Download as pptx, pdf, or txt
You might also like
- Wongs Essentials of Pediatric Nursing 9th Edition Hockenberry Test BankDocument3 pagesWongs Essentials of Pediatric Nursing 9th Edition Hockenberry Test Banka488625443100% (1)
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Iatrogenic Effects of Orthodontic TreatmentDocument29 pagesIatrogenic Effects of Orthodontic TreatmentKomal AsifNo ratings yet
- Written Examination GuideDocument17 pagesWritten Examination GuideIvanna H. A.No ratings yet
- An Adult OrthodonticsDocument16 pagesAn Adult OrthodonticsDrAla MohamedNo ratings yet
- Non XNDocument9 pagesNon XNNaveenNo ratings yet
- Public Health Lecture NotesDocument4 pagesPublic Health Lecture NotesSharon Gabriel100% (5)
- Diagnosis of Canine ImpactionDocument27 pagesDiagnosis of Canine ImpactionDr.Thrivikhraman KothandaramanNo ratings yet
- Management of Impacted CanineDocument97 pagesManagement of Impacted CanineOluseye SoyeboNo ratings yet
- Congenitally Missing Lateral IncisorDocument17 pagesCongenitally Missing Lateral IncisorAvneet MalikNo ratings yet
- Clinical Cases in Restorative and Reconstructive DentistryFrom EverandClinical Cases in Restorative and Reconstructive DentistryRating: 5 out of 5 stars5/5 (1)
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Orthodontics Classification of Skeletal PDFDocument7 pagesOrthodontics Classification of Skeletal PDFPriyank RaiNo ratings yet
- Orthodontic CurriculumDocument60 pagesOrthodontic CurriculumKiran KumarNo ratings yet
- Lecture (17) Orthodontic Dentistry .: ساملا نانج د Orthopaedic Appliance in OrthodonticDocument3 pagesLecture (17) Orthodontic Dentistry .: ساملا نانج د Orthopaedic Appliance in Orthodonticاسراء فاضل مصطفى100% (1)
- Biomechanical Implications of Rotation Correction in Orthodontics - Case SeriesDocument5 pagesBiomechanical Implications of Rotation Correction in Orthodontics - Case SeriescempapiNo ratings yet
- Preventive OrthodonticsDocument14 pagesPreventive OrthodonticsVaisakh Ramachandran0% (1)
- Burstone1962 PDFDocument18 pagesBurstone1962 PDFParameswaran ManiNo ratings yet
- Orthodontic Supplies CatalogDocument320 pagesOrthodontic Supplies CatalogOrtho OrganizersNo ratings yet
- Bio Mechanics of Tooth MovementDocument26 pagesBio Mechanics of Tooth MovementPriyanka Wadhawan100% (1)
- MARPE AbdAllah Bahaaa Ref NewDocument23 pagesMARPE AbdAllah Bahaaa Ref NewAya ElsayedNo ratings yet
- Preventive Orthodontics / Orthodontic Courses by Indian Dental AcademyDocument15 pagesPreventive Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Biology of Tooth Movement (Final)Document112 pagesBiology of Tooth Movement (Final)Lohith DNo ratings yet
- Growth QuesDocument8 pagesGrowth QuesShameer SFsNo ratings yet
- Sunday, March 2, 2008: Important Orthodontic StudiesDocument6 pagesSunday, March 2, 2008: Important Orthodontic StudiesXnb HajiNo ratings yet
- Genetics and OrthodonticsDocument26 pagesGenetics and OrthodonticsShabeel PnNo ratings yet
- Postgraduate Notes in Orthodontics-1-49Document49 pagesPostgraduate Notes in Orthodontics-1-49Mu'taz ArmanNo ratings yet
- Self-Ligating Brackets Do NotDocument22 pagesSelf-Ligating Brackets Do NotAnkit ChaurhaNo ratings yet
- Retention and RelapseDocument59 pagesRetention and RelapseAshwin ThejaswiNo ratings yet
- Orthodontics in CLP PresentationDocument26 pagesOrthodontics in CLP PresentationSiti FarhanahNo ratings yet
- Presented By: Assistant Professor:: M.R. Vatankhah Dr. H. M.SadeghiDocument36 pagesPresented By: Assistant Professor:: M.R. Vatankhah Dr. H. M.SadeghiMuhammed HassanNo ratings yet
- Orthodontic Expansion: Orthodontic Expansion, Produced by Conventional Fixed Appliances As Well As by Various RemovableDocument7 pagesOrthodontic Expansion: Orthodontic Expansion, Produced by Conventional Fixed Appliances As Well As by Various RemovableNiTa DöéMy HarDianaNo ratings yet
- 5.etiology of MalocclusionDocument20 pages5.etiology of MalocclusionAhmed Hegazy100% (2)
- Occulsal Morphology DeterminantsDocument38 pagesOcculsal Morphology DeterminantsrusschallengerNo ratings yet
- Medically Compromised PatientDocument84 pagesMedically Compromised PatientShubham khandkeNo ratings yet
- Retention & RelapseDocument12 pagesRetention & Relapseshahzeb memonNo ratings yet
- Bite RegistratnDocument68 pagesBite RegistratnBimalKrishnaNo ratings yet
- 36 Canine Retraction in Orthodontics - A Review of Various MethodsDocument9 pages36 Canine Retraction in Orthodontics - A Review of Various MethodsRahma Wahid100% (1)
- Abo GradingDocument11 pagesAbo GradingSonu RajuNo ratings yet
- Arch ExpansionDocument32 pagesArch ExpansionMoola Bharath Reddy100% (5)
- Orthodontic SeminarDocument12 pagesOrthodontic Seminarthanhchon100% (5)
- Twin BlockDocument124 pagesTwin Blockrama deviNo ratings yet
- Classification of Malocclusion Angle's Classification: Antero-Posterior (Sagittal) First Permanent MolarsDocument57 pagesClassification of Malocclusion Angle's Classification: Antero-Posterior (Sagittal) First Permanent Molarsisraa fuadNo ratings yet
- Lec.9 Ortho. MovementDocument10 pagesLec.9 Ortho. MovementSaid SaidNo ratings yet
- Retention and Relapse SeminarDocument51 pagesRetention and Relapse SeminarShipra SehgalNo ratings yet
- 3M - 93C HallTechGuide2191110 PDFDocument21 pages3M - 93C HallTechGuide2191110 PDFDuvan CastilloNo ratings yet
- 9 Cephalometric Analysis 2Document96 pages9 Cephalometric Analysis 2Mei Xiao100% (1)
- 7TranspalatalArchpvol7issue26-32 20190224080331 PDFDocument7 pages7TranspalatalArchpvol7issue26-32 20190224080331 PDFSoe San KyawNo ratings yet
- Crowding 180601115625 PDFDocument109 pagesCrowding 180601115625 PDFVishal SharmaNo ratings yet
- Methods of Gaining Space 2012 - 2Document3 pagesMethods of Gaining Space 2012 - 2Ahmad KhaledNo ratings yet
- Cone Beam Tomography in Orthodontics PDFDocument8 pagesCone Beam Tomography in Orthodontics PDFdruzair007No ratings yet
- Stem Cells - A Ray of Hope in OrthodonticsDocument3 pagesStem Cells - A Ray of Hope in OrthodonticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 6 Postgraduate Notes in Orthodontics-250-299Document54 pages6 Postgraduate Notes in Orthodontics-250-299Mu'taz ArmanNo ratings yet
- Treatment Ofclass II Anomalies PDFDocument224 pagesTreatment Ofclass II Anomalies PDFSabrina Nitulescu100% (1)
- Occlusion OrthodonticsDocument84 pagesOcclusion OrthodonticsMuhammad UzairNo ratings yet
- 66 Allery and OrthodonticDocument5 pages66 Allery and OrthodonticShruthi KamarajNo ratings yet
- Orthodontics DiagnosisDocument26 pagesOrthodontics DiagnosisMu'taz ArmanNo ratings yet
- Canine ImpactionDocument31 pagesCanine Impactionavanthika krishnarajNo ratings yet
- ABO Grading SystemDocument82 pagesABO Grading Systemsanjeed sanjuNo ratings yet
- Rle - NCM 109 Sample OnlyDocument3 pagesRle - NCM 109 Sample OnlyFaine Angela CaonesNo ratings yet
- Chapter Three Research MethodologyDocument7 pagesChapter Three Research MethodologyNejash Abdo IssaNo ratings yet
- Fdi-Oral Cancer-Chairside GuideDocument2 pagesFdi-Oral Cancer-Chairside GuideHien TruongNo ratings yet
- Chapter 01 - Health Care Delivery and Evidence-Based Nursing PracticeDocument9 pagesChapter 01 - Health Care Delivery and Evidence-Based Nursing PracticePrince K. TaileyNo ratings yet
- Desmand Whitson Resume 1PDFDocument2 pagesDesmand Whitson Resume 1PDFRed RaptureNo ratings yet
- 13147Document2 pages13147satishNo ratings yet
- Chapter IDocument11 pagesChapter IShoto TodorokiNo ratings yet
- NSCMP - Claim FormDocument6 pagesNSCMP - Claim FormArun Prabhakaran PNo ratings yet
- IBISWorld - Pharmacies & Drug Stores in The US - 2019Document44 pagesIBISWorld - Pharmacies & Drug Stores in The US - 2019uwybkpeyawxubbhxjyNo ratings yet
- Aspects of The Topic ReadingsDocument4 pagesAspects of The Topic ReadingsBettNo ratings yet
- Summary Maulik SiddhantDocument46 pagesSummary Maulik SiddhantErshad Shafi AhmedNo ratings yet
- Mkell DNP Project 9-16Document2 pagesMkell DNP Project 9-16Miserable*No ratings yet
- Hydro DemolitionDocument1 pageHydro DemolitionAgnes BNo ratings yet
- Protocolo de EscritaDocument5 pagesProtocolo de EscritaGabriela Ruggiero NorNo ratings yet
- World Health Organization (WHO)Document4 pagesWorld Health Organization (WHO)Krista P. AguinaldoNo ratings yet
- Week 10 Assignment - EditedDocument6 pagesWeek 10 Assignment - EditedHugoNo ratings yet
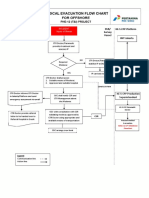
- 3-A4 - Medical Evacuation Flow Chart (Rev.0)Document1 page3-A4 - Medical Evacuation Flow Chart (Rev.0)SiskaNo ratings yet
- Nutrition Essentials For Nursing Practice Dudek 7th Edition Test BankDocument15 pagesNutrition Essentials For Nursing Practice Dudek 7th Edition Test Bankfinnmilcah2puNo ratings yet
- Geron Group 1 ReportingDocument13 pagesGeron Group 1 ReportingPotato TomatoNo ratings yet
- CPH AssignmentDocument3 pagesCPH AssignmentChrystelle Mariano TibayNo ratings yet
- SIMULUS 8 Offline RegistrationDocument8 pagesSIMULUS 8 Offline RegistrationNeutral Body NursingNo ratings yet
- TAEI-TMCH-TNHSRP Presentation FinalDocument26 pagesTAEI-TMCH-TNHSRP Presentation FinalMuraleedharan V R IITMNo ratings yet
- Abortion Care Thrombose ProfylaxeDocument22 pagesAbortion Care Thrombose ProfylaxeambiebieNo ratings yet
- BlindnessDocument29 pagesBlindnessMegawati Abubakar50% (4)
- Clinical Teaching MethodsDocument5 pagesClinical Teaching MethodsFlora AlfaxdNo ratings yet
- Umbilical and Epigastric Hernia Information For PatientsDocument13 pagesUmbilical and Epigastric Hernia Information For PatientsSavulescu OvidiuNo ratings yet
- 1st Summative Test 10th GradeDocument2 pages1st Summative Test 10th GradeMay S. VelezNo ratings yet
- Pediatrics NFDN 2005 Assignment2Document2 pagesPediatrics NFDN 2005 Assignment2api-319232343No ratings yet