
COPD Management: Treatment, Pharmacological + Follow Up Rashk Kaushal 6 Course, grp:37
COPD Management: Treatment, Pharmacological + Follow Up Rashk Kaushal 6 Course, grp:37
You might also like
- QF3 Gastrointestinal DrugsDocument2 pagesQF3 Gastrointestinal DrugsNeil Feliciano Espiritu0% (1)
- BPOC in Medicina PrimaraDocument3 pagesBPOC in Medicina PrimaraAlina GheNo ratings yet
- Asthma, A Practical GuideDocument61 pagesAsthma, A Practical GuidePhaimNo ratings yet
- Chronic Obstructive Pulmonary Disease Case Study: QuestionsDocument7 pagesChronic Obstructive Pulmonary Disease Case Study: QuestionsMohammad KhalaylahNo ratings yet
- Exam 5 (Final Exam 23-25)Document19 pagesExam 5 (Final Exam 23-25)DoctorDrapionNo ratings yet
- Asthma Update: Thomas C. Bent, MD, FAAFP Infant, Child and Adolescent CourseDocument48 pagesAsthma Update: Thomas C. Bent, MD, FAAFP Infant, Child and Adolescent CourseSusie Marsick MartinNo ratings yet
- Copd ReportDocument69 pagesCopd ReportRadley Jed C. PelagioNo ratings yet
- Farmakoterapi Asma Dan COPD - 2Document32 pagesFarmakoterapi Asma Dan COPD - 2Camboy D' JablezNo ratings yet
- Pulmonary RehabilitationDocument41 pagesPulmonary RehabilitationAnandhu G100% (1)
- CopdDocument41 pagesCopdneelumshaukatNo ratings yet
- Asthma in Children My PresentationDocument49 pagesAsthma in Children My PresentationPutra Skate100% (3)
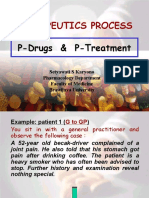
- Therapeutical ProcessDocument33 pagesTherapeutical ProcessecyzsiemoNo ratings yet
- End of Life, Palliative CareDocument35 pagesEnd of Life, Palliative CareFranz TariganNo ratings yet
- COPDDocument20 pagesCOPDعزالدين الزوقريNo ratings yet
- Case - Vii: AsthmaDocument18 pagesCase - Vii: AsthmaabubakarNo ratings yet
- Copd 2Document41 pagesCopd 2shrutik91No ratings yet
- Treatment of Schizophrenia and Management of Drug SideDocument83 pagesTreatment of Schizophrenia and Management of Drug SideAbelNo ratings yet
- Understanding Breathlessness in 10'ish Minutes!Document25 pagesUnderstanding Breathlessness in 10'ish Minutes!ناصر كشلافNo ratings yet
- PsikosomatikDocument65 pagesPsikosomatikHengki Permana PutraNo ratings yet
- Farmakoterapi Asma Dan COPDDocument32 pagesFarmakoterapi Asma Dan COPDArif StOneNo ratings yet
- Chronic Asthma Guidelines: in Adolescents & Adults 2007Document58 pagesChronic Asthma Guidelines: in Adolescents & Adults 2007Dark_loveNo ratings yet
- Drug AbuseDocument55 pagesDrug AbuseSujan AdhikariNo ratings yet
- Anti - Asthmatic Agents: Ana Marie R. Morelos, MD, DPPSDocument59 pagesAnti - Asthmatic Agents: Ana Marie R. Morelos, MD, DPPSRose AnnNo ratings yet
- Therapeutics Process: P-Drugs & P-TreatmentDocument35 pagesTherapeutics Process: P-Drugs & P-TreatmentdesyisrooNo ratings yet
- Clinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena AnjumDocument66 pagesClinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena Anjumgurrya786No ratings yet
- DetoxificationDocument85 pagesDetoxificationAce VisualsNo ratings yet
- AsthmaDocument28 pagesAsthmaJoel CanenciaNo ratings yet
- COPDDocument41 pagesCOPDsanalcrazy100% (3)
- Chronic Respiratory DisordersDocument41 pagesChronic Respiratory Disorderslady birdNo ratings yet
- III. Antipsychotic DrugsDocument31 pagesIII. Antipsychotic DrugsDanica AbarquezNo ratings yet
- Asthma & COPDDocument26 pagesAsthma & COPDraheenbushNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document12 pagesChronic Obstructive Pulmonary Disease (COPD)Marwan M.100% (1)
- ReportingDocument2 pagesReportingDeath WinterNo ratings yet
- End of Life CareDocument22 pagesEnd of Life CareMkindiNo ratings yet
- ERAS For Colorectal SurgeryDocument53 pagesERAS For Colorectal SurgeryJorge De VeraNo ratings yet
- Nausea Vomiting - DhitaDocument78 pagesNausea Vomiting - DhitaweNo ratings yet
- Toxicology in Critical Care: by Khairunnisa. Mansoor Instructor Acknowledgement: CCN TeamDocument28 pagesToxicology in Critical Care: by Khairunnisa. Mansoor Instructor Acknowledgement: CCN Teamshimama kanwalNo ratings yet
- Herbal Remedies For Otitis Media With Effusion (OME)Document21 pagesHerbal Remedies For Otitis Media With Effusion (OME)Tori Kehlani TanieluNo ratings yet
- Bronchial AsthmaDocument23 pagesBronchial AsthmaHermon WongNo ratings yet
- Chronic Obstructive Pulmonary Disease: Presented byDocument25 pagesChronic Obstructive Pulmonary Disease: Presented byChinni 12599No ratings yet
- Copd ExacerbationDocument42 pagesCopd Exacerbationأبوأحمد الحكيمNo ratings yet
- 0815 - Wednesday - Symptoms of Pulmonary Disease - BalterDocument34 pages0815 - Wednesday - Symptoms of Pulmonary Disease - Baltertechang1No ratings yet
- Connections: Nursing Practice ApplicationDocument3 pagesConnections: Nursing Practice ApplicationadadanNo ratings yet
- Chronic Obstructive Pulmonary Disease: Olga Alexeevna EfremovaDocument56 pagesChronic Obstructive Pulmonary Disease: Olga Alexeevna Efremovaسيف الشمريNo ratings yet
- End of Life Care PPPDocument43 pagesEnd of Life Care PPPElaine SUNo ratings yet
- Copd and Asthma FinalDocument26 pagesCopd and Asthma FinalRainer PoNo ratings yet
- Caring For The Client With Obstructive Pulmonary Disease: Pharmacologic PrinciplesDocument57 pagesCaring For The Client With Obstructive Pulmonary Disease: Pharmacologic PrinciplesgopscharanNo ratings yet
- Management of COPDDocument21 pagesManagement of COPDikrimahsbNo ratings yet
- Mood Disorders:: Identification and ManagementDocument45 pagesMood Disorders:: Identification and ManagementFikatu HugoronNo ratings yet
- DyspneaDocument13 pagesDyspneaIndri Noor HidayatiNo ratings yet
- Aap Ke Saath FinalDocument63 pagesAap Ke Saath FinalRaghubir DeNo ratings yet
- S3 2 Nurses and Chemotherapy - M. ReddahiDocument41 pagesS3 2 Nurses and Chemotherapy - M. Reddahicristina_zaharia865440No ratings yet
- The Care Plan (With An Overview of Medication Review) : Presented By: Maria Victoria B. WanceDocument22 pagesThe Care Plan (With An Overview of Medication Review) : Presented By: Maria Victoria B. WanceBlazy InhumangNo ratings yet
- Learning Material RLE NCM 112Document5 pagesLearning Material RLE NCM 112shiro the catNo ratings yet
- AsthmaDocument17 pagesAsthmashubhamz shaNo ratings yet
- Treating TB in AdultsDocument15 pagesTreating TB in AdultsMeenakshianandi KrishnanNo ratings yet
- Advance Clinical Nursing Presentation - SusanDocument40 pagesAdvance Clinical Nursing Presentation - SusanAbdul Hamid Al FarsiNo ratings yet
- ROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)Document45 pagesROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)rojosonNo ratings yet
- Aznan Lelo: Dep. Farmakologi & TerapeutikDocument36 pagesAznan Lelo: Dep. Farmakologi & Terapeutikrahmat feryadiNo ratings yet
- Managing Breathlessness in the CommunityFrom EverandManaging Breathlessness in the CommunityRating: 3.5 out of 5 stars3.5/5 (2)
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- 69 Haines Ely-Is Psoriasis A Bowel DiseaseDocument14 pages69 Haines Ely-Is Psoriasis A Bowel DiseaseJoe DoeNo ratings yet
- BPOC Si SDR MetabolicDocument29 pagesBPOC Si SDR MetabolicMarta DumitracheNo ratings yet
- Research PaperDocument22 pagesResearch PaperRocenne FernandezNo ratings yet
- (Ellie Lee) Abortion, Motherhood, and Mental HealtDocument302 pages(Ellie Lee) Abortion, Motherhood, and Mental HealtCamila PimentelNo ratings yet
- 300 Items NLE ReviewerDocument47 pages300 Items NLE Reviewercesspintas CuaresmaNo ratings yet
- Lesson Plan Health CDocument21 pagesLesson Plan Health CHannah BillonesNo ratings yet
- Review About Facts of Diabetes PDFDocument12 pagesReview About Facts of Diabetes PDFmifNo ratings yet
- Community Acquired Pneumonia, Lancet, 12-03Document11 pagesCommunity Acquired Pneumonia, Lancet, 12-03Maya ramadaniNo ratings yet
- Nausea and Vomiting in Adolescents and AdultsDocument30 pagesNausea and Vomiting in Adolescents and AdultsPramita Ines ParmawatiNo ratings yet
- Congestive - Cardiac-FailureDocument38 pagesCongestive - Cardiac-FailureAkhil R KrishnanNo ratings yet
- What Is NarcolepsyDocument1 pageWhat Is Narcolepsydata worksNo ratings yet
- Boyhood and BalanceDocument2 pagesBoyhood and Balanceapi-339039045No ratings yet
- Primer: ANCA-associated VasculitisDocument27 pagesPrimer: ANCA-associated VasculitisMedicinaNo ratings yet
- Textbook Introduction To Mediation Moderation and Conditional Process Analysis A Regression Based Approach Andrew F Hayes Ebook All Chapter PDFDocument54 pagesTextbook Introduction To Mediation Moderation and Conditional Process Analysis A Regression Based Approach Andrew F Hayes Ebook All Chapter PDFjames.stroud107100% (11)
- MSN Revised - Thea - For MergeDocument33 pagesMSN Revised - Thea - For Merge잔돈No ratings yet
- Communicable Diseases Control: November 2019Document128 pagesCommunicable Diseases Control: November 2019Henok TamiruNo ratings yet
- Cognitive-Behavioral Intervention in A Case of Self-MutilationDocument9 pagesCognitive-Behavioral Intervention in A Case of Self-MutilationMarinela MeliszekNo ratings yet
- 010 Pathology MCQ ACEM Primary Cell Injury 2Document3 pages010 Pathology MCQ ACEM Primary Cell Injury 2bmhsh100% (6)
- FavotriptanDocument12 pagesFavotriptansandyriaaaNo ratings yet
- AutoimmunityDocument40 pagesAutoimmunityKarl RobleNo ratings yet
- Hip and Buttock PainDocument26 pagesHip and Buttock PainEdy SetiawanNo ratings yet
- 1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamDocument4 pages1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamGeorgi GugicevNo ratings yet
- Cholesteatoma Report06Document3 pagesCholesteatoma Report06KatherineCentenoIlaganRNNo ratings yet
- Hypertensive CrisesDocument42 pagesHypertensive Crisescabinetuldeigiena0% (2)
- Reviewer Science Grade 9Document43 pagesReviewer Science Grade 9Earl AndreiNo ratings yet
- Clincial Quetsions Urinary and Bowel Reterntion Student VersionDocument4 pagesClincial Quetsions Urinary and Bowel Reterntion Student VersionDesha Gelles-SotoNo ratings yet
- A Brief Review in Dental Management of Medically Compromised PatientsDocument7 pagesA Brief Review in Dental Management of Medically Compromised PatientsMishellKarelisMorochoSegarraNo ratings yet
- English Final Paper TillyDocument7 pagesEnglish Final Paper Tillyapi-317278868No ratings yet
- Common Board QuestionsDocument2 pagesCommon Board QuestionsJonas Marvin AnaqueNo ratings yet





















































































Download as ppt, pdf, or txt
You might also like
- QF3 Gastrointestinal DrugsDocument2 pagesQF3 Gastrointestinal DrugsNeil Feliciano Espiritu0% (1)
- BPOC in Medicina PrimaraDocument3 pagesBPOC in Medicina PrimaraAlina GheNo ratings yet
- Asthma, A Practical GuideDocument61 pagesAsthma, A Practical GuidePhaimNo ratings yet
- Chronic Obstructive Pulmonary Disease Case Study: QuestionsDocument7 pagesChronic Obstructive Pulmonary Disease Case Study: QuestionsMohammad KhalaylahNo ratings yet
- Exam 5 (Final Exam 23-25)Document19 pagesExam 5 (Final Exam 23-25)DoctorDrapionNo ratings yet
- Asthma Update: Thomas C. Bent, MD, FAAFP Infant, Child and Adolescent CourseDocument48 pagesAsthma Update: Thomas C. Bent, MD, FAAFP Infant, Child and Adolescent CourseSusie Marsick MartinNo ratings yet
- Copd ReportDocument69 pagesCopd ReportRadley Jed C. PelagioNo ratings yet
- Farmakoterapi Asma Dan COPD - 2Document32 pagesFarmakoterapi Asma Dan COPD - 2Camboy D' JablezNo ratings yet
- Pulmonary RehabilitationDocument41 pagesPulmonary RehabilitationAnandhu G100% (1)
- CopdDocument41 pagesCopdneelumshaukatNo ratings yet
- Asthma in Children My PresentationDocument49 pagesAsthma in Children My PresentationPutra Skate100% (3)
- Therapeutical ProcessDocument33 pagesTherapeutical ProcessecyzsiemoNo ratings yet
- End of Life, Palliative CareDocument35 pagesEnd of Life, Palliative CareFranz TariganNo ratings yet
- COPDDocument20 pagesCOPDعزالدين الزوقريNo ratings yet
- Case - Vii: AsthmaDocument18 pagesCase - Vii: AsthmaabubakarNo ratings yet
- Copd 2Document41 pagesCopd 2shrutik91No ratings yet
- Treatment of Schizophrenia and Management of Drug SideDocument83 pagesTreatment of Schizophrenia and Management of Drug SideAbelNo ratings yet
- Understanding Breathlessness in 10'ish Minutes!Document25 pagesUnderstanding Breathlessness in 10'ish Minutes!ناصر كشلافNo ratings yet
- PsikosomatikDocument65 pagesPsikosomatikHengki Permana PutraNo ratings yet
- Farmakoterapi Asma Dan COPDDocument32 pagesFarmakoterapi Asma Dan COPDArif StOneNo ratings yet
- Chronic Asthma Guidelines: in Adolescents & Adults 2007Document58 pagesChronic Asthma Guidelines: in Adolescents & Adults 2007Dark_loveNo ratings yet
- Drug AbuseDocument55 pagesDrug AbuseSujan AdhikariNo ratings yet
- Anti - Asthmatic Agents: Ana Marie R. Morelos, MD, DPPSDocument59 pagesAnti - Asthmatic Agents: Ana Marie R. Morelos, MD, DPPSRose AnnNo ratings yet
- Therapeutics Process: P-Drugs & P-TreatmentDocument35 pagesTherapeutics Process: P-Drugs & P-TreatmentdesyisrooNo ratings yet
- Clinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena AnjumDocument66 pagesClinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena Anjumgurrya786No ratings yet
- DetoxificationDocument85 pagesDetoxificationAce VisualsNo ratings yet
- AsthmaDocument28 pagesAsthmaJoel CanenciaNo ratings yet
- COPDDocument41 pagesCOPDsanalcrazy100% (3)
- Chronic Respiratory DisordersDocument41 pagesChronic Respiratory Disorderslady birdNo ratings yet
- III. Antipsychotic DrugsDocument31 pagesIII. Antipsychotic DrugsDanica AbarquezNo ratings yet
- Asthma & COPDDocument26 pagesAsthma & COPDraheenbushNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document12 pagesChronic Obstructive Pulmonary Disease (COPD)Marwan M.100% (1)
- ReportingDocument2 pagesReportingDeath WinterNo ratings yet
- End of Life CareDocument22 pagesEnd of Life CareMkindiNo ratings yet
- ERAS For Colorectal SurgeryDocument53 pagesERAS For Colorectal SurgeryJorge De VeraNo ratings yet
- Nausea Vomiting - DhitaDocument78 pagesNausea Vomiting - DhitaweNo ratings yet
- Toxicology in Critical Care: by Khairunnisa. Mansoor Instructor Acknowledgement: CCN TeamDocument28 pagesToxicology in Critical Care: by Khairunnisa. Mansoor Instructor Acknowledgement: CCN Teamshimama kanwalNo ratings yet
- Herbal Remedies For Otitis Media With Effusion (OME)Document21 pagesHerbal Remedies For Otitis Media With Effusion (OME)Tori Kehlani TanieluNo ratings yet
- Bronchial AsthmaDocument23 pagesBronchial AsthmaHermon WongNo ratings yet
- Chronic Obstructive Pulmonary Disease: Presented byDocument25 pagesChronic Obstructive Pulmonary Disease: Presented byChinni 12599No ratings yet
- Copd ExacerbationDocument42 pagesCopd Exacerbationأبوأحمد الحكيمNo ratings yet
- 0815 - Wednesday - Symptoms of Pulmonary Disease - BalterDocument34 pages0815 - Wednesday - Symptoms of Pulmonary Disease - Baltertechang1No ratings yet
- Connections: Nursing Practice ApplicationDocument3 pagesConnections: Nursing Practice ApplicationadadanNo ratings yet
- Chronic Obstructive Pulmonary Disease: Olga Alexeevna EfremovaDocument56 pagesChronic Obstructive Pulmonary Disease: Olga Alexeevna Efremovaسيف الشمريNo ratings yet
- End of Life Care PPPDocument43 pagesEnd of Life Care PPPElaine SUNo ratings yet
- Copd and Asthma FinalDocument26 pagesCopd and Asthma FinalRainer PoNo ratings yet
- Caring For The Client With Obstructive Pulmonary Disease: Pharmacologic PrinciplesDocument57 pagesCaring For The Client With Obstructive Pulmonary Disease: Pharmacologic PrinciplesgopscharanNo ratings yet
- Management of COPDDocument21 pagesManagement of COPDikrimahsbNo ratings yet
- Mood Disorders:: Identification and ManagementDocument45 pagesMood Disorders:: Identification and ManagementFikatu HugoronNo ratings yet
- DyspneaDocument13 pagesDyspneaIndri Noor HidayatiNo ratings yet
- Aap Ke Saath FinalDocument63 pagesAap Ke Saath FinalRaghubir DeNo ratings yet
- S3 2 Nurses and Chemotherapy - M. ReddahiDocument41 pagesS3 2 Nurses and Chemotherapy - M. Reddahicristina_zaharia865440No ratings yet
- The Care Plan (With An Overview of Medication Review) : Presented By: Maria Victoria B. WanceDocument22 pagesThe Care Plan (With An Overview of Medication Review) : Presented By: Maria Victoria B. WanceBlazy InhumangNo ratings yet
- Learning Material RLE NCM 112Document5 pagesLearning Material RLE NCM 112shiro the catNo ratings yet
- AsthmaDocument17 pagesAsthmashubhamz shaNo ratings yet
- Treating TB in AdultsDocument15 pagesTreating TB in AdultsMeenakshianandi KrishnanNo ratings yet
- Advance Clinical Nursing Presentation - SusanDocument40 pagesAdvance Clinical Nursing Presentation - SusanAbdul Hamid Al FarsiNo ratings yet
- ROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)Document45 pagesROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)rojosonNo ratings yet
- Aznan Lelo: Dep. Farmakologi & TerapeutikDocument36 pagesAznan Lelo: Dep. Farmakologi & Terapeutikrahmat feryadiNo ratings yet
- Managing Breathlessness in the CommunityFrom EverandManaging Breathlessness in the CommunityRating: 3.5 out of 5 stars3.5/5 (2)
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- 69 Haines Ely-Is Psoriasis A Bowel DiseaseDocument14 pages69 Haines Ely-Is Psoriasis A Bowel DiseaseJoe DoeNo ratings yet
- BPOC Si SDR MetabolicDocument29 pagesBPOC Si SDR MetabolicMarta DumitracheNo ratings yet
- Research PaperDocument22 pagesResearch PaperRocenne FernandezNo ratings yet
- (Ellie Lee) Abortion, Motherhood, and Mental HealtDocument302 pages(Ellie Lee) Abortion, Motherhood, and Mental HealtCamila PimentelNo ratings yet
- 300 Items NLE ReviewerDocument47 pages300 Items NLE Reviewercesspintas CuaresmaNo ratings yet
- Lesson Plan Health CDocument21 pagesLesson Plan Health CHannah BillonesNo ratings yet
- Review About Facts of Diabetes PDFDocument12 pagesReview About Facts of Diabetes PDFmifNo ratings yet
- Community Acquired Pneumonia, Lancet, 12-03Document11 pagesCommunity Acquired Pneumonia, Lancet, 12-03Maya ramadaniNo ratings yet
- Nausea and Vomiting in Adolescents and AdultsDocument30 pagesNausea and Vomiting in Adolescents and AdultsPramita Ines ParmawatiNo ratings yet
- Congestive - Cardiac-FailureDocument38 pagesCongestive - Cardiac-FailureAkhil R KrishnanNo ratings yet
- What Is NarcolepsyDocument1 pageWhat Is Narcolepsydata worksNo ratings yet
- Boyhood and BalanceDocument2 pagesBoyhood and Balanceapi-339039045No ratings yet
- Primer: ANCA-associated VasculitisDocument27 pagesPrimer: ANCA-associated VasculitisMedicinaNo ratings yet
- Textbook Introduction To Mediation Moderation and Conditional Process Analysis A Regression Based Approach Andrew F Hayes Ebook All Chapter PDFDocument54 pagesTextbook Introduction To Mediation Moderation and Conditional Process Analysis A Regression Based Approach Andrew F Hayes Ebook All Chapter PDFjames.stroud107100% (11)
- MSN Revised - Thea - For MergeDocument33 pagesMSN Revised - Thea - For Merge잔돈No ratings yet
- Communicable Diseases Control: November 2019Document128 pagesCommunicable Diseases Control: November 2019Henok TamiruNo ratings yet
- Cognitive-Behavioral Intervention in A Case of Self-MutilationDocument9 pagesCognitive-Behavioral Intervention in A Case of Self-MutilationMarinela MeliszekNo ratings yet
- 010 Pathology MCQ ACEM Primary Cell Injury 2Document3 pages010 Pathology MCQ ACEM Primary Cell Injury 2bmhsh100% (6)
- FavotriptanDocument12 pagesFavotriptansandyriaaaNo ratings yet
- AutoimmunityDocument40 pagesAutoimmunityKarl RobleNo ratings yet
- Hip and Buttock PainDocument26 pagesHip and Buttock PainEdy SetiawanNo ratings yet
- 1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamDocument4 pages1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamGeorgi GugicevNo ratings yet
- Cholesteatoma Report06Document3 pagesCholesteatoma Report06KatherineCentenoIlaganRNNo ratings yet
- Hypertensive CrisesDocument42 pagesHypertensive Crisescabinetuldeigiena0% (2)
- Reviewer Science Grade 9Document43 pagesReviewer Science Grade 9Earl AndreiNo ratings yet
- Clincial Quetsions Urinary and Bowel Reterntion Student VersionDocument4 pagesClincial Quetsions Urinary and Bowel Reterntion Student VersionDesha Gelles-SotoNo ratings yet
- A Brief Review in Dental Management of Medically Compromised PatientsDocument7 pagesA Brief Review in Dental Management of Medically Compromised PatientsMishellKarelisMorochoSegarraNo ratings yet
- English Final Paper TillyDocument7 pagesEnglish Final Paper Tillyapi-317278868No ratings yet
- Common Board QuestionsDocument2 pagesCommon Board QuestionsJonas Marvin AnaqueNo ratings yet