
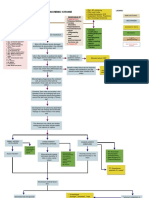
Indications of ICU Admission and ICU Management of COVID 19 NEW
Indications of ICU Admission and ICU Management of COVID 19 NEW
You might also like
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Picosure-CRG-921-7012-000rev7 - May 2015Document54 pagesPicosure-CRG-921-7012-000rev7 - May 2015Serenity Zhang100% (2)
- Anesthaesia and Intensive CareDocument139 pagesAnesthaesia and Intensive CareIvan Kurniadi100% (2)
- IAPD20 Virtual Abstract Book CompressedDocument991 pagesIAPD20 Virtual Abstract Book CompressedAnonymous NqTjEcNo ratings yet
- Sepsis - 3Document36 pagesSepsis - 3Mohd Ekhwan DarusNo ratings yet
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocument139 pagesAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (2)
- Clinical Evaluation Test Result Trends: DiagnosisDocument3 pagesClinical Evaluation Test Result Trends: DiagnosisStephen CrossNo ratings yet
- Severe Sepsis and Septic ShockDocument39 pagesSevere Sepsis and Septic ShockYogi Agil MurdjitoNo ratings yet
- EMRA Sepsis CardDocument4 pagesEMRA Sepsis Cardsgod34100% (1)
- Intensive Care Unit (ICU) Manual 2020-21Document146 pagesIntensive Care Unit (ICU) Manual 2020-21anithaNo ratings yet
- Surviving Sepsis GuidelinesDocument17 pagesSurviving Sepsis GuidelinesNabil RohaizatNo ratings yet
- SS Improving Patient OutcomesDocument11 pagesSS Improving Patient OutcomesspartacuslivesNo ratings yet
- TreatmentDocument55 pagesTreatmentderarataye6No ratings yet
- Management of SepsisDocument34 pagesManagement of SepsisTamim IshtiaqueNo ratings yet
- Current Recommendations For The Management of Severe Sepsis & Septic ShockDocument34 pagesCurrent Recommendations For The Management of Severe Sepsis & Septic ShockAmit KochetaNo ratings yet
- Blood Transfusion: By: Dr. Hira HanifDocument51 pagesBlood Transfusion: By: Dr. Hira HanifTariq sattarNo ratings yet
- Internal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiDocument209 pagesInternal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiSilvi Qiro'atul AiniNo ratings yet
- Sepsis Nursing Management in Emergency Care: By: Diah Retno Wulan, S.Kep., NS., M.KepDocument23 pagesSepsis Nursing Management in Emergency Care: By: Diah Retno Wulan, S.Kep., NS., M.KepTia AFNo ratings yet
- Upper GI BleedDocument8 pagesUpper GI BleedbbyesNo ratings yet
- Sepsis Guidelines PocketDocument2 pagesSepsis Guidelines Pocket陳悅生No ratings yet
- Sepsis and SIRSDocument24 pagesSepsis and SIRSFryda 'buona' YantiNo ratings yet
- Cme: Sirs and Modsfinal 3Document26 pagesCme: Sirs and Modsfinal 3asraf amirullahNo ratings yet
- Sepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashaDocument38 pagesSepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashapashaNo ratings yet
- Management of Patients With Vascular Disorders: Venous ArterialDocument56 pagesManagement of Patients With Vascular Disorders: Venous ArterialHamss AhmedNo ratings yet
- VTEDocument45 pagesVTEABREHAM BUKULONo ratings yet
- Severe Sepsis and Septic ShockDocument47 pagesSevere Sepsis and Septic Shocksembakarani thevagumaranNo ratings yet
- Day 1 Biomedis UAP Sepsis - MontoyaDocument45 pagesDay 1 Biomedis UAP Sepsis - MontoyaRye CalderonNo ratings yet
- Adverse Effects of Blood TransfusionsDocument3 pagesAdverse Effects of Blood Transfusionsay254No ratings yet
- Sepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMDocument3 pagesSepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMAli AftabNo ratings yet
- Sepsis Management: Runal Shah 1 Year Resident MEM, Kdah, MumbaiDocument18 pagesSepsis Management: Runal Shah 1 Year Resident MEM, Kdah, Mumbaibotet_2306No ratings yet
- Critical Care 123Document66 pagesCritical Care 123Mr.ShazNo ratings yet
- Sepsis & Septic Shock: Case Studies in Therapeutics (Iv)Document23 pagesSepsis & Septic Shock: Case Studies in Therapeutics (Iv)Dima MasadehNo ratings yet
- Sepsis Dan Egdt: Dr. Muhammad Ilhamul Karim Dr. Deny Budiman HDocument34 pagesSepsis Dan Egdt: Dr. Muhammad Ilhamul Karim Dr. Deny Budiman HAkhmad MustafaNo ratings yet
- Abinash em Gi SurDocument72 pagesAbinash em Gi Sursapkota18No ratings yet
- Chapter 3: Perioperative ManagementDocument14 pagesChapter 3: Perioperative ManagementpoddataNo ratings yet
- An Introduction To Surgical Icu.: by DR Farrukh SaeedDocument33 pagesAn Introduction To Surgical Icu.: by DR Farrukh SaeedTARIQNo ratings yet
- DR Ahmed. Intensive Care Unit Book Important PointsDocument11 pagesDR Ahmed. Intensive Care Unit Book Important Pointsphilipswright74No ratings yet
- Sepsis Presentation 08-2010Document28 pagesSepsis Presentation 08-2010Karen Ann AloeNo ratings yet
- Management of Severe Malaria: Paul N HarijantoDocument56 pagesManagement of Severe Malaria: Paul N HarijantoDaniel MatiusNo ratings yet
- Early Goal Directed Theraphy2Document16 pagesEarly Goal Directed Theraphy2Taufiek HikmawanNo ratings yet
- Harrison's Hour - Sepsis Bundle 2016Document5 pagesHarrison's Hour - Sepsis Bundle 2016Bobet Reña100% (1)
- Septic Shock TreatmentDocument22 pagesSeptic Shock TreatmentAdreiTheTripleA100% (1)
- EGDTDocument33 pagesEGDTaLineLanNo ratings yet
- Git BleedingDocument28 pagesGit Bleedingsembakarani thevagumaranNo ratings yet
- Pulmonary EmbolismDocument70 pagesPulmonary Embolismalhindhy.gNo ratings yet
- SepsisDocument55 pagesSepsisAli SohailNo ratings yet
- Sepsis: Pathophysiology and Management in The ICU: Moderator: DR Kavita Rani Sharma Presenter: Dr. PrashanthDocument38 pagesSepsis: Pathophysiology and Management in The ICU: Moderator: DR Kavita Rani Sharma Presenter: Dr. Prashanthprashsubbu100% (1)
- Sir ClanDocument109 pagesSir ClanJames AbendanNo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- MalariaDocument5 pagesMalariaMo MonuNo ratings yet
- Tugas DR Yoma AncaDocument30 pagesTugas DR Yoma Ancaaby mayuNo ratings yet
- IV FluidDocument28 pagesIV FluidZulfkar Latief QadrieNo ratings yet
- Surviving Sepsis: Early Goal Directed TherapyDocument32 pagesSurviving Sepsis: Early Goal Directed Therapydr.mahensNo ratings yet
- Treatment Approach Considerations: Pericardial SclerosisDocument7 pagesTreatment Approach Considerations: Pericardial SclerosisDikie MustofadijayaNo ratings yet
- Revalida 1Document3 pagesRevalida 1herrabiel solisNo ratings yet
- Consider Abdominal Compartment Syndrome in Patients With Refractory HypotensionDocument26 pagesConsider Abdominal Compartment Syndrome in Patients With Refractory HypotensionHari AdityonugrohoNo ratings yet
- Sepsis, Sirs and ModsDocument4 pagesSepsis, Sirs and ModsMayra Alejandra Prada SerranoNo ratings yet
- Referat Sepsis Dan ARDS - Lea SichiliaDocument24 pagesReferat Sepsis Dan ARDS - Lea SichiliaLea SichiliaNo ratings yet
- MNI SAH ProtocolDocument10 pagesMNI SAH ProtocolAbo ZakariaNo ratings yet
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2No ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Cardiopulmonary ResuscitationDocument10 pagesCardiopulmonary ResuscitationLilay MakulayNo ratings yet
- MNT Case StudyDocument13 pagesMNT Case Studyapi-384503305No ratings yet
- SunburnsDocument3 pagesSunburnsCameron YoungNo ratings yet
- Physical Examination of The 4 Genitourinary TractDocument12 pagesPhysical Examination of The 4 Genitourinary TractrudybisNo ratings yet
- Molecular Prevalence of Pulmonary Tuberculosis in Prisons: Case of The Central Prison of FrancevilleDocument8 pagesMolecular Prevalence of Pulmonary Tuberculosis in Prisons: Case of The Central Prison of FrancevilleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CeftriaxoneDocument2 pagesCeftriaxonegaatgaatNo ratings yet
- HOPE NotesDocument6 pagesHOPE Notesayaka kamisatoNo ratings yet
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDocument13 pagesTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNo ratings yet
- Health Education On HypertentionDocument13 pagesHealth Education On HypertentionParth VasaveNo ratings yet
- Natural Abortion MethodsDocument10 pagesNatural Abortion MethodsSury Ganesh100% (1)
- 2014-15 Department Annual ReportDocument9 pages2014-15 Department Annual ReportPramodNo ratings yet
- NP2Document20 pagesNP2Anonymous hDcvpptNo ratings yet
- Guidelines Mediclaim L&TDocument5 pagesGuidelines Mediclaim L&Tnidnitrkl051296No ratings yet
- CBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsDocument5 pagesCBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsSatvik MishraNo ratings yet
- Working in Lap of Corona Virus Disease (Covid - 19) at HMCH Hazaribagh JharkhandDocument3 pagesWorking in Lap of Corona Virus Disease (Covid - 19) at HMCH Hazaribagh JharkhandBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Practical PharmacologyhjhjhDocument9 pagesPractical PharmacologyhjhjhMonzer AchtarNo ratings yet
- Guder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine EnglishDocument41 pagesGuder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine Englishrild278111100% (1)
- Endocrine Part 2 DRAFTDocument6 pagesEndocrine Part 2 DRAFTPreeti Joan BuxaniNo ratings yet
- PharmacogeneticsDocument18 pagesPharmacogeneticsHafsah ShoaibNo ratings yet
- Introduction To Abnormal Psychology Boundless PsychologyDocument17 pagesIntroduction To Abnormal Psychology Boundless PsychologySana NasirNo ratings yet
- Sickle Cell AnaemiaDocument10 pagesSickle Cell AnaemiaAhmadNo ratings yet
- Quick Sleep Tips For Truck DriversDocument2 pagesQuick Sleep Tips For Truck DriversBaye HickinsNo ratings yet
- Renal Pathology Unit ExamDocument50 pagesRenal Pathology Unit ExamCherry RahimaNo ratings yet
- Leaky Gut in AutismDocument18 pagesLeaky Gut in AutismAdinda RaihanaNo ratings yet
- David Jockers Symptomatic Digestive Relief GuideDocument24 pagesDavid Jockers Symptomatic Digestive Relief GuideConfidentro BlospotNo ratings yet
- D.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Document6 pagesD.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Dr-Sanjay SinghaniaNo ratings yet























































































Download as pptx, pdf, or txt
You might also like
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Picosure-CRG-921-7012-000rev7 - May 2015Document54 pagesPicosure-CRG-921-7012-000rev7 - May 2015Serenity Zhang100% (2)
- Anesthaesia and Intensive CareDocument139 pagesAnesthaesia and Intensive CareIvan Kurniadi100% (2)
- IAPD20 Virtual Abstract Book CompressedDocument991 pagesIAPD20 Virtual Abstract Book CompressedAnonymous NqTjEcNo ratings yet
- Sepsis - 3Document36 pagesSepsis - 3Mohd Ekhwan DarusNo ratings yet
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocument139 pagesAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (2)
- Clinical Evaluation Test Result Trends: DiagnosisDocument3 pagesClinical Evaluation Test Result Trends: DiagnosisStephen CrossNo ratings yet
- Severe Sepsis and Septic ShockDocument39 pagesSevere Sepsis and Septic ShockYogi Agil MurdjitoNo ratings yet
- EMRA Sepsis CardDocument4 pagesEMRA Sepsis Cardsgod34100% (1)
- Intensive Care Unit (ICU) Manual 2020-21Document146 pagesIntensive Care Unit (ICU) Manual 2020-21anithaNo ratings yet
- Surviving Sepsis GuidelinesDocument17 pagesSurviving Sepsis GuidelinesNabil RohaizatNo ratings yet
- SS Improving Patient OutcomesDocument11 pagesSS Improving Patient OutcomesspartacuslivesNo ratings yet
- TreatmentDocument55 pagesTreatmentderarataye6No ratings yet
- Management of SepsisDocument34 pagesManagement of SepsisTamim IshtiaqueNo ratings yet
- Current Recommendations For The Management of Severe Sepsis & Septic ShockDocument34 pagesCurrent Recommendations For The Management of Severe Sepsis & Septic ShockAmit KochetaNo ratings yet
- Blood Transfusion: By: Dr. Hira HanifDocument51 pagesBlood Transfusion: By: Dr. Hira HanifTariq sattarNo ratings yet
- Internal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiDocument209 pagesInternal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiSilvi Qiro'atul AiniNo ratings yet
- Sepsis Nursing Management in Emergency Care: By: Diah Retno Wulan, S.Kep., NS., M.KepDocument23 pagesSepsis Nursing Management in Emergency Care: By: Diah Retno Wulan, S.Kep., NS., M.KepTia AFNo ratings yet
- Upper GI BleedDocument8 pagesUpper GI BleedbbyesNo ratings yet
- Sepsis Guidelines PocketDocument2 pagesSepsis Guidelines Pocket陳悅生No ratings yet
- Sepsis and SIRSDocument24 pagesSepsis and SIRSFryda 'buona' YantiNo ratings yet
- Cme: Sirs and Modsfinal 3Document26 pagesCme: Sirs and Modsfinal 3asraf amirullahNo ratings yet
- Sepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashaDocument38 pagesSepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashapashaNo ratings yet
- Management of Patients With Vascular Disorders: Venous ArterialDocument56 pagesManagement of Patients With Vascular Disorders: Venous ArterialHamss AhmedNo ratings yet
- VTEDocument45 pagesVTEABREHAM BUKULONo ratings yet
- Severe Sepsis and Septic ShockDocument47 pagesSevere Sepsis and Septic Shocksembakarani thevagumaranNo ratings yet
- Day 1 Biomedis UAP Sepsis - MontoyaDocument45 pagesDay 1 Biomedis UAP Sepsis - MontoyaRye CalderonNo ratings yet
- Adverse Effects of Blood TransfusionsDocument3 pagesAdverse Effects of Blood Transfusionsay254No ratings yet
- Sepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMDocument3 pagesSepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMAli AftabNo ratings yet
- Sepsis Management: Runal Shah 1 Year Resident MEM, Kdah, MumbaiDocument18 pagesSepsis Management: Runal Shah 1 Year Resident MEM, Kdah, Mumbaibotet_2306No ratings yet
- Critical Care 123Document66 pagesCritical Care 123Mr.ShazNo ratings yet
- Sepsis & Septic Shock: Case Studies in Therapeutics (Iv)Document23 pagesSepsis & Septic Shock: Case Studies in Therapeutics (Iv)Dima MasadehNo ratings yet
- Sepsis Dan Egdt: Dr. Muhammad Ilhamul Karim Dr. Deny Budiman HDocument34 pagesSepsis Dan Egdt: Dr. Muhammad Ilhamul Karim Dr. Deny Budiman HAkhmad MustafaNo ratings yet
- Abinash em Gi SurDocument72 pagesAbinash em Gi Sursapkota18No ratings yet
- Chapter 3: Perioperative ManagementDocument14 pagesChapter 3: Perioperative ManagementpoddataNo ratings yet
- An Introduction To Surgical Icu.: by DR Farrukh SaeedDocument33 pagesAn Introduction To Surgical Icu.: by DR Farrukh SaeedTARIQNo ratings yet
- DR Ahmed. Intensive Care Unit Book Important PointsDocument11 pagesDR Ahmed. Intensive Care Unit Book Important Pointsphilipswright74No ratings yet
- Sepsis Presentation 08-2010Document28 pagesSepsis Presentation 08-2010Karen Ann AloeNo ratings yet
- Management of Severe Malaria: Paul N HarijantoDocument56 pagesManagement of Severe Malaria: Paul N HarijantoDaniel MatiusNo ratings yet
- Early Goal Directed Theraphy2Document16 pagesEarly Goal Directed Theraphy2Taufiek HikmawanNo ratings yet
- Harrison's Hour - Sepsis Bundle 2016Document5 pagesHarrison's Hour - Sepsis Bundle 2016Bobet Reña100% (1)
- Septic Shock TreatmentDocument22 pagesSeptic Shock TreatmentAdreiTheTripleA100% (1)
- EGDTDocument33 pagesEGDTaLineLanNo ratings yet
- Git BleedingDocument28 pagesGit Bleedingsembakarani thevagumaranNo ratings yet
- Pulmonary EmbolismDocument70 pagesPulmonary Embolismalhindhy.gNo ratings yet
- SepsisDocument55 pagesSepsisAli SohailNo ratings yet
- Sepsis: Pathophysiology and Management in The ICU: Moderator: DR Kavita Rani Sharma Presenter: Dr. PrashanthDocument38 pagesSepsis: Pathophysiology and Management in The ICU: Moderator: DR Kavita Rani Sharma Presenter: Dr. Prashanthprashsubbu100% (1)
- Sir ClanDocument109 pagesSir ClanJames AbendanNo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- MalariaDocument5 pagesMalariaMo MonuNo ratings yet
- Tugas DR Yoma AncaDocument30 pagesTugas DR Yoma Ancaaby mayuNo ratings yet
- IV FluidDocument28 pagesIV FluidZulfkar Latief QadrieNo ratings yet
- Surviving Sepsis: Early Goal Directed TherapyDocument32 pagesSurviving Sepsis: Early Goal Directed Therapydr.mahensNo ratings yet
- Treatment Approach Considerations: Pericardial SclerosisDocument7 pagesTreatment Approach Considerations: Pericardial SclerosisDikie MustofadijayaNo ratings yet
- Revalida 1Document3 pagesRevalida 1herrabiel solisNo ratings yet
- Consider Abdominal Compartment Syndrome in Patients With Refractory HypotensionDocument26 pagesConsider Abdominal Compartment Syndrome in Patients With Refractory HypotensionHari AdityonugrohoNo ratings yet
- Sepsis, Sirs and ModsDocument4 pagesSepsis, Sirs and ModsMayra Alejandra Prada SerranoNo ratings yet
- Referat Sepsis Dan ARDS - Lea SichiliaDocument24 pagesReferat Sepsis Dan ARDS - Lea SichiliaLea SichiliaNo ratings yet
- MNI SAH ProtocolDocument10 pagesMNI SAH ProtocolAbo ZakariaNo ratings yet
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2No ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Cardiopulmonary ResuscitationDocument10 pagesCardiopulmonary ResuscitationLilay MakulayNo ratings yet
- MNT Case StudyDocument13 pagesMNT Case Studyapi-384503305No ratings yet
- SunburnsDocument3 pagesSunburnsCameron YoungNo ratings yet
- Physical Examination of The 4 Genitourinary TractDocument12 pagesPhysical Examination of The 4 Genitourinary TractrudybisNo ratings yet
- Molecular Prevalence of Pulmonary Tuberculosis in Prisons: Case of The Central Prison of FrancevilleDocument8 pagesMolecular Prevalence of Pulmonary Tuberculosis in Prisons: Case of The Central Prison of FrancevilleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CeftriaxoneDocument2 pagesCeftriaxonegaatgaatNo ratings yet
- HOPE NotesDocument6 pagesHOPE Notesayaka kamisatoNo ratings yet
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDocument13 pagesTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNo ratings yet
- Health Education On HypertentionDocument13 pagesHealth Education On HypertentionParth VasaveNo ratings yet
- Natural Abortion MethodsDocument10 pagesNatural Abortion MethodsSury Ganesh100% (1)
- 2014-15 Department Annual ReportDocument9 pages2014-15 Department Annual ReportPramodNo ratings yet
- NP2Document20 pagesNP2Anonymous hDcvpptNo ratings yet
- Guidelines Mediclaim L&TDocument5 pagesGuidelines Mediclaim L&Tnidnitrkl051296No ratings yet
- CBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsDocument5 pagesCBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsSatvik MishraNo ratings yet
- Working in Lap of Corona Virus Disease (Covid - 19) at HMCH Hazaribagh JharkhandDocument3 pagesWorking in Lap of Corona Virus Disease (Covid - 19) at HMCH Hazaribagh JharkhandBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Practical PharmacologyhjhjhDocument9 pagesPractical PharmacologyhjhjhMonzer AchtarNo ratings yet
- Guder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine EnglishDocument41 pagesGuder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine Englishrild278111100% (1)
- Endocrine Part 2 DRAFTDocument6 pagesEndocrine Part 2 DRAFTPreeti Joan BuxaniNo ratings yet
- PharmacogeneticsDocument18 pagesPharmacogeneticsHafsah ShoaibNo ratings yet
- Introduction To Abnormal Psychology Boundless PsychologyDocument17 pagesIntroduction To Abnormal Psychology Boundless PsychologySana NasirNo ratings yet
- Sickle Cell AnaemiaDocument10 pagesSickle Cell AnaemiaAhmadNo ratings yet
- Quick Sleep Tips For Truck DriversDocument2 pagesQuick Sleep Tips For Truck DriversBaye HickinsNo ratings yet
- Renal Pathology Unit ExamDocument50 pagesRenal Pathology Unit ExamCherry RahimaNo ratings yet
- Leaky Gut in AutismDocument18 pagesLeaky Gut in AutismAdinda RaihanaNo ratings yet
- David Jockers Symptomatic Digestive Relief GuideDocument24 pagesDavid Jockers Symptomatic Digestive Relief GuideConfidentro BlospotNo ratings yet
- D.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Document6 pagesD.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Dr-Sanjay SinghaniaNo ratings yet