Download as pptx, pdf, or txt
You might also like
- Prepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Document53 pagesPrepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Mir JavidNo ratings yet
- RNTCP Training Course For Program Manager Module 1 To 4Document208 pagesRNTCP Training Course For Program Manager Module 1 To 4Ashis DaskanungoNo ratings yet
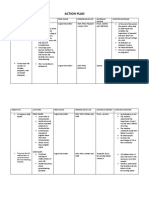
- Action PlanDocument4 pagesAction PlanJosette Mae Atanacio67% (3)
- Assessment To Compliance of Tuberculosis Treatment Among Tuberculosis PatientsDocument21 pagesAssessment To Compliance of Tuberculosis Treatment Among Tuberculosis PatientsabdulNo ratings yet
- Global Health Case Study CMHDocument6 pagesGlobal Health Case Study CMHapi-482580060No ratings yet
- Drug Resistance TBDocument27 pagesDrug Resistance TBpriyanka bhowmikNo ratings yet
- Directly Observed TreatmentDocument9 pagesDirectly Observed TreatmentNovelia CarolinNo ratings yet
- 82681-Article Text-199018-1-10-20121029Document8 pages82681-Article Text-199018-1-10-20121029sudirman efendiNo ratings yet
- Factors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsDocument14 pagesFactors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsAnonymous QPXAgjBwNo ratings yet
- Predictors of Tuberculosis (TBDocument11 pagesPredictors of Tuberculosis (TBchikomuezza19No ratings yet
- Baluchestan ProvinceDocument9 pagesBaluchestan ProvinceVincentius Michael WilliantoNo ratings yet
- Surveillance Evaluation Report of Tuberculosis in District Bhawalpur-2018 by DR Ammara TahirDocument22 pagesSurveillance Evaluation Report of Tuberculosis in District Bhawalpur-2018 by DR Ammara TahirSantosh WadhwaniNo ratings yet
- TB: Forgotten But Not GoneDocument55 pagesTB: Forgotten But Not GoneNational Press FoundationNo ratings yet
- Analisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanDocument14 pagesAnalisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanwahyuNo ratings yet
- Singh., 2020. Mekanisme Resistensi ObatDocument21 pagesSingh., 2020. Mekanisme Resistensi Obathasan andrianNo ratings yet
- The TB Patient Qualitative Evidence of Factors Affecting Compliance 2Document19 pagesThe TB Patient Qualitative Evidence of Factors Affecting Compliance 2musangobeni380No ratings yet
- Supraja Kanipakam Case Study SummaryDocument3 pagesSupraja Kanipakam Case Study Summaryapi-329758130No ratings yet
- Burden of Tuberculosis - Combating Drug Resistance: EditorialDocument3 pagesBurden of Tuberculosis - Combating Drug Resistance: EditorialmominamalikNo ratings yet
- BMC Research Notes: Research Article Open AccessDocument10 pagesBMC Research Notes: Research Article Open AccessRACHIDNo ratings yet
- Barriers and Facilitators To Adherence To Tuberculosis Treatment Among Drug Resistant TB Patients in GeorgiaDocument16 pagesBarriers and Facilitators To Adherence To Tuberculosis Treatment Among Drug Resistant TB Patients in GeorgiaCuratioCIFNo ratings yet
- Research On Prevalence of TB FinalDocument9 pagesResearch On Prevalence of TB FinalBontuNo ratings yet
- Tuberculosis Thesis TitleDocument5 pagesTuberculosis Thesis Titletjgyhvjef100% (2)
- WHO Bulletin 2005Document10 pagesWHO Bulletin 2005ajh2675No ratings yet
- Mjhid 6 1 E2014070Document8 pagesMjhid 6 1 E2014070Khoiril AnwarNo ratings yet
- Drug Resistance of TBDocument17 pagesDrug Resistance of TBGaurav Sharma100% (1)
- TB-Guidelines 2019 Final - 200619Document105 pagesTB-Guidelines 2019 Final - 200619Kalash SinghalNo ratings yet
- Molecular AnalysisDocument29 pagesMolecular AnalysisBaranishankarNo ratings yet
- TB DR MohabbatDocument27 pagesTB DR Mohabbatdr_hammadNo ratings yet
- Ofx 137Document7 pagesOfx 137Sheila Alcalde RNo ratings yet
- BMC Research Notes: Research Article Open AccessDocument10 pagesBMC Research Notes: Research Article Open Accessseptia mutiaraNo ratings yet
- New Developments in Tuberculosis Diagnosis and TreatmentDocument15 pagesNew Developments in Tuberculosis Diagnosis and TreatmentannewidiatmoNo ratings yet
- Recent Developments in The Diagnosis and Management of TuberculosisDocument8 pagesRecent Developments in The Diagnosis and Management of TuberculosisRhahahaNo ratings yet
- Ali2016 Article OutcomesOfTBTreatmentInHIVCo-iDocument9 pagesAli2016 Article OutcomesOfTBTreatmentInHIVCo-itishaNo ratings yet
- TB Complain Ce PM PJDocument8 pagesTB Complain Ce PM PJAnonymous QPXAgjBwNo ratings yet
- Research Article: Characteristics and Treatment Outcomes of Retreatment Tuberculosis Patients in BeninDocument7 pagesResearch Article: Characteristics and Treatment Outcomes of Retreatment Tuberculosis Patients in BeninfaustinaNo ratings yet
- BMJ m216 FullDocument18 pagesBMJ m216 Fulldiaspalma.medNo ratings yet
- Bao Et AlDocument7 pagesBao Et Alkang.asep008No ratings yet
- (2020) Treatment Outcome of Tuberculosis Treatment Regimens in Kandahar, AfghanistanDocument7 pages(2020) Treatment Outcome of Tuberculosis Treatment Regimens in Kandahar, AfghanistanBilal Ahmad RahimiNo ratings yet
- Pi Is 0261561423000250Document7 pagesPi Is 0261561423000250Rosul majeedNo ratings yet
- s12889 019 7980 XDocument12 pagess12889 019 7980 XYayew MaruNo ratings yet
- Epidemiology of Tuberculosis - UpToDateDocument33 pagesEpidemiology of Tuberculosis - UpToDateCentro de salud El quincheNo ratings yet
- Putra, 050 - 2901 - Nur Chayati - GalleyDocument10 pagesPutra, 050 - 2901 - Nur Chayati - GalleyHarumiNo ratings yet
- TB and Poverty: The Effect of Rifampicin-Resistant TB On Household IncomeDocument9 pagesTB and Poverty: The Effect of Rifampicin-Resistant TB On Household Incomestephenpillar1718No ratings yet
- Marzieh Shareizaei - Et.alDocument7 pagesMarzieh Shareizaei - Et.alkang.asep008No ratings yet
- 1201 Sanchez Padilla High Prevalence of Multidrug Resistant Tuberculosis Swaziland 2009 2010 Emerging Infectious Diseases 18 1Document9 pages1201 Sanchez Padilla High Prevalence of Multidrug Resistant Tuberculosis Swaziland 2009 2010 Emerging Infectious Diseases 18 1dewi ayu wulandariNo ratings yet
- BMC Public HealthDocument8 pagesBMC Public HealthAnselmo MatusseNo ratings yet
- 206560-Article Text-514620-1-10-20210429Document10 pages206560-Article Text-514620-1-10-20210429Odessa Fernandez DysangcoNo ratings yet
- J of Applied Microbiology - 2019 - Singh - Recent Updates On Drug Resistance in Mycobacterium TuberculosisDocument21 pagesJ of Applied Microbiology - 2019 - Singh - Recent Updates On Drug Resistance in Mycobacterium TuberculosisAnggun Millenia MuktiNo ratings yet
- Palagrism 4Document33 pagesPalagrism 4Mudasir UsmanNo ratings yet
- Pone 0194087 PDFDocument15 pagesPone 0194087 PDFInekeNo ratings yet
- Factsheet Hivtb UpdateDocument2 pagesFactsheet Hivtb UpdatedidirafaNo ratings yet
- 2017 Article 2662Document11 pages2017 Article 2662Dhani KurniawanNo ratings yet
- National Tuberculosis Control ProgramDocument4 pagesNational Tuberculosis Control ProgramSlepy chngNo ratings yet
- Use Only: Oral Anti-Tuberculosis Drugs: An Urgent Medication Reconciliation at Hospitals in IndonesiaDocument7 pagesUse Only: Oral Anti-Tuberculosis Drugs: An Urgent Medication Reconciliation at Hospitals in IndonesiaHeryanti PusparisaNo ratings yet
- IJTLDeditorial Protecting HCworkers Form TBDocument2 pagesIJTLDeditorial Protecting HCworkers Form TBRoma ParyaniNo ratings yet
- TB and HIVDocument62 pagesTB and HIVNational Press FoundationNo ratings yet
- Linezolid To Treat MDR-/XDR-tuberculosis: Available Evidence and Future ScenariosDocument5 pagesLinezolid To Treat MDR-/XDR-tuberculosis: Available Evidence and Future ScenariosNop PiromNo ratings yet
- Tuberculosis: An OverviewDocument45 pagesTuberculosis: An OverviewaNo ratings yet
- Rab 3Document8 pagesRab 3Belia DestamaNo ratings yet
- Survival Status and Treatment Outcome ofDocument6 pagesSurvival Status and Treatment Outcome ofEghar EverydayishellNo ratings yet
- Health Promotion ModelDocument8 pagesHealth Promotion ModelRobinson MurasiNo ratings yet
- Telemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.From EverandTelemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.No ratings yet
- LugobaDocument8 pagesLugobagabrielNo ratings yet
- Annual ReportDocument522 pagesAnnual ReportBetan Heath PostNo ratings yet
- Health Quarter 3 - Module 1 Health Trends, Issues and Concerns (Global Level)Document56 pagesHealth Quarter 3 - Module 1 Health Trends, Issues and Concerns (Global Level)Janice Cajepe67% (3)
- 100 Item MEDICAL SURGICAL Nursing ExaminationDocument18 pages100 Item MEDICAL SURGICAL Nursing ExaminationAijem Ryan100% (1)
- Resp System KoleyaDocument96 pagesResp System KoleyaAlberto MeroNo ratings yet
- Philip SebastianDocument33 pagesPhilip SebastianPhilip SebastianNo ratings yet
- Page-4 Ni 23 MarchDocument1 pagePage-4 Ni 23 MarchThingsulthliahNo ratings yet
- Kenia Afirca ResilienciaDocument7 pagesKenia Afirca ResilienciaBlanca PacsiNo ratings yet
- 761-Article Text-2181-1-10-20230217Document9 pages761-Article Text-2181-1-10-20230217ananda candraNo ratings yet
- DLP in Health 10 Global Health InitiativesDocument10 pagesDLP in Health 10 Global Health InitiativesJoshua MaravillasNo ratings yet
- AutoGenomics Intl-AACC, LADocument63 pagesAutoGenomics Intl-AACC, LAmohdkhairNo ratings yet
- Medical MCQ Center Tuberculosis MCQsDocument4 pagesMedical MCQ Center Tuberculosis MCQsBanu KubendiranNo ratings yet
- ORTHO Booklet 427-B1 FinalDocument226 pagesORTHO Booklet 427-B1 FinalMandisa Ndlovu Tenego0% (1)
- This Global TB Report Was Produced by A Core Team of 17 PeopleDocument11 pagesThis Global TB Report Was Produced by A Core Team of 17 Peopleevi novalitaNo ratings yet
- Tuberculosis Unit 1 Lecture - 1Document39 pagesTuberculosis Unit 1 Lecture - 1Kubra Rasool100% (3)
- Millennium Development GoalsDocument4 pagesMillennium Development GoalsMaria João BarrosNo ratings yet
- Anti TB PPT FinalDocument43 pagesAnti TB PPT FinalKeziah GillNo ratings yet
- JPETSTI Engver1 2Document56 pagesJPETSTI Engver1 2ilham rifaiNo ratings yet
- Jurnal Ssemi Fowler ErmaDocument11 pagesJurnal Ssemi Fowler ErmaLagee PukoNo ratings yet
- Key Activities in Rapid AssessmentDocument15 pagesKey Activities in Rapid AssessmentKewkew AzilearNo ratings yet
- Report of The Technical Consultation On Innovative Clinical Trial Designs For Evaluating New TB Preventive TreatmentsDocument59 pagesReport of The Technical Consultation On Innovative Clinical Trial Designs For Evaluating New TB Preventive TreatmentscarolNo ratings yet
- Female Genital Tuberculosis-PatelDocument37 pagesFemale Genital Tuberculosis-PatelLionel BaniquedNo ratings yet
- Academic Sessions: Date Topic Speaker Designation DepartmentDocument6 pagesAcademic Sessions: Date Topic Speaker Designation Departmentgoutham valapalaNo ratings yet
- COC Model Questions For Level IV PharmacyDocument9 pagesCOC Model Questions For Level IV Pharmacygemechu gebisa100% (2)
- Acsm Kap GuideDocument68 pagesAcsm Kap GuideFabienne GoutilleNo ratings yet
- Antitubercular AgentsDocument45 pagesAntitubercular Agentspallavi DiwareNo ratings yet
- RNTCP Guidelines Presentation, Gujarat, IndiaDocument22 pagesRNTCP Guidelines Presentation, Gujarat, IndiaDhaval BhawaniNo ratings yet
- English TB Paru SGD 9 Malika Sayyidina Azizah HakimDocument8 pagesEnglish TB Paru SGD 9 Malika Sayyidina Azizah HakimbruhwahatNo ratings yet