Download as pptx, pdf, or txt
You might also like
- Heart Failure Topic DiscussionDocument11 pagesHeart Failure Topic Discussionapi-665372449No ratings yet
- Antiviral Effects of Ibogaine and Hepatitis - LotsofDocument22 pagesAntiviral Effects of Ibogaine and Hepatitis - Lotsofjesterstable100% (2)
- CANNABISDocument5 pagesCANNABISGeorgina AttipoeNo ratings yet
- SHARGELDocument2,115 pagesSHARGELFrançoise BNo ratings yet
- Acute Ischemic Stroke: by Steven H. Nakajima, Pharm.D., BCCCP and Katleen Wyatt Chester, Pharm.D., BCCCP, BCGPDocument26 pagesAcute Ischemic Stroke: by Steven H. Nakajima, Pharm.D., BCCCP and Katleen Wyatt Chester, Pharm.D., BCCCP, BCGPCristian Florin CrasmaruNo ratings yet
- Reference Guide For Foreign Pharmacy Licensing ExamDocument6 pagesReference Guide For Foreign Pharmacy Licensing Examcarp liciniaNo ratings yet
- Hypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pharmacist Role in ADR MDocument9 pagesPharmacist Role in ADR Mimran moopansNo ratings yet
- APHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDocument13 pagesAPHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDrSamia El WakilNo ratings yet
- Drug Interactions of Antianginal Drugs..Document40 pagesDrug Interactions of Antianginal Drugs..Kamal SikandarNo ratings yet
- تجمعيات اسئلة كل موضوع لحالهDocument120 pagesتجمعيات اسئلة كل موضوع لحالهMian. Shoaib.No ratings yet
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiNo ratings yet
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22No ratings yet
- 2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDDocument58 pages2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDKishan SethNo ratings yet
- AMH Must FlagDocument2 pagesAMH Must FlagpurnibaNo ratings yet
- 2013 December Exam CompilationDocument7 pages2013 December Exam CompilationabbasyaqobiNo ratings yet
- Anupama Cv-Pharmacist-2021Document2 pagesAnupama Cv-Pharmacist-2021ragesh r nairNo ratings yet
- Clinical Pharmacy Lab - Quiz Part 2Document4 pagesClinical Pharmacy Lab - Quiz Part 2Aassh DcmbrNo ratings yet
- Katzung & Trevor's Pharmacology Examination & Board Review-Pages-303-311Document9 pagesKatzung & Trevor's Pharmacology Examination & Board Review-Pages-303-311Princess Alyssa H. PasajolNo ratings yet
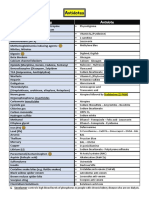
- Antidote Indication Mode of ActionDocument5 pagesAntidote Indication Mode of ActionRegalado AguhayonNo ratings yet
- Antidotes and The Clinical Applications Antidote: An Antidote Is A Substance Which Can Counteract A Form ofDocument2 pagesAntidotes and The Clinical Applications Antidote: An Antidote Is A Substance Which Can Counteract A Form ofManohar Chowdary KovvuriNo ratings yet
- HAAD Applicant KitDocument9 pagesHAAD Applicant KitMenGuitarNo ratings yet
- Diabetes Type 2 HassanDocument26 pagesDiabetes Type 2 Hassanyash_acharya007100% (1)
- Drugs Interaction1Document13 pagesDrugs Interaction1Akshay MandhotraNo ratings yet
- Name Honor Pledge (Signature) : Questions 1 - 2 Refer To The Following CaseDocument9 pagesName Honor Pledge (Signature) : Questions 1 - 2 Refer To The Following CasegregstevensNo ratings yet
- Cam Therapies, Vitamins, Otc StudentDocument30 pagesCam Therapies, Vitamins, Otc StudentLynn EarnestNo ratings yet
- Cardiology Lectures 1 4 DR - Deduyo PDFDocument31 pagesCardiology Lectures 1 4 DR - Deduyo PDFMiguel Cuevas DolotNo ratings yet
- QuestionsDocument13 pagesQuestionsMikee MeladNo ratings yet
- 3dr Year Common Biochemistry MCQsDocument8 pages3dr Year Common Biochemistry MCQsYasmin Amr NounouNo ratings yet
- Therapeutic Classification of DrugsDocument35 pagesTherapeutic Classification of DrugsJomarie Villalobos BuñoNo ratings yet
- Cardiovascular Disorders LectureDocument132 pagesCardiovascular Disorders LectureHarper Epps100% (1)
- Clinical Pharmacology Book 2018Document304 pagesClinical Pharmacology Book 2018Sumaiya Islam Khan100% (1)
- Principles of PharmacotherapyDocument40 pagesPrinciples of Pharmacotherapyjunitria13No ratings yet
- TDM of DigoxinDocument13 pagesTDM of DigoxinMounika16 PedamalluNo ratings yet
- SPIRIVA HandiHaler InstructionsDocument9 pagesSPIRIVA HandiHaler InstructionssamyvnNo ratings yet
- RPS Full Mock Exam Part 2 May2022FINALDocument72 pagesRPS Full Mock Exam Part 2 May2022FINALAshley LeeNo ratings yet
- Mock Test 1 Part A Summer 2006Document53 pagesMock Test 1 Part A Summer 2006Alida Rautenbach0% (1)
- Ee Summary Pebc Osce ResourcesDocument56 pagesEe Summary Pebc Osce ResourcesChristianNo ratings yet
- Drugs Used in PregnancyDocument1 pageDrugs Used in PregnancyFahad AlkenaniNo ratings yet
- Osam D Tab Leaflet Pakistan PDFDocument1 pageOsam D Tab Leaflet Pakistan PDFpharmacist PUCPNo ratings yet
- Ischaemic Heart DiseaseDocument30 pagesIschaemic Heart DiseaseEB100% (1)
- Pharmacotherapy For SchizophreniaDocument17 pagesPharmacotherapy For SchizophreniaNadya SaptarinaNo ratings yet
- Ed enDocument376 pagesEd enNashria Rusdhy100% (2)
- Multiple Sclerosis Drug TherapyDocument2 pagesMultiple Sclerosis Drug Therapyampogison08No ratings yet
- Psychiatric and Neurological Drugs Mock TestDocument46 pagesPsychiatric and Neurological Drugs Mock TestSylvia AmakaNo ratings yet
- Side Effects of Common Drugs PDFDocument2 pagesSide Effects of Common Drugs PDFImran ChaudhryNo ratings yet
- In The Name of GOD: Calculation Summary For KAPSDocument21 pagesIn The Name of GOD: Calculation Summary For KAPSMushtaq AhmedNo ratings yet
- Day 1 PNUDocument250 pagesDay 1 PNUM LNo ratings yet
- Renal PharmacologyDocument52 pagesRenal PharmacologyashrafNo ratings yet
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanNo ratings yet
- Drugs of ChoiceDocument2 pagesDrugs of ChoiceGian Carla SoNo ratings yet
- Autacoids: Group No. 1Document92 pagesAutacoids: Group No. 1Rohan Pal100% (1)
- 8B - Antianginal DrugsDocument70 pages8B - Antianginal Drugslalitrajindolia100% (1)
- Antidotes: Poison/Drug AntidoteDocument1 pageAntidotes: Poison/Drug AntidoteAfsal Ur FriendNo ratings yet
- Drug Interaction Report PDFDocument111 pagesDrug Interaction Report PDFbaerbaNo ratings yet
- CVS MCQS 06 QDocument2 pagesCVS MCQS 06 Qharshad patelNo ratings yet
- Pharm MnemonicsDocument47 pagesPharm MnemonicsMina RacadioNo ratings yet
- Exam Model 1: 1-Therapeutic Index IsDocument165 pagesExam Model 1: 1-Therapeutic Index Is8pj54fxgjvNo ratings yet
- Pharmacogenomics of Human Drug Transporters: Clinical ImpactsFrom EverandPharmacogenomics of Human Drug Transporters: Clinical ImpactsNo ratings yet
- Guidelines for Measuring Household and Individual Dietary DiversityFrom EverandGuidelines for Measuring Household and Individual Dietary DiversityNo ratings yet
- The 24-Hour Pharmacist: Advice, Options, and Amazing Cures from America's Most Trusted PharmacistFrom EverandThe 24-Hour Pharmacist: Advice, Options, and Amazing Cures from America's Most Trusted PharmacistNo ratings yet
- Marriage Uner Hindu LawDocument48 pagesMarriage Uner Hindu LawBharath GowdaNo ratings yet
- Legal Methods SynopsisDocument2 pagesLegal Methods SynopsisBharath GowdaNo ratings yet
- Patient Profile Form - DSCPDocument6 pagesPatient Profile Form - DSCPBharath GowdaNo ratings yet
- Diabetis Mellitus Ischemic Heart Disease Chronic Renal FailureDocument24 pagesDiabetis Mellitus Ischemic Heart Disease Chronic Renal FailureBharath GowdaNo ratings yet
- KrupaCon 2018 - BengaluruDocument8 pagesKrupaCon 2018 - BengaluruBharath GowdaNo ratings yet
- Inflammation and Healing: Inflammation "Local Response of Living Mammalian Tissues To Injury Due To Any Agent"Document121 pagesInflammation and Healing: Inflammation "Local Response of Living Mammalian Tissues To Injury Due To Any Agent"Bharath GowdaNo ratings yet
- Cell Injury: Ii PharmdDocument51 pagesCell Injury: Ii PharmdBharath GowdaNo ratings yet
- Shock: Ii PharmdDocument25 pagesShock: Ii PharmdBharath GowdaNo ratings yet
- Rational Drug Use: Presented By: H.SruthiDocument19 pagesRational Drug Use: Presented By: H.SruthiBharath Gowda100% (1)
- ��تجميعات الفارما�Document4 pages��تجميعات الفارما�Turky TurkyNo ratings yet
- Aurobindo PharmaceuticalsDocument7 pagesAurobindo Pharmaceuticalsitsvijay100% (1)
- FluconazoleDocument14 pagesFluconazoleasdwasdNo ratings yet
- Tramadol + ParacetamolDocument4 pagesTramadol + ParacetamolFaye Andrea Francisco100% (2)
- Cannabis PK 2024 Final For UploadDocument27 pagesCannabis PK 2024 Final For UploadswagciciliNo ratings yet
- Myanmar Regulatory and Market ProfileDocument15 pagesMyanmar Regulatory and Market ProfileMaaz Khan100% (1)
- Drug Study - ER-1ST 50Document64 pagesDrug Study - ER-1ST 50Merlash MerlaNo ratings yet
- List of Drug OtotoxicDocument3 pagesList of Drug OtotoxicLukas I Nyoman Yesaya CavinNo ratings yet
- Pharmacology Chapterwise Year Questions 2nd Yr BdsDocument9 pagesPharmacology Chapterwise Year Questions 2nd Yr Bds76 S.SHRAVAN KUMARNo ratings yet
- Sample Case ScenarioDocument10 pagesSample Case ScenarioKarilee Salcedo AyunayunNo ratings yet
- Generic Name: Brand Name: Lasix Classification: Loop DiureticsDocument5 pagesGeneric Name: Brand Name: Lasix Classification: Loop DiureticsKat ZNo ratings yet
- Master Drugs Database - EgyptDocument442 pagesMaster Drugs Database - EgyptNizar SalehNo ratings yet
- World of BiosimilarsDocument20 pagesWorld of BiosimilarsWasi AkhtarNo ratings yet
- Directorate General of Drug Administration: SL Name of The Pharmaceutical Address Location Licence No. Present StatusDocument2 pagesDirectorate General of Drug Administration: SL Name of The Pharmaceutical Address Location Licence No. Present StatusAnamika SahaNo ratings yet
- Oxybutynin Chloride Tablet, USPDocument8 pagesOxybutynin Chloride Tablet, USPsurafelNo ratings yet
- S&P Pharma Industry Overview - 11252010Document49 pagesS&P Pharma Industry Overview - 11252010earajesh100% (1)
- PARENTERAL MEDICATION Manual and Checklist 1Document14 pagesPARENTERAL MEDICATION Manual and Checklist 1Hazel Shaine BaybayanNo ratings yet
- PharmacovigilanceDocument45 pagesPharmacovigilancepavani valluriNo ratings yet
- The Ultimate Guide To ADHD MedicationDocument20 pagesThe Ultimate Guide To ADHD MedicationM Mohsin Chowdhury100% (2)
- 1re Pds Autoplant Modeler LTR en LR 0716Document1 page1re Pds Autoplant Modeler LTR en LR 0716kk kumarNo ratings yet
- Generic Name Therapeutic Classifications Indication Popular Brand NameDocument8 pagesGeneric Name Therapeutic Classifications Indication Popular Brand NameEderNo ratings yet
- Article Title Here in Title Case (Alt+A)Document8 pagesArticle Title Here in Title Case (Alt+A)Annafiatu zakiahNo ratings yet
- RisperidoneDocument4 pagesRisperidoneimaginarna_88No ratings yet
- Polypharmacy PDFDocument9 pagesPolypharmacy PDFsheryl maeNo ratings yet
- FDA Approved NMEs 2003 2018 ExcelDocument34 pagesFDA Approved NMEs 2003 2018 ExcelsurvivorNo ratings yet
- UnasynDocument3 pagesUnasynianecunar100% (4)
- Obat Di Apotek Plus SuplierDocument48 pagesObat Di Apotek Plus SuplierApotek MandaNo ratings yet
- Assignment 1 For Chem of Natural ProductsDocument4 pagesAssignment 1 For Chem of Natural ProductsBreeza Marie VeralloNo ratings yet