Download as ppt, pdf, or txt
You might also like
- 72 NamesOfGod For-MeditationDocument13 pages72 NamesOfGod For-MeditationLeonardo C.100% (5)
- Mother Earth by Chris ThomasDocument13 pagesMother Earth by Chris ThomasCoincidence Cafe100% (1)
- RE-sample MCQ For XQPDocument11 pagesRE-sample MCQ For XQPVenkadeshwaran KuthalingamNo ratings yet
- DOLE OSH Program TemplateDocument13 pagesDOLE OSH Program Templateoshc caraga100% (3)
- ASME - PTC4.1 .Boiler Efficiency TestDocument29 pagesASME - PTC4.1 .Boiler Efficiency TestBC Harish92% (13)
- Ebola Outbreak Analyzing The Data WorksheetDocument2 pagesEbola Outbreak Analyzing The Data Worksheetapi-262360890No ratings yet
- Tutopia Solutions - NEBOSH - DefinitionsDocument3 pagesTutopia Solutions - NEBOSH - DefinitionsElavarasan RamalingamNo ratings yet
- Human Reliability1Document27 pagesHuman Reliability1Chandramohan MuruganNo ratings yet
- Foundation For Safety Culture Improvement - in Pursuit of Safety ExcellenceDocument32 pagesFoundation For Safety Culture Improvement - in Pursuit of Safety Excellencearsaya100% (1)
- Chapter 4 - Hazard Identification, Risk Assessment Risk Control (HIRARC)Document39 pagesChapter 4 - Hazard Identification, Risk Assessment Risk Control (HIRARC)eyqinleeNo ratings yet
- Information To Suppliers On Vigilance - IndiaDocument7 pagesInformation To Suppliers On Vigilance - IndiaNix4crazyNo ratings yet
- TMP EFEADocument6 pagesTMP EFEAFrontiersNo ratings yet
- BDA Advice Sheet A11Document12 pagesBDA Advice Sheet A11soomro76134No ratings yet
- Iris Recognition TechnologyDocument14 pagesIris Recognition TechnologySathya KalaivananNo ratings yet
- SSLT Individual Assignment: Problem StatementDocument3 pagesSSLT Individual Assignment: Problem StatementParikshit MishraNo ratings yet
- Real-World Anomaly Detection in Surveillance VideosDocument10 pagesReal-World Anomaly Detection in Surveillance VideosSomya swarya naikNo ratings yet
- Tower Climbing SafetyDocument125 pagesTower Climbing Safetyakinola emmanuel100% (1)
- Topic C - PERSONAL PROTECTIVE EQUIPMENTDocument43 pagesTopic C - PERSONAL PROTECTIVE EQUIPMENTSn CarbonelNo ratings yet
- Automated PerimetryDocument16 pagesAutomated Perimetryyovis61722No ratings yet
- 1 s2.0 S2212671614001024 MainDocument6 pages1 s2.0 S2212671614001024 MainYaman MaximilienNo ratings yet
- 13T 160307 EU Asset IntegrityDocument13 pages13T 160307 EU Asset Integritykawtherhassan29No ratings yet
- JHADocument53 pagesJHASyed Mohd FirdausNo ratings yet
- Eurocontrol White Paperon Resilience EngineeringDocument17 pagesEurocontrol White Paperon Resilience EngineeringVikki KalilNo ratings yet
- Baseline Ohs Risk Assessment (Bra)Document8 pagesBaseline Ohs Risk Assessment (Bra)aceNo ratings yet
- Bbs Preventive ToolsDocument6 pagesBbs Preventive ToolsEmmanuelNo ratings yet
- SWMS2 Confined Space EntryDocument9 pagesSWMS2 Confined Space EntryIslam Sarhan100% (1)
- 0th ReviewDocument14 pages0th ReviewDhanshikaNo ratings yet
- MC 2019 EU-MDRSuccessfulPractices2Document59 pagesMC 2019 EU-MDRSuccessfulPractices2M. MARHANSYAHNo ratings yet
- 8 Process Safety Awareness PresentationDocument27 pages8 Process Safety Awareness PresentationVincent Magtibay67% (3)
- Overview of Condition Based MaintenanceDocument31 pagesOverview of Condition Based MaintenanceGisela Balderas100% (1)
- LSR Self Assessments Tool - Q3Document27 pagesLSR Self Assessments Tool - Q3RitikNo ratings yet
- OSH Program BAESA CHINISE DIMSUM & NOODLES HUBDocument13 pagesOSH Program BAESA CHINISE DIMSUM & NOODLES HUBArmando AballeNo ratings yet
- In-Ear EEG Biometrics For Feasible and Readily Collectable Real-World Person AuthenticationDocument14 pagesIn-Ear EEG Biometrics For Feasible and Readily Collectable Real-World Person AuthenticationTimothy AdeyemiNo ratings yet
- Bio Dimple VermaDocument7 pagesBio Dimple VermaNilesh SinghNo ratings yet
- Layer of Protection Analysis: SciencedirectDocument11 pagesLayer of Protection Analysis: SciencedirectDigitalMastersTXNo ratings yet
- Swarm Intelligence MODIFIEDDocument18 pagesSwarm Intelligence MODIFIEDAbid AnjumNo ratings yet
- NERC Application of Power Line CarrierDocument50 pagesNERC Application of Power Line Carrierschaefer1015719No ratings yet
- HSE Plan For Old ContractDocument72 pagesHSE Plan For Old ContractDURGAPRASAD JANYAVULANo ratings yet
- Task Risk Assessment FormDocument1 pageTask Risk Assessment Formmuhammadsuhaib100% (1)
- Cocu 5 - First Aid AdministrationDocument15 pagesCocu 5 - First Aid AdministrationIzzati SalbiyanaNo ratings yet
- Standards-Based Education 2009 - ULDocument20 pagesStandards-Based Education 2009 - ULdavid_diaz_sNo ratings yet
- Behavior Base SafetyDocument52 pagesBehavior Base SafetySheik AsarudeenNo ratings yet
- JSA-001 Earth Works & Civil WorksDocument5 pagesJSA-001 Earth Works & Civil WorksMoaatazz Nouisri50% (2)
- 03 1 Industrial Hygiene IntroductionDocument20 pages03 1 Industrial Hygiene IntroductionAstra BeckettNo ratings yet
- alarp_report_2024-03_02Document100 pagesalarp_report_2024-03_02Mohamed AchourNo ratings yet
- Lecture 7Document11 pagesLecture 7Ahmad AftabNo ratings yet
- Lec 4. Radiology WorkflowDocument24 pagesLec 4. Radiology Workflowallexa jimlaniNo ratings yet
- Occupational Safety and Health (OSH) Program Of: Sunrise Medical Lab, IncDocument11 pagesOccupational Safety and Health (OSH) Program Of: Sunrise Medical Lab, IncMarc SilvestreNo ratings yet
- A Presentation On Eyes Scanning: - Ujjawal - Soham - Anindita - Aditya - TuhinDocument15 pagesA Presentation On Eyes Scanning: - Ujjawal - Soham - Anindita - Aditya - TuhinAditya Bikram BhattacharjeeNo ratings yet
- Iris Recognition From Classic To Modern ApproachesDocument8 pagesIris Recognition From Classic To Modern ApproachesSathya KalaivananNo ratings yet
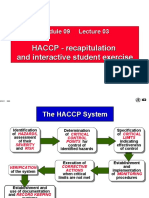
- HACCP - Recapitulation and Interactive Student ExerciseDocument7 pagesHACCP - Recapitulation and Interactive Student ExerciseMardha AzizahNo ratings yet
- Security Test Audit Report: True Protection Actual SecurityDocument9 pagesSecurity Test Audit Report: True Protection Actual SecurityJosé Ramón Pazos SánchezNo ratings yet
- Are You Doing The Right MaintenanceDocument5 pagesAre You Doing The Right Maintenancelrolindo100% (1)
- Information Security Attestation GuideDocument2 pagesInformation Security Attestation GuidePivot Point Security100% (1)
- TMP FFBCDocument7 pagesTMP FFBCFrontiersNo ratings yet
- ICAM Presentation1 ILversion 01.1Document112 pagesICAM Presentation1 ILversion 01.1redcutsaNo ratings yet
- Baseline Risk Assessment (Bra)Document8 pagesBaseline Risk Assessment (Bra)aceNo ratings yet
- Audit Checklist Process ApproachDocument131 pagesAudit Checklist Process ApproachEvaan KhanNo ratings yet
- Presentation Graduate ProgramDocument14 pagesPresentation Graduate Programzainab.alajmi99No ratings yet
- 07-Physical Protection TextDocument10 pages07-Physical Protection TextjoyitabiswasNo ratings yet
- Iris Recognition Technology: Implementation, Application, and Security ConsiderationDocument5 pagesIris Recognition Technology: Implementation, Application, and Security ConsiderationNitishSingh0095No ratings yet
- Prevent Hazardous Conditions From Causing Unsafe Incidents: Ecostruxure™ Triconex Emergency Shutdown SystemsDocument12 pagesPrevent Hazardous Conditions From Causing Unsafe Incidents: Ecostruxure™ Triconex Emergency Shutdown SystemsFederico BrigatoNo ratings yet
- Patient Safety Essentials ToolkitDocument47 pagesPatient Safety Essentials ToolkitHadiNo ratings yet
- SlessentialsDocument27 pagesSlessentialsHadiNo ratings yet
- Session 6 Slides - Mental Health SafetyDocument44 pagesSession 6 Slides - Mental Health SafetyHadiNo ratings yet
- Introduction To The Fundamentals of Teamstepps Concepts and Tools (Part 1 of 3)Document42 pagesIntroduction To The Fundamentals of Teamstepps Concepts and Tools (Part 1 of 3)HadiNo ratings yet
- Leadership Moments in Eliminating Preventable Harm Through High ReliabilityDocument18 pagesLeadership Moments in Eliminating Preventable Harm Through High ReliabilityHadiNo ratings yet
- Individual Application SPSC AWARD TEMPLATEDocument23 pagesIndividual Application SPSC AWARD TEMPLATEHadiNo ratings yet
- Activities CompletedDocument4 pagesActivities Completedウィリアムズ アンディNo ratings yet
- COVID Testing Labs 25122020Document151 pagesCOVID Testing Labs 25122020Seen Still AliveNo ratings yet
- Sabita Asphalt Manual Draft V10c 260814 PDFDocument93 pagesSabita Asphalt Manual Draft V10c 260814 PDFAshebirNo ratings yet
- Video 1Document9 pagesVideo 1Siti Hajar AjaNo ratings yet
- Distinction College-Application FormDocument2 pagesDistinction College-Application FormLiviesh AndersonNo ratings yet
- Characterization of Thermally Annealed PEEKDocument10 pagesCharacterization of Thermally Annealed PEEK高亚男No ratings yet
- API 570-Final Model Exam-Open Book Without AnswersDocument6 pagesAPI 570-Final Model Exam-Open Book Without Answersbanana100% (1)
- Fenomastic Pure Colours Enamel MattDocument4 pagesFenomastic Pure Colours Enamel MattAslam KhanNo ratings yet
- Chapter 5-Hydrology of Ungauged CatchmentsDocument18 pagesChapter 5-Hydrology of Ungauged CatchmentsMubarek AbduljebarNo ratings yet
- Code - Aster: "Exact" Elements of Beams (Right and Curved)Document68 pagesCode - Aster: "Exact" Elements of Beams (Right and Curved)Claudio Enrique Nuñez ReyesNo ratings yet
- APOLLO 13 Problem Solution & ManagementDocument7 pagesAPOLLO 13 Problem Solution & ManagementIke Sweesy88% (8)
- PHYSICS (Geometrical Optics) Set-2Document10 pagesPHYSICS (Geometrical Optics) Set-2malani.swastikNo ratings yet
- WWW - Studymaterialz.in: Signal and System Important 30 MCQ PDF With SolutionDocument71 pagesWWW - Studymaterialz.in: Signal and System Important 30 MCQ PDF With SolutionYash Gopani100% (1)
- Science EntranceDocument9 pagesScience EntrancechipendosalemNo ratings yet
- Envea Qal 260 Qal1 Back Scatter Particulate Emission Monitor enDocument4 pagesEnvea Qal 260 Qal1 Back Scatter Particulate Emission Monitor enRodrigo MeirelesNo ratings yet
- PrimeProbe3+ PPS-PP3-044-2.0Document18 pagesPrimeProbe3+ PPS-PP3-044-2.0Kishan ChandrasekaraNo ratings yet
- Textbook Modernism S Visible Hand Architecture and Regulation in America Michael Osman Ebook All Chapter PDFDocument53 pagesTextbook Modernism S Visible Hand Architecture and Regulation in America Michael Osman Ebook All Chapter PDFjames.myrick314100% (13)
- English 1-Q4-L18 ModuleDocument17 pagesEnglish 1-Q4-L18 ModuleJOSEPHINE CASINNo ratings yet
- Astm E855Document8 pagesAstm E855Hulisses MarconNo ratings yet
- Communication-Lesson 7Document36 pagesCommunication-Lesson 7maria bitarNo ratings yet
- Target Aiims: Pre-Medical: Chemistry AllenDocument24 pagesTarget Aiims: Pre-Medical: Chemistry Allenaleemhak100% (1)
- Tle G8-Epas Q1 M1 NewDocument29 pagesTle G8-Epas Q1 M1 NewAaron AnsaldoNo ratings yet
- How Is The Philippines Affected by Climate ChangeDocument2 pagesHow Is The Philippines Affected by Climate ChangeQueenie SantosNo ratings yet
- (T. Mandiri & T. Presentasi) (PerPan I C-TM4310) Genap 2021-2022Document2 pages(T. Mandiri & T. Presentasi) (PerPan I C-TM4310) Genap 2021-2022Ari Meliasta Ginting04No ratings yet
- International Journal of Information Technology, Control and Automation (IJITCA)Document2 pagesInternational Journal of Information Technology, Control and Automation (IJITCA)ijitcajournalNo ratings yet
- Swot Analysis: S W O TDocument17 pagesSwot Analysis: S W O TPratham TadasareNo ratings yet