior Based Safetysumitdel9136No ratings yet
- Effective Safety LeadershipDocument77 pagesEffective Safety LeadershipRyan SetiawanNo ratings yet
- Safety Culture What Why and HowDocument19 pagesSafety Culture What Why and HowDilip PatelNo ratings yet
- Report - Aubrey RecierdoDocument11 pagesReport - Aubrey RecierdoAubrey RecierdoNo ratings yet
- IHI-NSC SelfAssessmentTool NationalActionPlantoAdvancePatientSafetyDocument14 pagesIHI-NSC SelfAssessmentTool NationalActionPlantoAdvancePatientSafetyAnonymous 4gmLmemTPNo ratings yet
- 11 - Safety Health - Safety Culture PDFDocument31 pages11 - Safety Health - Safety Culture PDFVinashree PonneNo ratings yet
- Peran LeadershipDocument28 pagesPeran LeadershipnoviNo ratings yet
- Leadership Performance in Safety Management SystemsDocument10 pagesLeadership Performance in Safety Management SystemsMohamed AgrNo ratings yet
- Materi 3Document34 pagesMateri 3nur ariNo ratings yet
- Common Topics Common Topic 4: Safety CultureDocument4 pagesCommon Topics Common Topic 4: Safety CultureAnonymous ANmMebffKRNo ratings yet
- WHS Policies and Procedures Developed in Activity 2Document9 pagesWHS Policies and Procedures Developed in Activity 2vaibhavacademicmantraNo ratings yet
- Behavior-Based Safety - Virtual LearningDocument3 pagesBehavior-Based Safety - Virtual LearningDinesh PCNo ratings yet
- Proceeding 2Document102 pagesProceeding 2userscribd2011No ratings yet
- 4 Pillars of Safety Management System SMSDocument5 pages4 Pillars of Safety Management System SMSraja ahmedNo ratings yet
- Bbs SafetyDocument34 pagesBbs SafetyXis Ws plannerNo ratings yet
- Safety Culture 5: BackgroundDocument8 pagesSafety Culture 5: BackgroundGülten İbişNo ratings yet
- A Blueprint For Action 240619Document98 pagesA Blueprint For Action 240619abdu misbahNo ratings yet
- MaPSaF - GPDocument7 pagesMaPSaF - GPDwi SurantoNo ratings yet
- Behavior Based Safety BBSDocument67 pagesBehavior Based Safety BBSAkhilesh Kumar Singh100% (1)
- What Is Safety CultureDocument59 pagesWhat Is Safety CultureSuad BushiNo ratings yet
- JD OccupationalHealthandSafetyAdviser September2023Document6 pagesJD OccupationalHealthandSafetyAdviser September2023Stanley Yakic BasaweNo ratings yet
- Looking For Higher Standards: Behavioural Safety - Improving PerformanceDocument16 pagesLooking For Higher Standards: Behavioural Safety - Improving PerformanceHelp Tubestar Crew100% (1)
- Advanced Safety ManagementDocument2 pagesAdvanced Safety ManagementziyadeliNo ratings yet
- PSM 6 - Element 1 - Process Safety Culture (v3)Document29 pagesPSM 6 - Element 1 - Process Safety Culture (v3)Ahmed Hamad100% (1)
- Management & SafetyDocument25 pagesManagement & SafetyJawad Ahmad Bin KhanNo ratings yet
- Risk Management WFPDocument132 pagesRisk Management WFPBibek BaralNo ratings yet
- NAHQ Industry Insights - RLDatix Provider ManagementDocument43 pagesNAHQ Industry Insights - RLDatix Provider ManagementHEBA ALSHAIBINo ratings yet
- 2.6 BBS Overview BrochureDocument3 pages2.6 BBS Overview BrochureherikNo ratings yet
- Unit 1: Worker Safety and Safety Culture - An IntroductionDocument64 pagesUnit 1: Worker Safety and Safety Culture - An IntroductionBukenya RaymondNo ratings yet
- Corporate H&S StrategyDocument4 pagesCorporate H&S StrategyEmad ElshaerNo ratings yet
- Guideline SmsDocument15 pagesGuideline SmsEdison IANo ratings yet
- What Is Safety CultureDocument59 pagesWhat Is Safety Culturesjarvis5100% (5)
- BEHAVIOUR BASED SAFETY GUIDE.pdfDocument24 pagesBEHAVIOUR BASED SAFETY GUIDE.pdfAbdallah AbdallahNo ratings yet
- Tantangan K3RS Yang Mendukung Mutu & Keselamatan Di FanyankesDocument28 pagesTantangan K3RS Yang Mendukung Mutu & Keselamatan Di FanyankesAngela PuspitaNo ratings yet
- BHGN 3: Keperibadian Dan KetrampilanDocument7 pagesBHGN 3: Keperibadian Dan KetrampilanSakinah Mhd ShukreeNo ratings yet
- Chapter 11Document2 pagesChapter 11fzubairisaabNo ratings yet
- Duties of Safety OfficerDocument5 pagesDuties of Safety Officerjio4g1941No ratings yet
- Seven Leading Indicators To Drive Safety Improvement in Your OrganizationDocument16 pagesSeven Leading Indicators To Drive Safety Improvement in Your OrganizationKimberly ConleyNo ratings yet
- Improving Safety Cultures Manchester Branch 11 March 2014Document23 pagesImproving Safety Cultures Manchester Branch 11 March 2014Bobby Sharon100% (1)
- Behavior OptimizationDocument13 pagesBehavior OptimizationDUCE FUHRERNo ratings yet
- Day 1 M11 OOS 2018Document118 pagesDay 1 M11 OOS 2018AbdulslamNo ratings yet
- Safety CultureDocument20 pagesSafety Cultureali_1987No ratings yet
- Chapter 3-Using Structure CommunicationDocument21 pagesChapter 3-Using Structure CommunicationSafiyaPiroNo ratings yet
- CEP2010 Heat TransferDocument8 pagesCEP2010 Heat TransferamsukdNo ratings yet
- Ca en Government Vaccine Mandate Aoda v2Document16 pagesCa en Government Vaccine Mandate Aoda v2GlowstarNo ratings yet
- Membangun Budaya Keselamatan Pasien: Budi SampurnaDocument61 pagesMembangun Budaya Keselamatan Pasien: Budi SampurnaDkt TegalNo ratings yet
- Quality ImprovementDocument125 pagesQuality ImprovementNia SinghNo ratings yet
- ELEMENT 3 Managing Risk - Understanding People and Process1Document60 pagesELEMENT 3 Managing Risk - Understanding People and Process1asn qureshiNo ratings yet
- CER+Comfort+Family+Group+21 06Document46 pagesCER+Comfort+Family+Group+21 06ashwani niteshNo ratings yet
- VA IO EZ-IO-Clinical-Principles SHORTDocument21 pagesVA IO EZ-IO-Clinical-Principles SHORTMohammed HammedNo ratings yet
- Imdrf Meet 160913 Brazil Iso14155 2011Document23 pagesImdrf Meet 160913 Brazil Iso14155 2011Mohammed HammedNo ratings yet
- MDCG 2021-25 Legacy DevicesDocument11 pagesMDCG 2021-25 Legacy DevicesMohammed HammedNo ratings yet
- GHTF sg5 n3 Clinical Investigations 100212Document11 pagesGHTF sg5 n3 Clinical Investigations 100212Mohammed HammedNo ratings yet
- Celex 32023R0607 en TXTDocument6 pagesCelex 32023R0607 en TXTMohammed HammedNo ratings yet
- 3.1 Investigational Medical DeviceDocument4 pages3.1 Investigational Medical DeviceMohammed HammedNo ratings yet
- 4.1 Applicability of Section 4: Yes NoDocument2 pages4.1 Applicability of Section 4: Yes NoMohammed HammedNo ratings yet
- Development of Clinical Practice Guidelines For The NHSDocument24 pagesDevelopment of Clinical Practice Guidelines For The NHSMohammed HammedNo ratings yet
- Clinical Investigation - Application Form Under Medical Device RegulationDocument21 pagesClinical Investigation - Application Form Under Medical Device RegulationMohammed HammedNo ratings yet
- Clinical Outcomes With Newer Antihyperglycemic Agents: FDA-Mandated CV Safety TrialsDocument27 pagesClinical Outcomes With Newer Antihyperglycemic Agents: FDA-Mandated CV Safety TrialsMohammed HammedNo ratings yet
- 6 - USP Packaging Update StultsDocument26 pages6 - USP Packaging Update StultsMohammed HammedNo ratings yet
- Accuracy When Assessing and Evaluating Body Temperature in Clinical Practice: Time For A Change?Document8 pagesAccuracy When Assessing and Evaluating Body Temperature in Clinical Practice: Time For A Change?Mohammed HammedNo ratings yet
- Pharmacovigilance in Clinical Trials: Version 04 Feb 2021Document81 pagesPharmacovigilance in Clinical Trials: Version 04 Feb 2021Mohammed HammedNo ratings yet
- Burns Starting Clinical ResearchDocument16 pagesBurns Starting Clinical ResearchMohammed HammedNo ratings yet
- Clinical ValidationDocument39 pagesClinical ValidationMohammed HammedNo ratings yet
- JCG Clinical Trials 2016 V 3.5Document39 pagesJCG Clinical Trials 2016 V 3.5Mohammed HammedNo ratings yet
- 06 Prof Deborah Ashby ObeDocument54 pages06 Prof Deborah Ashby ObeMohammed HammedNo ratings yet
- Why Nih Clinical Research MattersDocument15 pagesWhy Nih Clinical Research MattersMohammed HammedNo ratings yet
- 10 1016-j Jaci 2012 01 063figureDocument12 pages10 1016-j Jaci 2012 01 063figureMohammed HammedNo ratings yet
- The Clinical Indemnity Scheme-National Clinical Incident Reporting SystemDocument23 pagesThe Clinical Indemnity Scheme-National Clinical Incident Reporting SystemMohammed HammedNo ratings yet
- Characteristics of Children With Learning DisabilitiesDocument4 pagesCharacteristics of Children With Learning DisabilitiesDanilo Siquig Jr.No ratings yet
- Phosphate COOLING TOWERS PDFDocument23 pagesPhosphate COOLING TOWERS PDFDaneyal BabarNo ratings yet
- RP 1 4Document10 pagesRP 1 4supervenienceNo ratings yet
- Prince CVDocument2 pagesPrince CVporosh.ezio420No ratings yet
- ENEE 624 Advanced Digital Signal Processing Problem Set 2 SolutionsDocument10 pagesENEE 624 Advanced Digital Signal Processing Problem Set 2 SolutionsstephanNo ratings yet
- PWL5650 Encore LT Manual Powder Spray System enDocument4 pagesPWL5650 Encore LT Manual Powder Spray System enHaendel RamirezNo ratings yet
- American Anthropological Association, Wiley American EthnologistDocument4 pagesAmerican Anthropological Association, Wiley American Ethnologistbolontiku9No ratings yet
- PAPER Employees Performance Appraisal of Chettinad Cement GulbargaDocument11 pagesPAPER Employees Performance Appraisal of Chettinad Cement GulbargaDr Bhadrappa HaralayyaNo ratings yet
- Streamlines: Streamlines Dialog Box, Providing The Results Contain Flow ResultsDocument2 pagesStreamlines: Streamlines Dialog Box, Providing The Results Contain Flow ResultsManuel LavinNo ratings yet
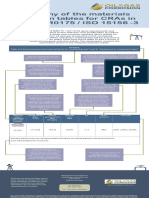
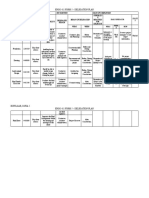
- Anatomy of The Materials Selection Tables For Cras in Nace Mr0175 / Iso 15156 - 3Document1 pageAnatomy of The Materials Selection Tables For Cras in Nace Mr0175 / Iso 15156 - 3MahsaNo ratings yet
- Project ProposalDocument5 pagesProject ProposalSarmast Bilawal Khuhro0% (1)
- English: Quarter 4 - Module 6Document14 pagesEnglish: Quarter 4 - Module 6Belle RomeroNo ratings yet
- Ingestable Robots: Presented By: Rakesh C N IV Sem McaDocument12 pagesIngestable Robots: Presented By: Rakesh C N IV Sem McaRamesh kNo ratings yet
- Principles of SpeechwritingDocument10 pagesPrinciples of SpeechwritingMarc Riomalos58% (12)
- Engg 411 Form 5 Delegation PlanDocument2 pagesEngg 411 Form 5 Delegation PlanSofiaJabadanEspulgarNo ratings yet
- Diagnostic Test All Subjects - Docx Version 1Document22 pagesDiagnostic Test All Subjects - Docx Version 1Junelle Joy CatbaganNo ratings yet
- Asteriods, Meteriods and CometDocument13 pagesAsteriods, Meteriods and CometTin BaynosaNo ratings yet
- LIFELONG-LEARNING - Da CheckDocument2 pagesLIFELONG-LEARNING - Da CheckHoàng Minh HồngNo ratings yet
- Makalah Bahasa InggrisDocument6 pagesMakalah Bahasa InggrisFatur RahmNNo ratings yet
- Datasheet-Sandvik-9ru10-En-V2021-08-16 09 - 55 Version 1Document5 pagesDatasheet-Sandvik-9ru10-En-V2021-08-16 09 - 55 Version 1aceinsteinNo ratings yet
- 1b. NIST - GCR.16-917-40 (SMRF 2nd Ed) 1Document23 pages1b. NIST - GCR.16-917-40 (SMRF 2nd Ed) 1Ismail HasanNo ratings yet
- Biomass Gasifier Using CDFDocument71 pagesBiomass Gasifier Using CDFarnalt_stalinNo ratings yet
- Practice-Tasks IxDocument6 pagesPractice-Tasks IxRidwan IslamNo ratings yet
- Kasmaji Techical Specifications - ENDocument3 pagesKasmaji Techical Specifications - ENrolandianurNo ratings yet
- A Tractable Probabilistic Approach To Analyze Sybil Attacks in Sharding-Based Blockchain ProtocolsDocument11 pagesA Tractable Probabilistic Approach To Analyze Sybil Attacks in Sharding-Based Blockchain Protocolsdileepbaby111No ratings yet
- Invitation EnglishDocument10 pagesInvitation EnglishHariz HabibiNo ratings yet
- Art Star Program Dream Plan Template: CG HobbyistDocument12 pagesArt Star Program Dream Plan Template: CG HobbyistDinda RachelNo ratings yet
- 16.time Table - Pratham (All Phases) - 2024-25Document1 page16.time Table - Pratham (All Phases) - 2024-25kcshreyas453No ratings yet