Download as pptx, pdf, or txt
You might also like
- OB-Gyn Case Presentation - BicornuateDocument53 pagesOB-Gyn Case Presentation - BicornuateZari Novela100% (1)
- TMJDocument38 pagesTMJAnonymous 6kAmeZzINo ratings yet
- Ectopic Pregnancy FINALDocument32 pagesEctopic Pregnancy FINALZak KazNo ratings yet
- Dela Torre Case Presentation South GenDocument44 pagesDela Torre Case Presentation South GenRalph Dale Dela TorreNo ratings yet
- Hydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaDocument80 pagesHydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaSheila Mary TanNo ratings yet
- Pap SmearDocument75 pagesPap SmearRaine BowNo ratings yet
- Placenta PreviaDocument36 pagesPlacenta Previaotartil_nimanNo ratings yet
- CMC Abruptio PlacentaDocument76 pagesCMC Abruptio PlacentaNorman Vryne CaduaNo ratings yet
- Bedside OutputDocument5 pagesBedside OutputREGENE KRIS SIMMONE GAMILNo ratings yet
- CC 19 Feb 2018 PEBDocument63 pagesCC 19 Feb 2018 PEBShinta Retno WulandariNo ratings yet
- Responsi DR EricDocument59 pagesResponsi DR EricMuhammad Edwin O MustofaNo ratings yet
- Kasus Perdarahan Post PartumDocument59 pagesKasus Perdarahan Post Partumnurul hidayahNo ratings yet
- AbortionDocument40 pagesAbortionSholen SamaritaNo ratings yet
- Case Presentation: Yousef Hassan Basman BazarDocument76 pagesCase Presentation: Yousef Hassan Basman BazarYousef Hassan BazarNo ratings yet
- Small Group Discussion NSDDocument96 pagesSmall Group Discussion NSDKittidej KaewruangNo ratings yet
- CC 13 Mar 2018 PEBDocument62 pagesCC 13 Mar 2018 PEBDhicky MaulanaNo ratings yet
- Module 4 Soap NoteDocument5 pagesModule 4 Soap Noteapi-539434803No ratings yet
- APPENDICITISDocument69 pagesAPPENDICITISKim Alvarez100% (1)
- PPT Case NephrolithiasisDocument45 pagesPPT Case NephrolithiasisRifka Anisa0% (1)
- Borang HSDDocument38 pagesBorang HSDFirdhaTriasuryaNo ratings yet
- Case Presentation and Discussion: Internal Medicine DepartmentDocument8 pagesCase Presentation and Discussion: Internal Medicine DepartmentCalingalan Hussin CaluangNo ratings yet
- M&M Hepatocellular CarcinomaDocument68 pagesM&M Hepatocellular Carcinomacharmaine BallanoNo ratings yet
- Name of Presentation: BymrxDocument60 pagesName of Presentation: BymrxFrancis Panes MaranianNo ratings yet
- Case Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DDocument18 pagesCase Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DKen StarNo ratings yet
- Lapjag 10 Maret 19Document2 pagesLapjag 10 Maret 19Bernardo Daniel LawrenciusNo ratings yet
- Case Presentat ION: Group No 2 Subgroup 2 Sec C Garge Shrikant Harish 33 Gunasekaran Janani 37 Kurpat Musthabeen 49Document27 pagesCase Presentat ION: Group No 2 Subgroup 2 Sec C Garge Shrikant Harish 33 Gunasekaran Janani 37 Kurpat Musthabeen 49Zedd ZorïNo ratings yet
- OB GYN CasePre FinalDocument82 pagesOB GYN CasePre FinalMarjorie Lahaylahay AlabataNo ratings yet
- Urogynecology Case: Parade of Surgery 2018Document10 pagesUrogynecology Case: Parade of Surgery 2018IMampu ZaharieNo ratings yet
- Screenshot 2023-02-19 at 11.11.49 AMDocument24 pagesScreenshot 2023-02-19 at 11.11.49 AMabdulrahmanNo ratings yet
- Pedia Case PresentationDocument59 pagesPedia Case PresentationincognitoNo ratings yet
- B6 - Surgery GS II Case IIDocument10 pagesB6 - Surgery GS II Case IIGregNo ratings yet
- Sample Case MgtemedDocument50 pagesSample Case MgtemedKenneth MiguelNo ratings yet
- Senior Interns GrandroundsDocument119 pagesSenior Interns GrandroundsNicko GranadoNo ratings yet
- Surgery Long Cases PrintDocument49 pagesSurgery Long Cases Printdrroshanshaji786No ratings yet
- Clinicopathologic Conference: Governor Celestino Gallares Memorial Hospital Department of Obstetrics and GynecologyDocument57 pagesClinicopathologic Conference: Governor Celestino Gallares Memorial Hospital Department of Obstetrics and GynecologyramwshNo ratings yet
- Inversio UteriDocument16 pagesInversio UteridellaNo ratings yet
- Burn Case StudyDocument15 pagesBurn Case StudyH MNo ratings yet
- Edited CapDocument81 pagesEdited CapSimon Peter MollanedaNo ratings yet
- TisonDocument29 pagesTisonvillaflorreinaNo ratings yet
- Pre-Res Case Presentation: Jo Anne N. Ramos, MDDocument72 pagesPre-Res Case Presentation: Jo Anne N. Ramos, MDKah Mote KyuNo ratings yet
- Sample Obstetric CaseDocument46 pagesSample Obstetric CasemelissaoljoyNo ratings yet
- OG CasesDocument82 pagesOG CasesgeethaNo ratings yet
- Postpartum Hemorrhage Due To Uterine AtonyDocument30 pagesPostpartum Hemorrhage Due To Uterine Atonymie_anum88% (8)
- Querol, Zachary Ivan G. - EAMC OB-GYNE CASE WRITE-UP 3Document8 pagesQuerol, Zachary Ivan G. - EAMC OB-GYNE CASE WRITE-UP 3zachary.ivan.querolNo ratings yet
- AGN PresentationDocument119 pagesAGN PresentationNikki GarlejoNo ratings yet
- Case 10Document1 pageCase 10alanjones3No ratings yet
- Gyn InfertilityDocument51 pagesGyn Infertilityayunisalleh100% (1)
- Ectopic PregnancyDocument54 pagesEctopic Pregnancypatriciaatan1497No ratings yet
- Massive TransfusionDocument104 pagesMassive Transfusionbingkydoodle1012No ratings yet
- TT Ket Ec Tim2 Jumaat-1Document19 pagesTT Ket Ec Tim2 Jumaat-1cuepNo ratings yet
- Case PresentationDocument49 pagesCase PresentationandikaprtmNo ratings yet
- Pages From First - Aid.for - The.obstetrics - And.gynecology - Clerkship.3rd - Ed-Ublog - TKDocument6 pagesPages From First - Aid.for - The.obstetrics - And.gynecology - Clerkship.3rd - Ed-Ublog - TKMahmoud MohsenNo ratings yet
- Case Study 29-APHDocument31 pagesCase Study 29-APHZarul Naim Mohd TamiziNo ratings yet
- Group 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariDocument35 pagesGroup 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariZedd ZorïNo ratings yet
- Ob CaseDocument46 pagesOb CasemelissaoljoyNo ratings yet
- Small Group DiscussionDocument78 pagesSmall Group DiscussionRose PeranteNo ratings yet
- Postterm PregnancyDocument48 pagesPostterm PregnancyrizaNo ratings yet
- Pre-Operative Conference: Presented By: Sarah Manaloto MDDocument20 pagesPre-Operative Conference: Presented By: Sarah Manaloto MDSarah ManalotoNo ratings yet
- ICP PPT 1Document27 pagesICP PPT 1SOWMYA GOTTIPALLINo ratings yet
- A Guide To House Officers in Surgery Casualty ReceptionDocument19 pagesA Guide To House Officers in Surgery Casualty ReceptionVinicio LabanoNo ratings yet
- Case Presentation: Prepared By: Erick Rafel Anca, M.DDocument121 pagesCase Presentation: Prepared By: Erick Rafel Anca, M.DErick AncaNo ratings yet
- Case Presentation: Residents-In-Charge: Dr. Gonzalez/Dr. Yusingbo/Dr. Bunyi Presented By: Intern Maria Cristina S. AmatDocument77 pagesCase Presentation: Residents-In-Charge: Dr. Gonzalez/Dr. Yusingbo/Dr. Bunyi Presented By: Intern Maria Cristina S. AmatErick AncaNo ratings yet
- Shock: Ron Michael N. Olaguera 2 Year Surgery ResidentDocument40 pagesShock: Ron Michael N. Olaguera 2 Year Surgery ResidentErick Anca100% (2)
- Case Presentation: Department of Obstetrics & Gynecology San Juan de Dios Educational Foundation, IncDocument98 pagesCase Presentation: Department of Obstetrics & Gynecology San Juan de Dios Educational Foundation, IncErick AncaNo ratings yet
- Case Presentation: Prepared By: Erick Rafel Anca, M.DDocument121 pagesCase Presentation: Prepared By: Erick Rafel Anca, M.DErick AncaNo ratings yet
- Types of CirculationDocument7 pagesTypes of Circulationhow are you?No ratings yet
- Effects of Transurethral Resection of Prostate (Turp) On Uroflowmetry Parameters On Patients Having Benign Prostatic HyperplasiaDocument6 pagesEffects of Transurethral Resection of Prostate (Turp) On Uroflowmetry Parameters On Patients Having Benign Prostatic HyperplasiaKamran AfzalNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- SPONDYLOLISTHESISDocument27 pagesSPONDYLOLISTHESISJulioYoko100% (1)
- DefibrillatorDocument22 pagesDefibrillatorKarthikeyan TNo ratings yet
- A Practical Approach To Obstetric AnesthesiaDocument1,401 pagesA Practical Approach To Obstetric AnesthesiaSarah FreyNo ratings yet
- Obstetrical Procedures 72Document3 pagesObstetrical Procedures 72Rosnalia HariyantoNo ratings yet
- Step-By-Step Approach To Endoscopic Cadaveric DissectionDocument205 pagesStep-By-Step Approach To Endoscopic Cadaveric DissectionJavier Gutiérrez CastilloNo ratings yet
- Avascular NecrosisDocument49 pagesAvascular NecrosisvhugalabudeliNo ratings yet
- Medscape and RadiopediaDocument21 pagesMedscape and RadiopediaRuhasri HumastutiNo ratings yet
- Dialysis TermsDocument2 pagesDialysis TermsmagillaniNo ratings yet
- Gallblad DER: ImagingDocument45 pagesGallblad DER: ImagingBohna FranciscoNo ratings yet
- Utility of Office Hysteroscopy in Diagnosing Retained Products of Conception Following Early Pregnancy Loss After in Vitro FertilizationDocument9 pagesUtility of Office Hysteroscopy in Diagnosing Retained Products of Conception Following Early Pregnancy Loss After in Vitro FertilizationAntonio JiménezNo ratings yet
- Recurrent Laryngeal Nerve Injury During Thyroidectomy - What NextDocument31 pagesRecurrent Laryngeal Nerve Injury During Thyroidectomy - What NextAnisur RahmanNo ratings yet
- Acodaduras Ureterales (Kinking)Document7 pagesAcodaduras Ureterales (Kinking)Clínica CIPRONo ratings yet
- Prevalence of Varicose Veins in Medical Heathcare Professionals Survey DocumentDocument13 pagesPrevalence of Varicose Veins in Medical Heathcare Professionals Survey Documentsanskruti.sonkamble00No ratings yet
- Shalakya Tantra-1 (Short Book) @bamsbooksinDocument197 pagesShalakya Tantra-1 (Short Book) @bamsbooksinಪ್ರಗತಿ. ಆರ್No ratings yet
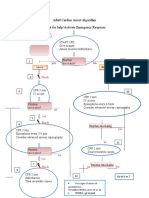
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocument1 pageAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMNo ratings yet
- Local Anesthetics 2019Document47 pagesLocal Anesthetics 20197s49sv4rmzNo ratings yet
- 5 Questions DR VryghemDocument1 page5 Questions DR VryghemDr. Jérôme C. VryghemNo ratings yet
- Iso 10555 5 2013Document9 pagesIso 10555 5 2013Katerin MartínezNo ratings yet
- ACS Parotidectomy PDFDocument10 pagesACS Parotidectomy PDFadel santosNo ratings yet
- Lesson 4 Circulatory System 2Document2 pagesLesson 4 Circulatory System 2Glaisa CudiaNo ratings yet
- Eye Problems in ChildrenDocument6 pagesEye Problems in ChildrenSachin CharodiNo ratings yet
- ENGLISH 7-Week3Document2 pagesENGLISH 7-Week3JERIZZA MAGNE PARAFINANo ratings yet
- Genital Tract InjuriesDocument24 pagesGenital Tract InjuriesManisha ThakurNo ratings yet
- Adv Tech Stand Neurosurg 2011 (37) 213Document31 pagesAdv Tech Stand Neurosurg 2011 (37) 213Emilia MoreiroNo ratings yet
- Unintentional Durotomy During Spinal Surgeries Performed by The Department of Neurosurgery, Abbasi Shaheed Hospital Karachi A Two Years Review StudyDocument1 pageUnintentional Durotomy During Spinal Surgeries Performed by The Department of Neurosurgery, Abbasi Shaheed Hospital Karachi A Two Years Review Studyapi-19502000No ratings yet
- AbbreviationsDocument3 pagesAbbreviationsJade Hemmings100% (1)