Download as pptx, pdf, or txt
You might also like
- Hensleys Practical Approach To Cardiothoracic Anesthesia Sixth EditionDocument62 pagesHensleys Practical Approach To Cardiothoracic Anesthesia Sixth Editiontimothy.daniels842100% (46)
- 1 - Anatomy - Pass - Mrcog 2017Document92 pages1 - Anatomy - Pass - Mrcog 2017omernouman100% (2)
- Legg-Calvé-Perthes Disease - An Overview With Recent LiteratureDocument10 pagesLegg-Calvé-Perthes Disease - An Overview With Recent LiteratureFranz BlacuttNo ratings yet
- Hydrocephalus IDocument52 pagesHydrocephalus IVlad Alexandra50% (2)
- A Skeletal Traction Technique For Proximal Femur Fracture Management in An Austere EnvironmentDocument5 pagesA Skeletal Traction Technique For Proximal Femur Fracture Management in An Austere EnvironmentJean CotteNo ratings yet
- Colles FractureDocument89 pagesColles Fracturenur syafiqah kamaruzaman100% (1)
- Congenital Muscular TorticollisDocument29 pagesCongenital Muscular Torticolliskashmala afzal100% (1)
- Orthopedic SlidesDocument78 pagesOrthopedic SlidesAzry Mustapa100% (1)
- Classification of StrokeDocument3 pagesClassification of StrokeafhamazmanNo ratings yet
- Cervical SpondylosisDocument25 pagesCervical Spondylosisjeevan ghimireNo ratings yet
- Management Head Injury in ICUDocument5 pagesManagement Head Injury in ICUIrma KusumaNo ratings yet
- Classification of Bone TumoursDocument3 pagesClassification of Bone TumoursMalueth AnguiNo ratings yet
- Degenerative Disorders of Lumbar SpineDocument54 pagesDegenerative Disorders of Lumbar Spineapi-19916399No ratings yet
- Scapulohumeral PeriarthritisDocument29 pagesScapulohumeral PeriarthritisMárcia PatríciaNo ratings yet
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- TKR RehabilitationDocument1 pageTKR RehabilitationgursangeetNo ratings yet
- M.P.T. Neurology Syllabus by Dr. Krishna N. SharmaDocument7 pagesM.P.T. Neurology Syllabus by Dr. Krishna N. SharmaDr. Krishna N. Sharma0% (1)
- Supracondylar Humerus FractureDocument20 pagesSupracondylar Humerus FractureMusyawarah MelalaNo ratings yet
- Cervical PalpationDocument22 pagesCervical Palpationpraveen100% (12)
- PNF FullDocument46 pagesPNF FullHUZAIFA YAMAAN100% (1)
- Congenital Talipes Equino-VarusDocument48 pagesCongenital Talipes Equino-VarusKojo DuncanNo ratings yet
- CRANIOVETEBRALJUNCTIONDocument130 pagesCRANIOVETEBRALJUNCTIONdrarunrao100% (1)
- Endocrinopathies Are Now Well Recognized. These Include Myopathies Associated With ThyroidDocument10 pagesEndocrinopathies Are Now Well Recognized. These Include Myopathies Associated With ThyroidTeves AdrianNo ratings yet
- Osteomyelitis Metabolic Bone DisordersDocument36 pagesOsteomyelitis Metabolic Bone DisordersVishesh JainNo ratings yet
- Overview of Spinal Cord Injuries - PhysiopediaDocument20 pagesOverview of Spinal Cord Injuries - PhysiopediaRaina Ginella DsouzaNo ratings yet
- Awareness of PoliomyelitisDocument23 pagesAwareness of Poliomyelitissabreen hires100% (1)
- Amputation: Sites of Amputation: UEDocument6 pagesAmputation: Sites of Amputation: UEChristine PilarNo ratings yet
- ARCHDocument63 pagesARCHDebashish Chanda100% (1)
- BHTDocument18 pagesBHTNitesh KumawatNo ratings yet
- Thyroid NeoplasmDocument11 pagesThyroid NeoplasmPravin KumarNo ratings yet
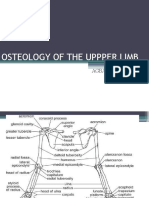
- Osteology of Upper LimbDocument63 pagesOsteology of Upper LimbAkomolede AbosedeNo ratings yet
- Fractures DR MadehDocument12 pagesFractures DR Madehdoos1No ratings yet
- Presentation Brachial Plexus Injuries in PeadsDocument30 pagesPresentation Brachial Plexus Injuries in Peadskashmala afzalNo ratings yet
- Erbs PalsyDocument9 pagesErbs PalsyVatsalVermaNo ratings yet
- What Is PolymyositisDocument24 pagesWhat Is PolymyositisAshraf MobyNo ratings yet
- De Quervain SyndromeDocument5 pagesDe Quervain Syndromebangla018No ratings yet
- Shoulder Dislocation: Nguyen Phuoc Thanh - MDDocument71 pagesShoulder Dislocation: Nguyen Phuoc Thanh - MDThành NPNo ratings yet
- 4 Year B.P.T. Subject: Physiotherapy in OrthopaedicsDocument36 pages4 Year B.P.T. Subject: Physiotherapy in OrthopaedicsNageswaraRoyal GovindugariNo ratings yet
- Brachial Plexus InjuriesDocument64 pagesBrachial Plexus Injuriesprashanth naikNo ratings yet
- Pediatric OrthopaedicDocument66 pagesPediatric OrthopaedicDhito RodriguezNo ratings yet
- Peripheral Nerve InjuriesDocument12 pagesPeripheral Nerve InjuriesJiggs LimNo ratings yet
- Flexor Tendon Injury: Dr. BestinDocument53 pagesFlexor Tendon Injury: Dr. Bestinbestin athappilly100% (1)
- 8758 - PPT AchondroplasiaDocument33 pages8758 - PPT AchondroplasiaFidesha Nurganiah SiregarNo ratings yet
- Ataxias Neuro Condition DetailedDocument80 pagesAtaxias Neuro Condition DetailedMikail AtiyehNo ratings yet
- Thomas' SplintDocument2 pagesThomas' SplintCee SanchezNo ratings yet
- Anatomy and Physiology of SkinDocument2 pagesAnatomy and Physiology of SkinjeromevmagatNo ratings yet
- Sprengel's ShoulderDocument21 pagesSprengel's ShoulderNahayo Xavier100% (1)
- Ulnar Nerve PalsyDocument63 pagesUlnar Nerve PalsyArben Cenollari100% (1)
- S Pondy Lolis ThesisDocument13 pagesS Pondy Lolis ThesisFadlu Manaf100% (1)
- Tabes DorsalisDocument36 pagesTabes DorsalisEric ChristianNo ratings yet
- Chondromalacia Patella - Causes & Treatment - Knee Pain ExplainedDocument5 pagesChondromalacia Patella - Causes & Treatment - Knee Pain ExplainedJames MukhwanaNo ratings yet
- Klumpke's ParalysisDocument7 pagesKlumpke's ParalysisNeelam VermaNo ratings yet
- Splints and Tractions in OrthopaedicsDocument26 pagesSplints and Tractions in OrthopaedicsNailahRahmahNo ratings yet
- Basic of Manual TherapyDocument30 pagesBasic of Manual Therapycamy bhagatNo ratings yet
- Avn and Perthes DiseaseDocument29 pagesAvn and Perthes DiseaseRoopa Lexmy MuniandyNo ratings yet
- Club Foot-Dr J SahooDocument9 pagesClub Foot-Dr J SahooSheel Gupta100% (1)
- Spinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PuneDocument43 pagesSpinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PunePraneetha NouduriNo ratings yet
- Assignment: Cervical SpondylosisDocument14 pagesAssignment: Cervical SpondylosisJaspreet kaurNo ratings yet
- Non UnionDocument25 pagesNon UnionHaziq AnuarNo ratings yet
- Coxa ValgaDocument7 pagesCoxa Valgachitz.14No ratings yet
- Turf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTurf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Uptodate: Chronic Kidney DiseaseDocument13 pagesUptodate: Chronic Kidney DiseaseAtiqah ShahNo ratings yet
- Hollow Cheeeks GuideDocument52 pagesHollow Cheeeks Guidepoomisuk2550No ratings yet
- Jennifer ResumeDocument3 pagesJennifer Resumeapi-266976751No ratings yet
- Wondfo Optical Coagulation OCG 102 1Document2 pagesWondfo Optical Coagulation OCG 102 1asfand yaRNo ratings yet
- Intracranial Pressure: Current Perspectives On Physiology and MonitoringDocument11 pagesIntracranial Pressure: Current Perspectives On Physiology and MonitoringCristian Andres Arancibia GomezNo ratings yet
- ANAT 1100 - Tutorial 1 - F2023 - OND-OnE - StudentDocument42 pagesANAT 1100 - Tutorial 1 - F2023 - OND-OnE - StudentHelen DaoNo ratings yet
- Pit and Fissure SealantsDocument35 pagesPit and Fissure SealantsshrutiNo ratings yet
- Shivering in The Postoperative PatientDocument5 pagesShivering in The Postoperative PatientBrian SoesantoNo ratings yet
- Procedure Checklist For Assissting Chest Tube Insertion NCM 112 SL Done Not DoneDocument3 pagesProcedure Checklist For Assissting Chest Tube Insertion NCM 112 SL Done Not DoneAngelica GuevarraNo ratings yet
- Endo Don TicsDocument11 pagesEndo Don TicsLang100% (1)
- Nursing Lab Articles As Per Indian Nursing CouncilDocument52 pagesNursing Lab Articles As Per Indian Nursing CouncilRahul KashyapNo ratings yet
- AVOX July2011Document6 pagesAVOX July2011Kriss JonesNo ratings yet
- Palatal InjectionDocument10 pagesPalatal InjectionJose Salas AdragnaNo ratings yet
- Types of Heart DiseasesDocument4 pagesTypes of Heart DiseaseslalalallaNo ratings yet
- Tracheostomy Care and SuctionDocument2 pagesTracheostomy Care and SuctionMsPocketbook HoarderNo ratings yet
- Jeyaraj 2018Document16 pagesJeyaraj 2018shagun singhNo ratings yet
- Pyogenic Granuloma A Case ReportDocument9 pagesPyogenic Granuloma A Case ReportSafira HlwNo ratings yet
- Upper Extraction ForcepsDocument45 pagesUpper Extraction ForcepsTina SioNo ratings yet
- Hysterosalphingogram: Dr.C.Oviya Mbbs Ms (O&G)Document93 pagesHysterosalphingogram: Dr.C.Oviya Mbbs Ms (O&G)Oviya ChitharthanNo ratings yet
- NicardipineeeDocument8 pagesNicardipineeekevin100% (1)
- CGHS Pune Rates 2018Document44 pagesCGHS Pune Rates 2018N.J. WaghmareNo ratings yet
- Emergency and Acute Phase in Burns - Afriyanti SandhiDocument45 pagesEmergency and Acute Phase in Burns - Afriyanti SandhiPtunk Ndu PutraNo ratings yet
- Introduction, Deep ReflexesDocument10 pagesIntroduction, Deep ReflexesQairul AzmanNo ratings yet
- Kim Kunzman ResumeDocument3 pagesKim Kunzman Resumeapi-280455698No ratings yet
- Percutaneous Endoscopic GastrostomyDocument27 pagesPercutaneous Endoscopic GastrostomyDoha EbedNo ratings yet
- Total Hip Replacement v4.1 Jan20Document3 pagesTotal Hip Replacement v4.1 Jan20DindaNo ratings yet
- Luis 18Document129 pagesLuis 18José santanaNo ratings yet