Download as pptx, pdf, or txt
You might also like
- Review of A Little Book For New TheologiansDocument3 pagesReview of A Little Book For New Theologianscreative2009No ratings yet
- π (1) π (n) 1 n 1 n i<j i jDocument4 pagesπ (1) π (n) 1 n 1 n i<j i jYuanqingWuNo ratings yet
- Case Study ChryslerDocument10 pagesCase Study ChryslerShatesh Kumar ChandrahasanNo ratings yet
- Schizophrenia: M - MweembaDocument51 pagesSchizophrenia: M - MweembaMaxwell C Jay KafwaniNo ratings yet
- Delusional Disorders & Acute & Transient PsychosisDocument38 pagesDelusional Disorders & Acute & Transient PsychosisHardeep KaurNo ratings yet
- Paranoid Schizophrenia: OlehDocument52 pagesParanoid Schizophrenia: Olehbunga julia100% (1)
- Hamdallah Khalid RN, BSN, Mss Ibn Sina College Palestine Hamdallah Khalid RN, BSN, Mss Ibn Sina College PalestineDocument40 pagesHamdallah Khalid RN, BSN, Mss Ibn Sina College Palestine Hamdallah Khalid RN, BSN, Mss Ibn Sina College PalestineMAYHAMDALLAHNo ratings yet
- SCHIZOPHRENIADocument29 pagesSCHIZOPHRENIAmercygreat2014No ratings yet
- Jawaban Dk2 p3 FullDocument102 pagesJawaban Dk2 p3 FullNaufal DianNo ratings yet
- Schizophrenia Other Psychotic DisorderDocument57 pagesSchizophrenia Other Psychotic DisorderGlory MimiNo ratings yet
- Schizophrenia and Other Psychotic Disorders: Agustine Mahardika MD, PsychDocument57 pagesSchizophrenia and Other Psychotic Disorders: Agustine Mahardika MD, PsychLydia AmaliaNo ratings yet
- Psychological DisordersDocument48 pagesPsychological Disordersapi-448144386100% (1)
- SchizophreniaDocument35 pagesSchizophreniatendolsmithNo ratings yet
- Week 5 - Clinical PsychologyDocument89 pagesWeek 5 - Clinical PsychologyDora SimunovicNo ratings yet
- UntitledDocument40 pagesUntitledCrescia Jane TerazaNo ratings yet
- Schizophrenia: Psychotic Disorders SHMNDocument63 pagesSchizophrenia: Psychotic Disorders SHMNPinkRose BrownSpiceNo ratings yet
- SchizophreniaDocument36 pagesSchizophreniasanyakotwani08No ratings yet
- Chapters 14 & 15 Schizophrenia & Treatment (Color)Document10 pagesChapters 14 & 15 Schizophrenia & Treatment (Color)Carla AndreiaNo ratings yet
- KR - SchizophreniaDocument4 pagesKR - SchizophreniaValantino RamosNo ratings yet
- SchizophreniaDocument33 pagesSchizophreniaAkanshNo ratings yet
- AbPsych Day Two Final1Document103 pagesAbPsych Day Two Final1Rachel AlmiaNo ratings yet
- Schizophrenia Lecture 2010 PART 1 and 2Document69 pagesSchizophrenia Lecture 2010 PART 1 and 2Rahul Kumar DiwakarNo ratings yet
- Mood Disorders and SchizophreniaDocument6 pagesMood Disorders and SchizophreniaAdela ChristinaNo ratings yet
- SchizphreniaDocument151 pagesSchizphreniaAyaBasilioNo ratings yet
- Sschizophrenia LectureDocument27 pagesSschizophrenia Lectureepic sound everNo ratings yet
- PsychosisDocument61 pagesPsychosisJohn CabilanNo ratings yet
- Psychopathology: Fikirte Girma M.D, Psychiatrist Department of Psychiatry AAU November 2014Document38 pagesPsychopathology: Fikirte Girma M.D, Psychiatrist Department of Psychiatry AAU November 2014Z26No ratings yet
- Psychiatric Illness: Schizophrenia and Major DepressionDocument23 pagesPsychiatric Illness: Schizophrenia and Major DepressionLealiza B. BruceNo ratings yet
- Mental Illness: Scene III - BiographyDocument42 pagesMental Illness: Scene III - BiographyHenry LawNo ratings yet
- Schizophrenia: 2 Most Frequent Diagnosis of Patients 14-64 Y/o at CRH in 2008Document52 pagesSchizophrenia: 2 Most Frequent Diagnosis of Patients 14-64 Y/o at CRH in 2008michaelNo ratings yet
- On SchizophreniaDocument30 pagesOn SchizophreniaRanieska GoNo ratings yet
- 3 - Schizophrenia rg1Document35 pages3 - Schizophrenia rg1api-343457547No ratings yet
- PSY1002 Chapter 14 Part 1Document50 pagesPSY1002 Chapter 14 Part 1Melisa AkkuşNo ratings yet
- 9 Psychological DisordersDocument13 pages9 Psychological Disordersvomedoy787No ratings yet
- Inside The World of Schizophrenia: Presented by Lucille Mae P. BorjaDocument8 pagesInside The World of Schizophrenia: Presented by Lucille Mae P. BorjaApol Polendey BorjaNo ratings yet
- Abnormal PsychologyDocument54 pagesAbnormal PsychologyVIJAYKUMAR HIREMATHNo ratings yet
- Psychotic DisordersDocument38 pagesPsychotic DisordersMala Rasaily100% (2)
- Schizophrenia Spectrum Disorders Cognitive DisorderDocument13 pagesSchizophrenia Spectrum Disorders Cognitive DisorderRENEROSE TORRESNo ratings yet
- SchizophreniaDocument49 pagesSchizophreniaJemi LoriNo ratings yet
- Copy-Classification of Psychiatric DisordersDocument56 pagesCopy-Classification of Psychiatric Disordersshadrach bineyNo ratings yet
- Unit 4 - Schizophrenia - Students Copy (2023)Document72 pagesUnit 4 - Schizophrenia - Students Copy (2023)jihanrajabNo ratings yet
- SCHIZOPHRENIADocument16 pagesSCHIZOPHRENIAHanna CarsanoNo ratings yet
- Adigrat UniversityDocument29 pagesAdigrat UniversityabrihamNo ratings yet
- Schizophrenia ENGLISH 2020Document56 pagesSchizophrenia ENGLISH 2020unknownNo ratings yet
- Sub-Types of SchizophreniaDocument76 pagesSub-Types of Schizophreniadrkadiyala2No ratings yet
- Neurobyology Respons Schizophrenia & Other Psychotic DisorderDocument24 pagesNeurobyology Respons Schizophrenia & Other Psychotic DisorderquinnNo ratings yet
- SCHIZOAFFECTIVEDocument37 pagesSCHIZOAFFECTIVEDhea Faizia TasyaNo ratings yet
- SchizophreniaDocument58 pagesSchizophreniaArpit AroraNo ratings yet
- SchizophreniaDocument50 pagesSchizophreniaNabina PaneruNo ratings yet
- Schizophrenia and OtherDocument24 pagesSchizophrenia and OtherMariamNo ratings yet
- SchizoDocument48 pagesSchizobemina jaNo ratings yet
- Lecture 1-Introduction of Abnormal PsychologyPDF - 240220 - 220006Document24 pagesLecture 1-Introduction of Abnormal PsychologyPDF - 240220 - 220006hui xin ngNo ratings yet
- Some Procedural IssuesDocument13 pagesSome Procedural IssuesAlexandra Adina RădescuNo ratings yet
- Abnormal Psychology Final CoachingDocument638 pagesAbnormal Psychology Final Coachingmonne100% (1)
- Mental DisordersDocument34 pagesMental DisordersINDIRAKALYANINo ratings yet
- Psychotic DisordersDocument70 pagesPsychotic DisordersGiorgi TamazashviliNo ratings yet
- Case VignettesfinalpdfDocument189 pagesCase VignettesfinalpdfPratik Kumar DeyNo ratings yet
- Psychological DisordersDocument52 pagesPsychological Disordersember_memoriesNo ratings yet
- Topic 8 Schizophrenia SpectrumDocument35 pagesTopic 8 Schizophrenia Spectrumelphas walelaNo ratings yet
- Personality Disorders TAUDocument48 pagesPersonality Disorders TAUZakaria AhmedNo ratings yet
- Schizophrenia and Psychotic Disorders PPT Chap 21Document46 pagesSchizophrenia and Psychotic Disorders PPT Chap 21Claudia SanchezNo ratings yet
- Summary of E. Fuller Torrey's Surviving Schizophrenia, 7th EditionFrom EverandSummary of E. Fuller Torrey's Surviving Schizophrenia, 7th EditionNo ratings yet
- Schizophrenia Unmasked: Personal Stories and Proven Techniques to Reclaim Your LifeFrom EverandSchizophrenia Unmasked: Personal Stories and Proven Techniques to Reclaim Your LifeNo ratings yet
- Bovine MastitisDocument31 pagesBovine MastitisMitao WilbertNo ratings yet
- Science Fiction EssayDocument5 pagesScience Fiction Essayyezfvwwhd100% (2)
- The Bible Episode 5 The SurvivalDocument2 pagesThe Bible Episode 5 The SurvivalMarestel SivesindNo ratings yet
- MODULE 1 PsychologyDocument48 pagesMODULE 1 PsychologyTanu ShreeNo ratings yet
- Template e Rekam MedisDocument30 pagesTemplate e Rekam MedisChusnul MubarokNo ratings yet
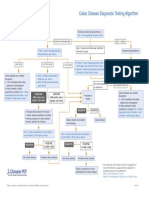
- Celiac Disease Diagnostic Testing AlgorithmDocument1 pageCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakNo ratings yet
- Aleister Crowley - Liber CDXII - Liber A Vel ArmorumDocument5 pagesAleister Crowley - Liber CDXII - Liber A Vel ArmorumnegreanNo ratings yet
- Chemistry of LifeDocument15 pagesChemistry of LifeEnggar PrapithaNo ratings yet
- 1179 1186Document9 pages1179 1186theoNo ratings yet
- Jesus Asks, What Are You Doing To Promote Devotion To My MotherDocument5 pagesJesus Asks, What Are You Doing To Promote Devotion To My MotherThe Fatima CenterNo ratings yet
- The Analysis of Organizational Culture For Improving Corporate Performance at PT. XYZ DiscreetDocument10 pagesThe Analysis of Organizational Culture For Improving Corporate Performance at PT. XYZ DiscreetTsweeg OnlineNo ratings yet
- The Cask of Amontillado by Edgar Allan Poe (1846)Document29 pagesThe Cask of Amontillado by Edgar Allan Poe (1846)Arlein Cess MercadoNo ratings yet
- Amar Jesani: Violence and Health Care Profession in IndiaDocument13 pagesAmar Jesani: Violence and Health Care Profession in IndiaAmar JesaniNo ratings yet
- Arduino Based Smart Irrigation System Using Iot: March 2017Document6 pagesArduino Based Smart Irrigation System Using Iot: March 2017Your TechMateNo ratings yet
- ' Fo 2 " / I, J: ZB,' (+. R (,?.D)Document2 pages' Fo 2 " / I, J: ZB,' (+. R (,?.D)SUMAN SAGARNo ratings yet
- In The Inter Media Te Grade S: by Sol Concepcion M. PamatDocument6 pagesIn The Inter Media Te Grade S: by Sol Concepcion M. PamatArnold PiamonteNo ratings yet
- 290 PentCapital Investment Corporation Vs MahinayDocument2 pages290 PentCapital Investment Corporation Vs MahinayJanno SangalangNo ratings yet
- Logical Reasoning 03 - Distribution-1 - Class Notes - MBA Elite 2023Document34 pagesLogical Reasoning 03 - Distribution-1 - Class Notes - MBA Elite 2023smit prajapatiNo ratings yet
- Normal Carbohydrate Balance and Maintenance of Blood Glucose LevelsDocument2 pagesNormal Carbohydrate Balance and Maintenance of Blood Glucose LevelsSig G. MiNo ratings yet
- Arabic Finger Ring From The Viking Age of Birka, Sweden PDFDocument7 pagesArabic Finger Ring From The Viking Age of Birka, Sweden PDFClaudia Patricia Arango100% (1)
- Written ExplanationDocument2 pagesWritten Explanationapi-537829855No ratings yet
- AXA Report 2007Document480 pagesAXA Report 2007dindaaynNo ratings yet
- Stolba Amp Hannestad Eds Chronologies of The Black Sea Area in The Period C 400 100 BCDocument338 pagesStolba Amp Hannestad Eds Chronologies of The Black Sea Area in The Period C 400 100 BCocratsira26No ratings yet
- Resume Teaching2016Document1 pageResume Teaching2016api-307736451No ratings yet
- Mul - Factorial Falls Risk Assessment: (Acute Hospital)Document2 pagesMul - Factorial Falls Risk Assessment: (Acute Hospital)eimear100% (1)
- 12 Years A Slave - SummaryDocument2 pages12 Years A Slave - SummaryEnrique SchererNo ratings yet
- SfcaDocument95 pagesSfcaविश्वेश सिंहNo ratings yet