You might also like
- 057608komatsu Hydraulic Oil HO 46-HMDocument5 pages057608komatsu Hydraulic Oil HO 46-HMrolex21No ratings yet
- Drug Compliance Among Hypertensive PatientsDocument5 pagesDrug Compliance Among Hypertensive PatientsSyifa MunawarahNo ratings yet
- 2013 Sepsis GuidelinesDocument58 pages2013 Sepsis GuidelinesMuhd Azam100% (1)
- HK I 05 Set A Cleaning CaddyDocument10 pagesHK I 05 Set A Cleaning CaddysamismithNo ratings yet
- Techniques To Improve Intradialytic Haemodynamic Stability: ReviewDocument7 pagesTechniques To Improve Intradialytic Haemodynamic Stability: Reviewnelbut2No ratings yet
- Acute Hemodialysis PrescriptionDocument18 pagesAcute Hemodialysis PrescriptionOlga Babii100% (1)
- Cherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyDocument10 pagesCherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyShareDialysisNo ratings yet
- Football Emergency Medicine Manual 2 EditionDocument152 pagesFootball Emergency Medicine Manual 2 EditionNicolás Alvarez VidelaNo ratings yet
- Acute Hemodialysis PrescriptionDocument13 pagesAcute Hemodialysis PrescriptionR DNo ratings yet
- Evaluation and Management of Suspected Sepsis and Septic Shock in Adults - UpToDateDocument37 pagesEvaluation and Management of Suspected Sepsis and Septic Shock in Adults - UpToDatebarcanbiancaNo ratings yet
- Report2014 PDFDocument332 pagesReport2014 PDFShareDialysis100% (1)
- Ebp Formative Synthesis PaperDocument9 pagesEbp Formative Synthesis Paperapi-404415990No ratings yet
- 2021 AHA:ACC:ASE:CHEST:SAEM:SCCT:SCMR Guideline For The Evaluation and Diagnosis of Chest PainDocument87 pages2021 AHA:ACC:ASE:CHEST:SAEM:SCCT:SCMR Guideline For The Evaluation and Diagnosis of Chest PainFábioOliveiraNo ratings yet
- Part A5 District HospitalDocument119 pagesPart A5 District Hospitalreddi.demullu007No ratings yet
- Crash Cart Policy and Checklist in HospitalDocument7 pagesCrash Cart Policy and Checklist in HospitalDnyanesh AitalwadNo ratings yet
- Principles of Fluid Management 2015 PDFDocument17 pagesPrinciples of Fluid Management 2015 PDFJorge DíazNo ratings yet
- Pleural Fluid AnalysisDocument15 pagesPleural Fluid AnalysisNatalie Sarah MoonNo ratings yet
- Evidence Paper JpeacottricardosDocument7 pagesEvidence Paper Jpeacottricardosapi-302415380No ratings yet
- Understanding Your Hemodialysis Options EngDocument16 pagesUnderstanding Your Hemodialysis Options EngKavidu KeshanNo ratings yet
- Geriatric 602 FinalDocument5 pagesGeriatric 602 FinalLhen-Vincelyn LeysonNo ratings yet
- CV TEMPLATE Specialist DenmarkDocument8 pagesCV TEMPLATE Specialist DenmarkElena DumitriuNo ratings yet
- Blood Transfusion On Dialysis Guidelines Aug 2017 PDFDocument5 pagesBlood Transfusion On Dialysis Guidelines Aug 2017 PDFYolanda IrawatiNo ratings yet
- RXPG Series-Preventive and Social Medicine BUSTER (2004) (PDF) (UnitedVRG)Document156 pagesRXPG Series-Preventive and Social Medicine BUSTER (2004) (PDF) (UnitedVRG)Dr PNo ratings yet
- Technologies Designed To Help Improve Patients OutcomeDocument53 pagesTechnologies Designed To Help Improve Patients OutcomeHarby Ongbay AbellanosaNo ratings yet
- Makalah HypertensionDocument6 pagesMakalah HypertensionFatin ZafirahNo ratings yet
- ABC of Wound Healing PDFDocument4 pagesABC of Wound Healing PDFMrJPhaetonNo ratings yet
- National Health Policy 2009 PakistanDocument38 pagesNational Health Policy 2009 PakistanAbdul Wahab KhanNo ratings yet
- Diabetic Nephropathy: Assisstant Professor Dr. Mihaela-Dora DonciuDocument65 pagesDiabetic Nephropathy: Assisstant Professor Dr. Mihaela-Dora DonciuFloreaAndreiNo ratings yet
- Case Study Hypertension - EditedDocument8 pagesCase Study Hypertension - EditedJayReneNo ratings yet
- Blood Transfusio ChecklistDocument6 pagesBlood Transfusio ChecklistJLea OchiaNo ratings yet
- Novena To St. Expeditus: Mention The Particular Need Desired)Document2 pagesNovena To St. Expeditus: Mention The Particular Need Desired)Pierre TeoNo ratings yet
- Physiology & ApplicationsDocument52 pagesPhysiology & ApplicationsYuliyanti YasinNo ratings yet
- Descriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Document47 pagesDescriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Nina100% (1)
- Dialysis Dose Prescription: Presented by Dr. UjjawalDocument54 pagesDialysis Dose Prescription: Presented by Dr. UjjawalZH. omg sarNo ratings yet
- Summative 2 Renal 2011Document8 pagesSummative 2 Renal 2011Ike Annisa YuwelzaNo ratings yet
- Part A1 Sub CentresDocument75 pagesPart A1 Sub CentresPratheeka ShettyNo ratings yet
- Hemodiafiltration KuhlmannDocument31 pagesHemodiafiltration Kuhlmanntigercat100% (1)
- Overview of Heavy Proteinuria and The Nephrotic Syndrome - UpToDateDocument34 pagesOverview of Heavy Proteinuria and The Nephrotic Syndrome - UpToDatechristian47No ratings yet
- Blood Transfusion Therapy DefinitionDocument27 pagesBlood Transfusion Therapy DefinitionEvangelin MelvinNo ratings yet
- Tubulointerstitial Diseases: Dr. Raid JastaniaDocument48 pagesTubulointerstitial Diseases: Dr. Raid JastaniaThomas McconnellNo ratings yet
- Overview of The Management of Acute Kidney Injury in Adults - UpToDateDocument13 pagesOverview of The Management of Acute Kidney Injury in Adults - UpToDateDaniely FreitasNo ratings yet
- Renal Replacement Therapy HD, PD, Renal TransplantationDocument65 pagesRenal Replacement Therapy HD, PD, Renal TransplantationparciNo ratings yet
- Primer On Clinical Acid-Base Problem Solving - DisAMon 2004Document41 pagesPrimer On Clinical Acid-Base Problem Solving - DisAMon 2004Ashley100% (1)
- 10.08.07 Cardiac Tamponade HaagDocument16 pages10.08.07 Cardiac Tamponade HaagfoetorNo ratings yet
- Part A2 Primary Health Centres PDFDocument97 pagesPart A2 Primary Health Centres PDFSONNENo ratings yet
- Healthpolicy Brief Cervical Cancer Screening PhilippinesDocument13 pagesHealthpolicy Brief Cervical Cancer Screening PhilippinesIya JoyNo ratings yet
- Infection Prevention and Control Annual Report 2012-13 V 3 PDFDocument22 pagesInfection Prevention and Control Annual Report 2012-13 V 3 PDFTianti PuadiNo ratings yet
- Guidelines For Sedation and Anesthesia in GI Endos PDFDocument11 pagesGuidelines For Sedation and Anesthesia in GI Endos PDFHernan RuedaNo ratings yet
- Renal Failure PresentationDocument65 pagesRenal Failure PresentationBhawna Joshi100% (1)
- Outpt. Recommendation of Renal Transplant Patients.Document86 pagesOutpt. Recommendation of Renal Transplant Patients.Nephrology On-DemandNo ratings yet
- Meningitis - Practice Essentials, Background, PathophysiologyDocument26 pagesMeningitis - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- Pediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIDocument27 pagesPediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIAfied Fitrah100% (1)
- Development of A Self-Report Instrument To Measure Patient Safety Attitudes, Skills, and KnowledgeDocument5 pagesDevelopment of A Self-Report Instrument To Measure Patient Safety Attitudes, Skills, and KnowledgeEko Wahyu AgustinNo ratings yet
- Ethical Challenges of Organ Transplantation: Current Debates and International PerspectivesFrom EverandEthical Challenges of Organ Transplantation: Current Debates and International PerspectivesSolveig Lena HansenNo ratings yet
- Blood Transfusion Services in Sub Saharan Africa: Challenges and ConstraintsFrom EverandBlood Transfusion Services in Sub Saharan Africa: Challenges and ConstraintsNo ratings yet
- A Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesFrom EverandA Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesJamalul Azizi Abdul RahamanNo ratings yet
- Healthcare Environmental Services A Complete Guide - 2020 EditionFrom EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Lab Report For ParacetamolDocument5 pagesLab Report For Paracetamol9gcfz8zf9xNo ratings yet
- Brain Workshop - a Dual N-Back game - نسخةDocument4 pagesBrain Workshop - a Dual N-Back game - نسخةBTQNo ratings yet
- Masterclass in MatchaDocument39 pagesMasterclass in MatchatomasiskoNo ratings yet
- Benefits of Hypnosis Author Mental Health America of Northern KentuckyDocument4 pagesBenefits of Hypnosis Author Mental Health America of Northern KentuckyJakarta SelamatNo ratings yet
- ACTIVITY Psychological First Aid PFADocument25 pagesACTIVITY Psychological First Aid PFAChristine DianeNo ratings yet
- Chun-Hung Chen Kun-Cheng ChouDocument38 pagesChun-Hung Chen Kun-Cheng ChoutwnationNo ratings yet
- 10besar Kode PenyakitDocument5 pages10besar Kode PenyakitDEWINo ratings yet
- INDROMATIC LeafletDocument2 pagesINDROMATIC LeafletRabindra SinghNo ratings yet
- Prevention & Management of Sports Injuries: Quimcy Dsouza Fybms-Sm (B) 75Document26 pagesPrevention & Management of Sports Injuries: Quimcy Dsouza Fybms-Sm (B) 75Quimcy100% (1)
- An Appraisal On Occlusal Philosophies in Full-Mouth Rehabilitation A Literature ReviewDocument4 pagesAn Appraisal On Occlusal Philosophies in Full-Mouth Rehabilitation A Literature ReviewaggrolNo ratings yet
- 5X5 Intermediate - Bill StarrDocument7 pages5X5 Intermediate - Bill StarrAfrican MastiffNo ratings yet
- The Effects of Trauma and How To Deal With It Jim BanksDocument5 pagesThe Effects of Trauma and How To Deal With It Jim Banks2bug2me2not2No ratings yet
- Main AmbaniDocument28 pagesMain AmbaniankursagarNo ratings yet
- IELTS Cause-Problem and Effect-Solution Model EssayDocument17 pagesIELTS Cause-Problem and Effect-Solution Model EssaySayaf RashadNo ratings yet
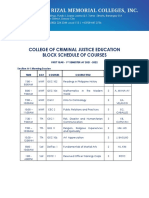
- College of Criminal Justice Education Block Schedule of CoursesDocument12 pagesCollege of Criminal Justice Education Block Schedule of CoursesKristel Ann ManlangitNo ratings yet
- Clamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)Document5 pagesClamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)rizwan900No ratings yet
- EthicsDocument10 pagesEthicsMadhubala JNo ratings yet
- Microbial PathogenesisDocument8 pagesMicrobial PathogenesisRachelleNo ratings yet
- S M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationDocument6 pagesS M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationLindsay JonesNo ratings yet
- HOLANDA ALEX CFE103 Module4 ContextEngageActivitiesDocument4 pagesHOLANDA ALEX CFE103 Module4 ContextEngageActivitiesAsus LaptopNo ratings yet
- Ultrarunning MagDocument60 pagesUltrarunning MagLynseyNo ratings yet
- JSP 403 Vol 2 Chapter 2Document61 pagesJSP 403 Vol 2 Chapter 2SOOD ASSOCIATES GOANo ratings yet
- Speed ManagementDocument284 pagesSpeed ManagementAdel AhmedNo ratings yet
- A Study of Work Life Balance of Female Employee With Refrence To HDFC Bank at MoradabadDocument72 pagesA Study of Work Life Balance of Female Employee With Refrence To HDFC Bank at MoradabadbuddysmbdNo ratings yet
- Manual CabinaDocument20 pagesManual CabinaCintexNo ratings yet
- Condylar Fracture: Muhammad Tahoor D17015Document36 pagesCondylar Fracture: Muhammad Tahoor D17015Umair KhalidNo ratings yet
- Lec 1disorders of Vascular Flow and ShockDocument91 pagesLec 1disorders of Vascular Flow and ShockMohid AhmedNo ratings yet
- 12.2 - Regulation of Body TemperatureDocument38 pages12.2 - Regulation of Body Temperature022797SemelllNo ratings yet