Download as pptx, pdf, or txt
You might also like
- ATLSPracticeTest3 PDFDocument10 pagesATLSPracticeTest3 PDFRodrigo Sanjines80% (5)
- Group 8: Patient Case History of Present IllnessDocument4 pagesGroup 8: Patient Case History of Present IllnessShara AboNo ratings yet
- W1. Pendekatan Sesak Pada AnakDocument32 pagesW1. Pendekatan Sesak Pada Anaksekrekomdik RSPDNo ratings yet
- NCP - Impaired Gas ExchangeDocument4 pagesNCP - Impaired Gas ExchangeRene John Francisco100% (1)
- Respiration in Fish N FrogDocument23 pagesRespiration in Fish N FrogHazirah HussinNo ratings yet
- To Make 9 BraceletsDocument23 pagesTo Make 9 Braceletssipil010No ratings yet
- Home PlannerDocument12 pagesHome PlannerSAndrewNo ratings yet
- Being Hungarian in Cleveland: Maintaining Language, Culture, and TraditionsFrom EverandBeing Hungarian in Cleveland: Maintaining Language, Culture, and TraditionsNo ratings yet
- American ArchitectureDocument50 pagesAmerican ArchitectureRoland CepedaNo ratings yet
- Transform Your Home into a Stylish Haven: Unique home décor: Modern home decorFrom EverandTransform Your Home into a Stylish Haven: Unique home décor: Modern home decorNo ratings yet
- Heavenly PlacesDocument425 pagesHeavenly PlacesGerald MazzarellaNo ratings yet
- Workshop #4 Internal Medicine IDocument78 pagesWorkshop #4 Internal Medicine IhevinpatelNo ratings yet
- Physical Examination Techniques and ManueversDocument160 pagesPhysical Examination Techniques and ManueversMa-anJaneDiamosNo ratings yet
- Case of ENDocument73 pagesCase of ENHarold Nathan TanNo ratings yet
- Respiratory Assessment OHT Branding EditsDocument25 pagesRespiratory Assessment OHT Branding EditsDeepika LingamNo ratings yet
- Workshop #5 Internal Medicine IIDocument77 pagesWorkshop #5 Internal Medicine IIhevinpatelNo ratings yet
- 2-Shortness of Breath by DR - HananDocument49 pages2-Shortness of Breath by DR - HananSoon SheedNo ratings yet
- CNUR 107S Respiratory Assessment Final Version 2024SDocument53 pagesCNUR 107S Respiratory Assessment Final Version 2024Sjennifertruong2108No ratings yet
- Family Case Presentation: Abat FamilyDocument80 pagesFamily Case Presentation: Abat FamilyGeraldine Marie SalvoNo ratings yet
- Cm2 Cu10 Assessment of Thorax Lungs 1Document24 pagesCm2 Cu10 Assessment of Thorax Lungs 1MARIANA FAITH LUCASNo ratings yet
- Overview Cardio-Respiratory SystemDocument20 pagesOverview Cardio-Respiratory Systemdhea wirantiNo ratings yet
- Shortness of BreathDocument49 pagesShortness of BreathMetkaNo ratings yet
- Gnrs 5320 Lessonpowerpoint RevisedDocument30 pagesGnrs 5320 Lessonpowerpoint Revisedapi-277849152No ratings yet
- Shortness of Breath NotesDocument7 pagesShortness of Breath NotesChananNo ratings yet
- N1030 Theory Week 5 PPT - Student VersionDocument70 pagesN1030 Theory Week 5 PPT - Student Versiontksd7No ratings yet
- CASE PRESENTATION On Respiratory MedicineDocument34 pagesCASE PRESENTATION On Respiratory MedicineTanoy BoseNo ratings yet
- DYSPNEADocument37 pagesDYSPNEAdr. snehal patilNo ratings yet
- 25th August Respiratory Integrated Case Study 2020Document44 pages25th August Respiratory Integrated Case Study 2020Sabashnee GovenderNo ratings yet
- Pneumonia and CXR Revision: Leigh-Anne HillDocument51 pagesPneumonia and CXR Revision: Leigh-Anne Hillapi-195799092No ratings yet
- Pa Thorax LungsDocument88 pagesPa Thorax LungsLovelights ZamoraNo ratings yet
- CP3 Respiratory SystemDocument23 pagesCP3 Respiratory SystemirynNo ratings yet
- A Comprehensive Neurological Examination Guide and Approach To LocalizationDocument86 pagesA Comprehensive Neurological Examination Guide and Approach To LocalizationLiberty AgcaoiliNo ratings yet
- Chapter - 027.bridge To NCLEX Review Question AnswersDocument9 pagesChapter - 027.bridge To NCLEX Review Question AnswersJackie JuddNo ratings yet
- Respiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkDocument34 pagesRespiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkThea BerteaNo ratings yet
- 2nd Activity - Patient With Cough and FeverDocument40 pages2nd Activity - Patient With Cough and FeverJethro Floyd QuintoNo ratings yet
- A Grand Tour of Pulmonary MedicineDocument115 pagesA Grand Tour of Pulmonary MedicineKaram SarhanNo ratings yet
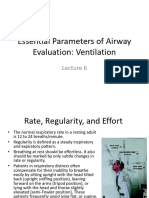
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- Respiratory Osce: AMSA Edinburgh X IMU Y4Document34 pagesRespiratory Osce: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Kuliah Pakar 2 Dyspnea PBLDocument35 pagesKuliah Pakar 2 Dyspnea PBLTrisya AksaraNo ratings yet
- Protocol - Lymphangioleiomyomatosis (HCC 02242023)Document15 pagesProtocol - Lymphangioleiomyomatosis (HCC 02242023)Brian OlajeNo ratings yet
- COPDDocument47 pagesCOPDMegha VadanereNo ratings yet
- Assessment of The Respiratory SystemDocument49 pagesAssessment of The Respiratory SystemMilanisti22No ratings yet
- Case Study On BronchitisDocument19 pagesCase Study On BronchitisSuchitaNo ratings yet
- A Guide To Physical ExaminationDocument73 pagesA Guide To Physical ExaminationDessy AmaranthaNo ratings yet
- Function of the respiratory system وظائف الجهاز التنفسيDocument15 pagesFunction of the respiratory system وظائف الجهاز التنفسيnoorayg.jNo ratings yet
- 2nd. AssessmentDocument61 pages2nd. AssessmentYunus ElonNo ratings yet
- Acute Cholangitis: Our Lady of Fatima UniversityDocument23 pagesAcute Cholangitis: Our Lady of Fatima UniversityMaria Paula Bungay100% (1)
- Case 1: Group 4Document26 pagesCase 1: Group 4John Joshua Lacson MedicineNo ratings yet
- Medical Surgical (MS) Rle Pulmonary/ Lung AssessmentDocument8 pagesMedical Surgical (MS) Rle Pulmonary/ Lung AssessmentYman Gio BumanglagNo ratings yet
- Penyakit Paru Obstruktif Kronik (PPOK) : Top Ten DiseaseDocument49 pagesPenyakit Paru Obstruktif Kronik (PPOK) : Top Ten DiseaseAldryn MuskananfolaNo ratings yet
- Respiratory System DisordersDocument353 pagesRespiratory System Disordersይደግ አብነውNo ratings yet
- CBD - CopdDocument51 pagesCBD - CopdBONG AIKCHINGNo ratings yet
- Pemeriksaan Fisik Sistem Pernapasan: Equipment NeededDocument78 pagesPemeriksaan Fisik Sistem Pernapasan: Equipment Neededsri karinaNo ratings yet
- Physiotherapy Assessment and Treatment On PICUDocument54 pagesPhysiotherapy Assessment and Treatment On PICUBatool Rehman100% (2)
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- A Review of A Case of A Patient Presenting With Low Back Pain Leading To A Low Back Emergency Managed in The Intensive Care Unit.Document57 pagesA Review of A Case of A Patient Presenting With Low Back Pain Leading To A Low Back Emergency Managed in The Intensive Care Unit.chadchimaNo ratings yet
- 2021 Lecture COPD & Asthma Full Size NotesDocument73 pages2021 Lecture COPD & Asthma Full Size NotesChelsea JiangNo ratings yet
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- Sleep ApneaDocument134 pagesSleep Apneakamal saud100% (1)
- Block 11 Tutorial Scenario C Mrs. A, A 29-Years Old House WifeDocument26 pagesBlock 11 Tutorial Scenario C Mrs. A, A 29-Years Old House Wiferio archuletaNo ratings yet
- Lungs and ThoraxDocument9 pagesLungs and ThoraxMaria Mika Ella RetizaNo ratings yet
- Synapse in My Pocket Neuro Exam & Localization - 1st Ed 2020Document63 pagesSynapse in My Pocket Neuro Exam & Localization - 1st Ed 2020SnowyNo ratings yet
- Please Focus On uWISE Questions As Your Main Study Material and You Can Use This Study Guide As A Reference. Female Reproductive PhysiologyDocument131 pagesPlease Focus On uWISE Questions As Your Main Study Material and You Can Use This Study Guide As A Reference. Female Reproductive PhysiologyhevinpatelNo ratings yet
- Obstetrics and Gynecology Module 4Document7 pagesObstetrics and Gynecology Module 4hevinpatel100% (1)
- Workshop #4 Internal Medicine IDocument78 pagesWorkshop #4 Internal Medicine IhevinpatelNo ratings yet
- OBGyn Endof Rotation OutlineDocument35 pagesOBGyn Endof Rotation OutlinehevinpatelNo ratings yet
- OBGyn Module 8Document9 pagesOBGyn Module 8hevinpatelNo ratings yet
- MHA 598 - Assignment #1Document4 pagesMHA 598 - Assignment #1hevinpatelNo ratings yet
- Workshop #5 Internal Medicine IIDocument77 pagesWorkshop #5 Internal Medicine IIhevinpatelNo ratings yet
- RMUPPC Module 3 Sinusitis and PneumoniaDocument11 pagesRMUPPC Module 3 Sinusitis and PneumoniahevinpatelNo ratings yet
- Methodist Health System Dallas Program: Residency Explorer™ ToolDocument8 pagesMethodist Health System Dallas Program: Residency Explorer™ ToolhevinpatelNo ratings yet
- Obstetrics and Gynecology Module 1 Hevinkumar PatelDocument12 pagesObstetrics and Gynecology Module 1 Hevinkumar PatelhevinpatelNo ratings yet
- Methodist Health System Dallas Program: Residency Explorer™ ToolDocument8 pagesMethodist Health System Dallas Program: Residency Explorer™ ToolhevinpatelNo ratings yet
- What Surprised You From The Videoconference and Why? What Could We Improve For The Next Video Conference?Document3 pagesWhat Surprised You From The Videoconference and Why? What Could We Improve For The Next Video Conference?hevinpatelNo ratings yet
- CPC Exam QuestionsDocument3 pagesCPC Exam QuestionshevinpatelNo ratings yet
- Toaz - Info Nbme 20 PDFPDF PRDocument200 pagesToaz - Info Nbme 20 PDFPDF PRhevinpatelNo ratings yet
- CPC Module 3 Sinusitis and PneumoniaDocument12 pagesCPC Module 3 Sinusitis and PneumoniahevinpatelNo ratings yet
- RMUPPC Module 1 Diabetes, Nutrition, Lab ResultsDocument6 pagesRMUPPC Module 1 Diabetes, Nutrition, Lab ResultshevinpatelNo ratings yet
- Module 12 Hematology and Oncology Hevinkumar PatelDocument24 pagesModule 12 Hematology and Oncology Hevinkumar PatelhevinpatelNo ratings yet
- CPC Exam Questions-2Document3 pagesCPC Exam Questions-2hevinpatelNo ratings yet
- Peds Outline 2Document20 pagesPeds Outline 2hevinpatelNo ratings yet
- Insulinoma Case PresentationDocument3 pagesInsulinoma Case PresentationhevinpatelNo ratings yet
- Module 9 Fluid and Electrolyte Management Hevinkumar PatelDocument5 pagesModule 9 Fluid and Electrolyte Management Hevinkumar PatelhevinpatelNo ratings yet
- Zdorovye - The Means To PrepareDocument4 pagesZdorovye - The Means To PrepareBrett DrinkwaterNo ratings yet
- Human Body Systems Essential VocabularyDocument6 pagesHuman Body Systems Essential Vocabularyapi-261172766No ratings yet
- URTIDocument2 pagesURTIYogeshRavalNo ratings yet
- The Ultimate Reviewer For Fundamentals of Nursing (Matt Vera)Document40 pagesThe Ultimate Reviewer For Fundamentals of Nursing (Matt Vera)josephmary09No ratings yet
- TB LarynxDocument3 pagesTB LarynxArunchandar VelusamyNo ratings yet
- MCQsDocument4 pagesMCQsSachin Singh100% (2)
- Comparative Anatomy of Respiratory SystemDocument129 pagesComparative Anatomy of Respiratory Systemgerman guazaNo ratings yet
- Respiration Rates ReportDocument8 pagesRespiration Rates Reportapi-284602266No ratings yet
- Narendra 2017Document13 pagesNarendra 2017Gundri FauziNo ratings yet
- L-4ff - 2/BME Date: 17/04/2022: Section-ADocument13 pagesL-4ff - 2/BME Date: 17/04/2022: Section-AHumyra HossainNo ratings yet
- Oropharyngeal and Nasotracheal SuctioningDocument2 pagesOropharyngeal and Nasotracheal SuctioningZoren CayananNo ratings yet
- English For Medicine Part 2 PDFDocument161 pagesEnglish For Medicine Part 2 PDFVictoria VintuNo ratings yet
- Physical AssessmentDocument5 pagesPhysical AssessmentLarr SumalpongNo ratings yet
- Pathology of The Lung: Djumadi AchmadDocument26 pagesPathology of The Lung: Djumadi AchmadVivi DeviyanaNo ratings yet
- Breathing & Exchange of Gases NotesDocument7 pagesBreathing & Exchange of Gases NotesKankana Biswas100% (1)
- Bansal Classes Biology ModulesDocument122 pagesBansal Classes Biology Modulesjia lissaNo ratings yet
- C19 SPACE ToolKit ChecklistsDocument8 pagesC19 SPACE ToolKit ChecklistsAdrian BălanNo ratings yet
- 3b. RhinoplastyDocument122 pages3b. RhinoplastyKamal Saud100% (2)
- Sci 5 SummativeDocument8 pagesSci 5 Summativemarion ildefonsoNo ratings yet
- Consenso EUR TQTDocument12 pagesConsenso EUR TQTCamila Villalobos BravoNo ratings yet
- Respiratory Physiology PostedDocument25 pagesRespiratory Physiology PostedYeni PuspitaNo ratings yet
- AutoflowDocument12 pagesAutoflowDaniela Merino FuentealbaNo ratings yet
- Nursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPDocument2 pagesNursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPLP Benoza100% (2)
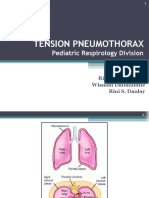
- Tension Pneumothorax: Pediatric Respirology DivisionDocument20 pagesTension Pneumothorax: Pediatric Respirology DivisionAan AlawiyahNo ratings yet
- PDF Pharmaceutical Inhalation Aerosol Technology Anthony J Hickey Ebook Full ChapterDocument53 pagesPDF Pharmaceutical Inhalation Aerosol Technology Anthony J Hickey Ebook Full Chaptershawn.auguste319100% (1)
- JAN-701-901 Instruction Manual PDFDocument508 pagesJAN-701-901 Instruction Manual PDFPiratsik OrbotanaNo ratings yet
- Edmark 2014Document9 pagesEdmark 2014Juampi FerrariNo ratings yet