Download as pptx, pdf, or txt
You might also like
- Case Scenario For Community Health NursingDocument5 pagesCase Scenario For Community Health Nursinghemihema100% (1)
- Acid-Base Disorder CasesDocument40 pagesAcid-Base Disorder CaseslrostomeNo ratings yet
- 1 Coagulation Disorderin PregnancyDocument21 pages1 Coagulation Disorderin PregnancyIntan Nursiani AgnurNo ratings yet
- AIIMS (MBBS) Solved Question Paper 2010Document34 pagesAIIMS (MBBS) Solved Question Paper 2010cbsestudymaterialsNo ratings yet
- Git MCQ Valume DDocument39 pagesGit MCQ Valume DAhmed ElwassiefNo ratings yet
- Written Exam Blue PrintDocument12 pagesWritten Exam Blue PrintMotasim_mNo ratings yet
- GNS 312 Complete QuestionDocument164 pagesGNS 312 Complete QuestionAdebayo Yusuff AdesholaNo ratings yet
- The Urinary SystemDocument91 pagesThe Urinary SystemKiko A100% (1)
- Body FluidsDocument24 pagesBody FluidsMohamed MidoNo ratings yet
- A Brief Overview of Hemoglobin ElectrophoresisDocument46 pagesA Brief Overview of Hemoglobin Electrophoresisمجاهد إسماعيل حسن حسينNo ratings yet
- MCQSDocument25 pagesMCQSkays30002403No ratings yet
- MED2031 Mid Semester 1 Practice ExaminationDocument29 pagesMED2031 Mid Semester 1 Practice ExaminationTyler VargasNo ratings yet
- Arterial Blood Gas AnalysisDocument32 pagesArterial Blood Gas AnalysisPradip ChougaleNo ratings yet
- Blood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIDocument39 pagesBlood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIIQBAL HAKKIKINo ratings yet
- Abg PPT NewDocument69 pagesAbg PPT NewMalaka Atapattu100% (3)
- Acid Base Disorders For Vet. StudentsDocument43 pagesAcid Base Disorders For Vet. StudentsAli H. Sadiek أ.د. علي حسن صديق100% (2)
- Acid BaseDocument89 pagesAcid BaseEdouinaNo ratings yet
- ABG MMHG InterpretationDocument92 pagesABG MMHG InterpretationManmeet SNo ratings yet
- ABGS Arterial Blood GasesDocument27 pagesABGS Arterial Blood GasesMuhammad asif samiNo ratings yet
- Acid-Base Balance PDFDocument10 pagesAcid-Base Balance PDFinah krizia lague100% (1)
- Acid - Base BalanceDocument38 pagesAcid - Base BalanceDianne EstradaNo ratings yet
- Acid-Base BalanceDocument7 pagesAcid-Base BalanceMichelle Mae JulianaNo ratings yet
- Fluid-Electrolytes and Acid-Base Disturbance in Surgery: Haidi Hu, MD, PHDDocument68 pagesFluid-Electrolytes and Acid-Base Disturbance in Surgery: Haidi Hu, MD, PHDHUNEL KimNo ratings yet
- Acid Base Disorders - Lecture 45Document14 pagesAcid Base Disorders - Lecture 45yassin mostafaNo ratings yet
- Maimun Zulhaidah A Tinny R Indra Clinical Pathology DeptDocument47 pagesMaimun Zulhaidah A Tinny R Indra Clinical Pathology DeptSunny AghniNo ratings yet
- Acid-Base BalanceDocument47 pagesAcid-Base BalanceEmmanuel RocksonNo ratings yet
- Arterial Blood Gas AnalysisDocument43 pagesArterial Blood Gas AnalysisLoribel Coma100% (1)
- Arterial-Blood Gas AnalysisDocument49 pagesArterial-Blood Gas AnalysisGovernance Book100% (1)
- Arterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfDocument64 pagesArterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfArmaanjeet SinghNo ratings yet
- Abg - MLT 4th Semester.Document146 pagesAbg - MLT 4th Semester.Sanjeev walvekarNo ratings yet
- Acid Base Disorders-MD3Document44 pagesAcid Base Disorders-MD3juliuskahabi1No ratings yet
- Lecture 2 - Fluid & Electrolyre Balance 2021Document28 pagesLecture 2 - Fluid & Electrolyre Balance 2021عمار عاشورNo ratings yet
- Saumya Gupta Moderator: Dr. Vishal GuptaDocument41 pagesSaumya Gupta Moderator: Dr. Vishal Guptaimranqazi11No ratings yet
- Lecture 2. Acid Base DisordesDocument62 pagesLecture 2. Acid Base DisordesPharmswipe KenyaNo ratings yet
- Blood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIDocument39 pagesBlood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSISalsabila RahmaNo ratings yet
- Acid - Base Balance & Abg AnalysisDocument71 pagesAcid - Base Balance & Abg AnalysisMohan KrishnaNo ratings yet
- Acid Base BalanceDocument45 pagesAcid Base BalanceSameer Ul BashirNo ratings yet
- Acid Base BalanceDocument17 pagesAcid Base BalanceayeshaNo ratings yet
- Acid Base Imbalance Final PresentationDocument18 pagesAcid Base Imbalance Final PresentationElla PaezNo ratings yet
- Acid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManDocument68 pagesAcid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManKeshia Joyce LimNo ratings yet
- Arterial Blood Gas AnalysisDocument6 pagesArterial Blood Gas AnalysisMaribee Tagayun EspirituNo ratings yet
- Audio 2021 03 29 12 31 31Document41 pagesAudio 2021 03 29 12 31 31wafaa moNo ratings yet
- Blood Gas AnalysisDocument39 pagesBlood Gas Analysisjtalan9No ratings yet
- Acid Base Balance 2022 NewDocument97 pagesAcid Base Balance 2022 New4tqpxmts7zNo ratings yet
- Acid Base Disorders: Mr. Ahmed Alnaji Mbchb. Mrcs 1+2 Palestinian Board G. Surgery European Gaza HospitalDocument60 pagesAcid Base Disorders: Mr. Ahmed Alnaji Mbchb. Mrcs 1+2 Palestinian Board G. Surgery European Gaza Hospitalpt.mahmoudNo ratings yet
- Physiology of Acid Base Balance by Dr. ROOMIDocument70 pagesPhysiology of Acid Base Balance by Dr. ROOMIMudassar Roomi100% (1)
- Acid-Base DisordersDocument35 pagesAcid-Base DisordersAnonymous eson90100% (2)
- Acid-Base Balance and BurnsDocument9 pagesAcid-Base Balance and Burnsjelly beanNo ratings yet
- Screenshot 2022-08-25 at 9.35.50 PMDocument77 pagesScreenshot 2022-08-25 at 9.35.50 PMaswathy yesodharanNo ratings yet
- Acid Base Disorders: Hasan Al-Dorzi, MD Pulmonary and Critical Care Consultant, Intensive Care DepartmentDocument47 pagesAcid Base Disorders: Hasan Al-Dorzi, MD Pulmonary and Critical Care Consultant, Intensive Care DepartmentAmjaSaudNo ratings yet
- ABGSDocument28 pagesABGSShafiq Ur RahmanNo ratings yet
- 2016 Acid Base DisordersDocument48 pages2016 Acid Base DisordersbellabelbonNo ratings yet
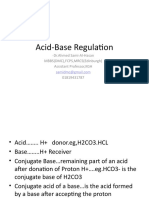
- Acid-Base Regulation: - DR - Ahmed Sami-Al-Hasan MBBS (DMC), FCPS, MRCS (Edinburgh) Assistant Professor, KGH 01819431787Document59 pagesAcid-Base Regulation: - DR - Ahmed Sami-Al-Hasan MBBS (DMC), FCPS, MRCS (Edinburgh) Assistant Professor, KGH 01819431787Inzamamul Haque ShihabNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasRathis Dasan100% (1)
- Screenshot 2024-04-02 at 10.36.50 PMDocument98 pagesScreenshot 2024-04-02 at 10.36.50 PMfalahattari12No ratings yet
- ABG ElectrolytesDocument48 pagesABG ElectrolytesDRwaqas Gulzar100% (1)
- Final MCW .ABDpptxDocument124 pagesFinal MCW .ABDpptxFazlul KarimNo ratings yet
- Blood GasesDocument51 pagesBlood Gasesrbm121415chyNo ratings yet
- Acid-Base Disorders NotesDocument10 pagesAcid-Base Disorders NotesLovely100% (1)
- Arterial Blood Gas AnalysisDocument32 pagesArterial Blood Gas AnalysisPervinNo ratings yet
- Abg SakshiDocument59 pagesAbg SakshiSakshi GuptaNo ratings yet
- Gout & Pseudogout: Chemical PathologyDocument9 pagesGout & Pseudogout: Chemical PathologyVivian KamaraNo ratings yet
- Endocrine: Mo GbessayDocument88 pagesEndocrine: Mo GbessayVivian KamaraNo ratings yet
- Calcium, Phosphate and MagnesiumDocument36 pagesCalcium, Phosphate and MagnesiumVivian Kamara100% (1)
- Arenaviridae: Third Year Notes DR Sulaiman ContehDocument253 pagesArenaviridae: Third Year Notes DR Sulaiman ContehVivian KamaraNo ratings yet
- Concepts in Chemical PathologyDocument41 pagesConcepts in Chemical PathologyVivian KamaraNo ratings yet
- Chem Path Introduction - Year 3.-1Document55 pagesChem Path Introduction - Year 3.-1Vivian KamaraNo ratings yet
- Filariasis Report (NCM 55 - B3)Document21 pagesFilariasis Report (NCM 55 - B3)Jette Charmae OlboNo ratings yet
- Microbial KeratitisDocument2 pagesMicrobial KeratitisNehal SonawaneNo ratings yet
- DAFTAR PUSTAKA PanhipopituitarismDocument2 pagesDAFTAR PUSTAKA PanhipopituitarismNoEr FitRiaNo ratings yet
- Product List - PCR AND ELISA - 2022 - V2 EN - Doc13672 1Document36 pagesProduct List - PCR AND ELISA - 2022 - V2 EN - Doc13672 1Edgar Fernando Sánchez BribiescaNo ratings yet
- 8 TCCC Scenarios IgDocument35 pages8 TCCC Scenarios Igherbert rogan0% (1)
- Project On UTIDocument34 pagesProject On UTIZulqarnain AslamNo ratings yet
- Ajodo MarpeDocument11 pagesAjodo MarpePuttnaree Nite100% (1)
- Gastroesophageal Reflux DiseaseDocument18 pagesGastroesophageal Reflux Diseasebrian3442No ratings yet
- Brochure Muscular DystrophyDocument3 pagesBrochure Muscular DystrophyDotticaDottisha TaylorNo ratings yet
- Case StudyDocument4 pagesCase StudyEdenNo ratings yet
- Automated Contrast Injectors For AngiogrDocument6 pagesAutomated Contrast Injectors For AngiogrAditya MadhavpeddiNo ratings yet
- BD TubesDocument6 pagesBD TubesdbNo ratings yet
- AsthmaDocument20 pagesAsthmablessed23No ratings yet
- Presentation 1 - DR Martin RoyleDocument66 pagesPresentation 1 - DR Martin Royleশরীফ উল কবীরNo ratings yet
- Form Stok Opname R ObatDocument3 pagesForm Stok Opname R Obatbernadetta ayuNo ratings yet
- Guidelines For The National Implementation of Dengue Rapid Diagnostic Test (RDT)Document13 pagesGuidelines For The National Implementation of Dengue Rapid Diagnostic Test (RDT)Billy John F. Lebosada100% (1)
- Headache History TakingDocument5 pagesHeadache History TakingRao Rizwan Shakoor0% (1)
- Final Synopsis PHDDocument13 pagesFinal Synopsis PHDKishor KanaseNo ratings yet
- Betahistine Dihidrochloride Betahistin MesilateDocument8 pagesBetahistine Dihidrochloride Betahistin MesilateApotek SuryaNo ratings yet
- Ectatic ConditionsDocument11 pagesEctatic ConditionsShuvashishSunuwarNo ratings yet
- Hypertension ReportDocument16 pagesHypertension ReportAxl SalimoNo ratings yet
- 1755Document43 pages1755modestusNo ratings yet
- Myofascial Trigger Points - Pathophysiology and Evidence-Informed Diagnosis and Management (Contemporary Issues in Physical Therapy and Rehabilitation Medicine) (PDFDrive)Document306 pagesMyofascial Trigger Points - Pathophysiology and Evidence-Informed Diagnosis and Management (Contemporary Issues in Physical Therapy and Rehabilitation Medicine) (PDFDrive)Christine DiVirgilioNo ratings yet
- Brochure C.a.T.S.plusDocument4 pagesBrochure C.a.T.S.plusvampire_bdgNo ratings yet
- Healthy Knees: Manual On Knee Pain and Different Therapeutic ApproachesDocument37 pagesHealthy Knees: Manual On Knee Pain and Different Therapeutic Approachesdaniel70_7No ratings yet
- Overview of Critical Care NursingDocument23 pagesOverview of Critical Care NursingMalak AbdullahNo ratings yet
- Patient Assistance Reimbursement Guide 2019Document93 pagesPatient Assistance Reimbursement Guide 2019Matthias Lee-Hifler100% (1)
- Tourette For Teachers PDFDocument8 pagesTourette For Teachers PDFkermit2goNo ratings yet
- JCM 08 00726 v2Document10 pagesJCM 08 00726 v2adhiniNo ratings yet