Download as pptx, pdf, or txt
You might also like
- Module 4 Maternal and Child Care NutritionDocument27 pagesModule 4 Maternal and Child Care NutritionmgllacunaNo ratings yet
- 141.0-81CO-797 CMM PDFDocument501 pages141.0-81CO-797 CMM PDFEngArab FqNo ratings yet
- 08 - Indications, Contraindications, Complications and Monitoring of enDocument13 pages08 - Indications, Contraindications, Complications and Monitoring of enbocah_britpopNo ratings yet
- L6 Water and Electrolyte BalanceDocument16 pagesL6 Water and Electrolyte BalancecuteNo ratings yet
- Action Against Hunger:: Acute Malnutrition BrochureDocument7 pagesAction Against Hunger:: Acute Malnutrition BrochureAction Against Hunger USA100% (1)
- Horn International University College: Colleege of Health ScienceDocument29 pagesHorn International University College: Colleege of Health Sciencekaise AbdiNo ratings yet
- ASPEN Critical Care - Susan BrantleyDocument44 pagesASPEN Critical Care - Susan BrantleyVitoria SilvaNo ratings yet
- Ipls PDFDocument119 pagesIpls PDFTekle TibebuNo ratings yet
- Biotransformation SeminarDocument16 pagesBiotransformation SeminarShreyasNo ratings yet
- 4.nutritional Requirement at Critical StagesDocument43 pages4.nutritional Requirement at Critical StagesBelayneh Tadesse100% (1)
- Hepatitis C: by DR Faiza SamadDocument44 pagesHepatitis C: by DR Faiza SamadMuhammad MakkiNo ratings yet
- English Diarrhea FixDocument20 pagesEnglish Diarrhea FixLa fazaNo ratings yet
- The Philippine Health Care SystemDocument3 pagesThe Philippine Health Care SystemMiki TroyoNo ratings yet
- Levelsofprevention 180123071404Document60 pagesLevelsofprevention 180123071404AJ Pascual AlonzoNo ratings yet
- Welcome To Community Medicine Dept ATBU BauchiDocument18 pagesWelcome To Community Medicine Dept ATBU BauchiYusuf Abdu MisauNo ratings yet
- Geriatric Giants Iwal 1 2020Document58 pagesGeriatric Giants Iwal 1 2020selymariaNo ratings yet
- Sam PDFDocument134 pagesSam PDFPunit Garg100% (2)
- Internship ReportDocument39 pagesInternship ReportHappy Sunshine50% (2)
- Introduction To Health Service ManagementDocument70 pagesIntroduction To Health Service ManagementephremNo ratings yet
- Community Based Management of Acute Malnutrition CMAM: Save The Children InternationalDocument68 pagesCommunity Based Management of Acute Malnutrition CMAM: Save The Children InternationalGeline Joy D. Samillano100% (1)
- Pharmaceutical CareDocument7 pagesPharmaceutical Caresomayya waliNo ratings yet
- Acute Nutrition PolicyDocument79 pagesAcute Nutrition PolicyyohaneskoNo ratings yet
- Diabetes Among HIV-Infected Patients On Antiretroviral Therapy at Mulago National Referral Hospital in Central UgandaDocument6 pagesDiabetes Among HIV-Infected Patients On Antiretroviral Therapy at Mulago National Referral Hospital in Central UgandaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Obesity and Iron Metabolism PDFDocument6 pagesObesity and Iron Metabolism PDFAhmed SobhNo ratings yet
- Syllabus Food AnalystDocument1 pageSyllabus Food AnalystKen SharmaNo ratings yet
- Types of AnemiaDocument8 pagesTypes of AnemiaApril Mae Magos LabradorNo ratings yet
- Question Bank - 3rd Prof, Part - II MbbsDocument174 pagesQuestion Bank - 3rd Prof, Part - II MbbsAnindya BiswasNo ratings yet
- CMAM Training PPT 2018 - 0Document57 pagesCMAM Training PPT 2018 - 0معلومة كيميائيةNo ratings yet
- Under Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Document10 pagesUnder Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Anonymous SMEU6r2No ratings yet
- Espen 2018 Paciente CriticoDocument117 pagesEspen 2018 Paciente CriticoCristina Correa SalazarNo ratings yet
- Araullo University FinalDocument19 pagesAraullo University FinalManzano JenecaNo ratings yet
- Nutritional Issues in The ICU Case FileDocument2 pagesNutritional Issues in The ICU Case Filehttps://medical-phd.blogspot.com100% (1)
- Magacyada Cudurada Iyo Waxa English Lagu Yiraahdo: Home Wararka Baargaal Maqaalo About Baargaal Nala Soo XiriirDocument6 pagesMagacyada Cudurada Iyo Waxa English Lagu Yiraahdo: Home Wararka Baargaal Maqaalo About Baargaal Nala Soo Xiriircankawaab100% (1)
- Concept of PreventionDocument48 pagesConcept of Preventionmahmoud100% (1)
- Anticancer Drugs NotesDocument112 pagesAnticancer Drugs Notesdnyanshri bhamareNo ratings yet
- Ashish Paliwal Rmncha PDFDocument83 pagesAshish Paliwal Rmncha PDFAshish PaliwalNo ratings yet
- Mini ProjectDocument12 pagesMini ProjectDaroo D.TNo ratings yet
- 2 Public Health For Primary Health CareDocument32 pages2 Public Health For Primary Health CarehervwNo ratings yet
- Introduction To HematologyDocument61 pagesIntroduction To HematologyThis is PonyNo ratings yet
- TPN Protocol HandoutDocument2 pagesTPN Protocol Handoutapi-610233914No ratings yet
- Nematode Infections 2019 Student PDFDocument272 pagesNematode Infections 2019 Student PDFCharlene SuliganNo ratings yet
- Medicine and Nutrition Case StudyDocument5 pagesMedicine and Nutrition Case Studyapi-384113918No ratings yet
- IGNOU Block 1 Unit 6 Bio-Medical Waste Management & Infection ControlDocument20 pagesIGNOU Block 1 Unit 6 Bio-Medical Waste Management & Infection Controlerice.research100% (1)
- Perinatal InfectionsDocument24 pagesPerinatal InfectionsAlexandra OanaNo ratings yet
- Applied Nutrition Unit 01-1Document36 pagesApplied Nutrition Unit 01-1Hira KhanNo ratings yet
- MNT For ObesityDocument45 pagesMNT For ObesitySyafiraaanlt 18No ratings yet
- Phulping Danda VDCDocument125 pagesPhulping Danda VDCSabaldgreat100% (1)
- Factors Impacting The Future Practice of Physiotherapy in CanadaDocument16 pagesFactors Impacting The Future Practice of Physiotherapy in Canadawasim.imiNo ratings yet
- Fluid and Electrolyte Imbalance QuizDocument2 pagesFluid and Electrolyte Imbalance QuizteabagmanNo ratings yet
- Nebiyu Proposal HIV AND NUTRTIONDocument28 pagesNebiyu Proposal HIV AND NUTRTIONBinkisa BilloNo ratings yet
- Nutrition in ICU: Enteral NutritionDocument24 pagesNutrition in ICU: Enteral NutritionMahenderaNo ratings yet
- CMAM Training PPT 2018 - 0Document57 pagesCMAM Training PPT 2018 - 0cabdinuux32100% (1)
- Pharmaceutics I Theory and Practical ForDocument21 pagesPharmaceutics I Theory and Practical ForNitin SharmaNo ratings yet
- Case Study 1Document4 pagesCase Study 1Maddah Hussain100% (1)
- Important Topics To Study For Fmge Exam: AnaesthesiaDocument11 pagesImportant Topics To Study For Fmge Exam: AnaesthesiaPrepladder ChyNo ratings yet
- Hepatoprotective ActivityDocument27 pagesHepatoprotective ActivityBilly Aditya PratamaNo ratings yet
- Indication For Insulin TX in Dm2Document28 pagesIndication For Insulin TX in Dm2Nishad BnNo ratings yet
- Foundational Knowledge for the Practice of Family Medicine in West AfricaFrom EverandFoundational Knowledge for the Practice of Family Medicine in West AfricaRating: 5 out of 5 stars5/5 (1)
- ScrewCompressors XRV204 SpecSheet DigitalDocument1 pageScrewCompressors XRV204 SpecSheet DigitalBarros Arias EnriqueNo ratings yet
- The Problem of Increasing Human Energy - Nikola Tesla PDFDocument27 pagesThe Problem of Increasing Human Energy - Nikola Tesla PDFKarhys100% (2)
- Honda City Vs Toyota CorollaDocument1 pageHonda City Vs Toyota CorollaMuhammad Sheharyar MohsinNo ratings yet
- DR - Nitish Kumar - CV ..Document6 pagesDR - Nitish Kumar - CV ..ABHISHEK SINGHNo ratings yet
- Replication and Disaster Recovery Administration Guide: Hitachi Unified NAS Module Hitachi NAS Platform Release 12.7Document97 pagesReplication and Disaster Recovery Administration Guide: Hitachi Unified NAS Module Hitachi NAS Platform Release 12.7PrasadValluraNo ratings yet
- Dewalt dw806 Manual PDFDocument28 pagesDewalt dw806 Manual PDFsanprojectNo ratings yet
- Pharmacological Studies of Ocimum Basilicum L.Document7 pagesPharmacological Studies of Ocimum Basilicum L.Baru Chandrasekhar RaoNo ratings yet
- Embediment LengthDocument6 pagesEmbediment LengthkelvinNo ratings yet
- LOC Taxed Under ITADocument3 pagesLOC Taxed Under ITARizhatul AizatNo ratings yet
- CAMBODIAN Temple Designs-And Hindu Cosmology-: DR Uday DokrasDocument15 pagesCAMBODIAN Temple Designs-And Hindu Cosmology-: DR Uday DokrasUday DokrasNo ratings yet
- Pulmonary ThromboembolismDocument61 pagesPulmonary ThromboembolismsanjivdasNo ratings yet
- Obesidade 2023Document69 pagesObesidade 2023Belinha DonattiNo ratings yet
- FRB13089887411Document4 pagesFRB13089887411MAHA KAALNo ratings yet
- IB Annual Financial InformationDocument458 pagesIB Annual Financial InformationazaiahNo ratings yet
- Ddpa 3092 Reaction of A Continuous BeamDocument4 pagesDdpa 3092 Reaction of A Continuous Beamnurlisa khaleedaNo ratings yet
- Halrev: Sistem Hukum Dan Teori Hukum ChaosDocument11 pagesHalrev: Sistem Hukum Dan Teori Hukum ChaosPUSATSTUDI RMIKNo ratings yet
- LPP - orDocument12 pagesLPP - orbharat_v79No ratings yet
- BSBSTR601 Student Project PortfolioDocument11 pagesBSBSTR601 Student Project PortfolioAmra Ali AliNo ratings yet
- Peripheral Testosterone MetabolismDocument8 pagesPeripheral Testosterone MetabolismAgung SentosaNo ratings yet
- Bearings - Boston GearDocument7 pagesBearings - Boston GearJames GreenNo ratings yet
- Activation PDFDocument270 pagesActivation PDFPedro Ruiz MedianeroNo ratings yet
- Kraftwerks K Series Race Supercharger Kit (C38) K Series PartsDocument1 pageKraftwerks K Series Race Supercharger Kit (C38) K Series PartsAndres GigenaNo ratings yet
- Individual Report 23001Document5 pagesIndividual Report 23001Ashley MartinezNo ratings yet
- K Tron Product Specification K SFT III Smart ForceDocument2 pagesK Tron Product Specification K SFT III Smart ForcesamirNo ratings yet
- Sample Report Teenager Not SIDocument13 pagesSample Report Teenager Not SIpenny van deer waltNo ratings yet
- 2.3 Routine, Good News and Good Will MessagesDocument20 pages2.3 Routine, Good News and Good Will MessagesSyed Zubair AliNo ratings yet
- Jab Chem Nat 5 Question Banks All ExamsDocument55 pagesJab Chem Nat 5 Question Banks All ExamsHariNo ratings yet
- Ford 970Document4 pagesFord 970amanNo ratings yet
- AHF Thesis - CorrectedDocument146 pagesAHF Thesis - CorrectedAlasdair FikourasNo ratings yet
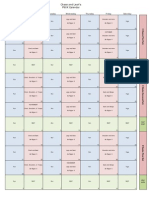
- CalendarDocument1 pageCalendarfattyfeet5No ratings yet