Download as ppt, pdf, or txt
You might also like
- Infectious Diseases USMLE NotesDocument1 pageInfectious Diseases USMLE NotesDhanoush Mşđ33% (3)
- LeptospirosisDocument9 pagesLeptospirosisDeepu VijayaBhanuNo ratings yet
- ACOG Practice Bulletin No 82 Management Of.50Document10 pagesACOG Practice Bulletin No 82 Management Of.50Ccorita GuerraNo ratings yet
- Circulatory VectorDocument90 pagesCirculatory VectorHeavenNo ratings yet
- L1tojl Ophcu) bq8fDocument31 pagesL1tojl Ophcu) bq8fKristel AnneNo ratings yet
- Penyebab Virus - Flaviridae (Dengue)Document32 pagesPenyebab Virus - Flaviridae (Dengue)Bendy Dwi IrawanNo ratings yet
- Fever Synonym:: Modes of TransmissionDocument6 pagesFever Synonym:: Modes of TransmissionEjie Boy IsagaNo ratings yet
- 1.2 Leptospirosis Dengue Fever Malaria Filariais EncephalitisDocument95 pages1.2 Leptospirosis Dengue Fever Malaria Filariais Encephalitisesbercinio8528valNo ratings yet
- Communicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistDocument846 pagesCommunicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistGrn Mynjrkxz100% (1)
- TyphoidDocument67 pagesTyphoidArnel L. SanicoNo ratings yet
- Case Study of LeptospirosisDocument4 pagesCase Study of Leptospirosisbuzz Q75% (4)
- Leptospirosis Smt7Document34 pagesLeptospirosis Smt7hendra_darmawan_4No ratings yet
- Typhoid Fever: Infectious DiseaseDocument52 pagesTyphoid Fever: Infectious Disease12. Akshit Atwal100% (1)
- Senior Ila-Dengue Fever - 220210 - 004908Document69 pagesSenior Ila-Dengue Fever - 220210 - 004908Aimeenul AzfarNo ratings yet
- Child Care ModuleDocument6 pagesChild Care ModuleMiriam D. GutierrezNo ratings yet
- Gil P. Soriano, RN, MhpedDocument24 pagesGil P. Soriano, RN, MhpedGil Platon SorianoNo ratings yet
- Leptospirosis, Typhoid and Other FeversDocument37 pagesLeptospirosis, Typhoid and Other FeverskarageeNo ratings yet
- Communicable Disease FinalDocument16 pagesCommunicable Disease FinalPatziedawn Gonzalvo50% (2)
- Enterovirus & PoliomyelitisDocument17 pagesEnterovirus & PoliomyelitisAbdulsalam HashiNo ratings yet
- Case Study Leptospirosis PowerpointDocument17 pagesCase Study Leptospirosis Powerpointbeancent100% (2)
- Foot and Mouth DiseasesDocument9 pagesFoot and Mouth Diseaseseutamène ramziNo ratings yet
- Communicable Diseases: InfectiousDocument4 pagesCommunicable Diseases: InfectiousRichmond Catchillar BonusNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- Dengue AutosavedDocument12 pagesDengue AutosavedMaricris PallarNo ratings yet
- Case Discussion On Dengue Fever Dengue VirusDocument5 pagesCase Discussion On Dengue Fever Dengue VirusMichelle Vera GabunNo ratings yet
- Biological Warfare: Renaat A. A. M. Peleman, MD, PHD Dept Internal Med, Div Infect Dis University Hospital GhentDocument63 pagesBiological Warfare: Renaat A. A. M. Peleman, MD, PHD Dept Internal Med, Div Infect Dis University Hospital GhentAbdullah Al-RashedNo ratings yet
- Communicable DiseasesDocument7 pagesCommunicable DiseasesRaisa Robelle Quicho100% (1)
- Dengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueDocument6 pagesDengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueKatrina PonceNo ratings yet
- Leptospirosis: Nurul Hidayu - Nashriq Aiman - Audi AdibahDocument28 pagesLeptospirosis: Nurul Hidayu - Nashriq Aiman - Audi AdibahAkshay D'souzaNo ratings yet
- Arboviral Diseases and Dengue FinalDocument73 pagesArboviral Diseases and Dengue FinalBinayaNo ratings yet
- A Case HistoryDocument43 pagesA Case Historymel_pusagNo ratings yet
- Community Notes by DR - Khan Final-1Document44 pagesCommunity Notes by DR - Khan Final-1Aqib IshaqNo ratings yet
- Communicable DiseasesDocument6 pagesCommunicable DiseasesLory LynNo ratings yet
- Small Animal MedicineDocument262 pagesSmall Animal Medicinelijyohannesmekonnen7No ratings yet
- 7 - LeptospirosisDocument18 pages7 - LeptospirosisCAÑADA, JOHANNELYN M.No ratings yet
- Lepto Dan RabiesDocument69 pagesLepto Dan RabiesHiszom AsyhariNo ratings yet
- MeaslesDocument58 pagesMeaslesDr.P.NatarajanNo ratings yet
- Fever and RashDocument120 pagesFever and RashsamaNo ratings yet
- WITH Notes - COMMUNICABLE DISEASE - PROF. ARCHIE ALVIZ - HANDOUTSDocument8 pagesWITH Notes - COMMUNICABLE DISEASE - PROF. ARCHIE ALVIZ - HANDOUTScammel ramosNo ratings yet
- Leptospirosis: Dr. Doni Priambodo Wijisaksono Sppd-KptiDocument33 pagesLeptospirosis: Dr. Doni Priambodo Wijisaksono Sppd-KptiFarika NorNo ratings yet
- Leptospirosis 22Document2 pagesLeptospirosis 22Mhick SyNo ratings yet
- Fever Online SessionDocument51 pagesFever Online SessionPrecious ChaiNo ratings yet
- Dengue Fever: Thrombocytopenic Purpura"Document8 pagesDengue Fever: Thrombocytopenic Purpura"christian quiaoitNo ratings yet
- Chapter 3.4 Family SpirochaetaceaeDocument27 pagesChapter 3.4 Family SpirochaetaceaecimdesadesuNo ratings yet
- Lassa PresentationDocument53 pagesLassa PresentationOlagoke OlatunjiNo ratings yet
- Family Spirochaetaceae and Leptospiraceae-1Document29 pagesFamily Spirochaetaceae and Leptospiraceae-1temesgensemahegn55No ratings yet
- A Report On Dengue Hemorrhagic Fever: Submitted byDocument6 pagesA Report On Dengue Hemorrhagic Fever: Submitted byEjay ObarNo ratings yet
- Division of Infectious and Tropical Diseases, Department of Internal Medicine, University of Sumatera Utara/ Adam Malik Hospital, Medan, IndonesiaDocument18 pagesDivision of Infectious and Tropical Diseases, Department of Internal Medicine, University of Sumatera Utara/ Adam Malik Hospital, Medan, IndonesiaIndah PutriNo ratings yet
- Rabies ScribdDocument78 pagesRabies Scribdbryfar100% (1)
- Infectious DiseasesDocument140 pagesInfectious DiseasesSamah IzzNo ratings yet
- Commmon Communcable Diseases Affecting The Gastointestinal System Final-1Document113 pagesCommmon Communcable Diseases Affecting The Gastointestinal System Final-1fulolorenzNo ratings yet
- Pasteurelosis: The Disease Due ToDocument45 pagesPasteurelosis: The Disease Due Toclarentina aristawatiNo ratings yet
- MEASLESDocument34 pagesMEASLESImran KhanNo ratings yet
- LeptospirosisDocument40 pagesLeptospirosistummalapalli venkateswara rao86% (7)
- Viral Diseases - 06Document51 pagesViral Diseases - 06HIMANSHU SINGHNo ratings yet
- CD FinalDocument16 pagesCD FinalPatziedawn GonzalvoNo ratings yet
- Enteric VikrannthDocument71 pagesEnteric Vikrannthvikrannth vNo ratings yet
- Arthropod-Borne Virus 1-RirisDocument37 pagesArthropod-Borne Virus 1-Ririslutfia papitaNo ratings yet
- Espiratory Infections BitseatDocument90 pagesEspiratory Infections BitseatAhmed KitawNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- GRP1 Peurperal Mastitis CONCEPT MAPPINGDocument34 pagesGRP1 Peurperal Mastitis CONCEPT MAPPINGMada mada DaneNo ratings yet
- Bachelor of Science in Nursing: NCMB 312 - : Related Learning ExperienceDocument6 pagesBachelor of Science in Nursing: NCMB 312 - : Related Learning ExperienceMada mada DaneNo ratings yet
- Parkinso N'S Disease: Grou p1Document15 pagesParkinso N'S Disease: Grou p1Mada mada DaneNo ratings yet
- GASTRODocument47 pagesGASTROMada mada DaneNo ratings yet
- Course Task Lung Cancer MedsurgDocument2 pagesCourse Task Lung Cancer MedsurgMada mada DaneNo ratings yet
- NCMB 312 Rle Week 14 Dengue FeverDocument3 pagesNCMB 312 Rle Week 14 Dengue FeverMada mada DaneNo ratings yet
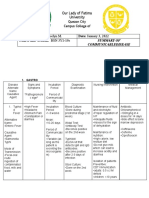
- Summary of CommunicablediseaseDocument31 pagesSummary of CommunicablediseaseMada mada DaneNo ratings yet
- Classic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyDocument5 pagesClassic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyTanveerNo ratings yet
- Severe Acute Respiratory SyndromeDocument12 pagesSevere Acute Respiratory SyndromeprincejeyarajpjsNo ratings yet
- UK Biologics Checklist May 2014Document2 pagesUK Biologics Checklist May 2014Dr Sneha's Skin and Allergy Clinic IndiaNo ratings yet
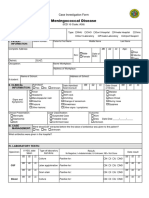
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- Tugas DR Vanda Covid 19 in Scuba DivingDocument2 pagesTugas DR Vanda Covid 19 in Scuba Divingfrd2c456ydNo ratings yet
- Chicken Pox ReportDocument25 pagesChicken Pox ReportDyanne Bautista100% (1)
- Mark Scheme (Results) May 2016: NQF BTEC Level 1/level 2 Firsts in Animal Care Unit 1: Animal Health (21883G)Document11 pagesMark Scheme (Results) May 2016: NQF BTEC Level 1/level 2 Firsts in Animal Care Unit 1: Animal Health (21883G)boho14No ratings yet
- Tugineyo Immaculate Faculty of Clinical Medicine and Dentistry Kampala International University Western Campus UgandaDocument15 pagesTugineyo Immaculate Faculty of Clinical Medicine and Dentistry Kampala International University Western Campus UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Daftar Penyakit Kompetensi 4ADocument12 pagesDaftar Penyakit Kompetensi 4ARoy Sandy PermanaNo ratings yet
- Vaccine-WPS OfficeDocument2 pagesVaccine-WPS OfficeJean FaustinoNo ratings yet
- Covid Letter - North Peace Seniors HousingDocument2 pagesCovid Letter - North Peace Seniors HousingAlaskaHighwayNewsNo ratings yet
- 5 Bacterial Infection and PathogenesisDocument31 pages5 Bacterial Infection and PathogenesisjakeyNo ratings yet
- Undulant Fever, Malta Fever, Mediterranean Fever, Enzootic Abortion, Epizootic Abortion, Contagious Abortion, Bang's DiseaseDocument31 pagesUndulant Fever, Malta Fever, Mediterranean Fever, Enzootic Abortion, Epizootic Abortion, Contagious Abortion, Bang's DiseaseanemenyeeNo ratings yet
- Microorganisms: What Is A Disease?Document8 pagesMicroorganisms: What Is A Disease?Rosa -No ratings yet
- HIVDocument56 pagesHIVenkinga67% (9)
- Case Study of GhulamDocument3 pagesCase Study of GhulamjanaNo ratings yet
- Arizona Communicable Disease FlipchartDocument98 pagesArizona Communicable Disease Flipchartapi-510866696No ratings yet
- Para Final ExamDocument18 pagesPara Final ExamLovely JeanNo ratings yet
- Parasite Infestation Tungiasis (Parasitologi)Document17 pagesParasite Infestation Tungiasis (Parasitologi)Aditya NobelNo ratings yet
- Uti PBL 2Document1 pageUti PBL 2Aliah ZuhairahNo ratings yet
- Vaccine Mandate PolicyDocument4 pagesVaccine Mandate PolicyLive 5 NewsNo ratings yet
- Neonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollDocument9 pagesNeonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollMarco Antonio Mendoza OjedaNo ratings yet
- Health FormDocument2 pagesHealth Formrhea engayNo ratings yet
- SADES18 DikonversiDocument90 pagesSADES18 DikonversiIc-tika Siee ChuabbieNo ratings yet
- Hiv Immunology Study CaseDocument7 pagesHiv Immunology Study Casetan choonNo ratings yet
- Expanded Program Immunization: NCM 104: Community Health Nursing I: Individual and FamilyDocument25 pagesExpanded Program Immunization: NCM 104: Community Health Nursing I: Individual and FamilyRica machells DaydaNo ratings yet
- Free Living Amoeba and CoccidiansDocument33 pagesFree Living Amoeba and CoccidiansGlanela ManalotoNo ratings yet
- Part5 RespiratoryDiseasesDocument4 pagesPart5 RespiratoryDiseasesAhmed HamdyNo ratings yet
- GiardiaDocument2 pagesGiardiaKristal ForteNo ratings yet