Download as pptx, pdf, or txt
You might also like
- Ryan's Retina 6th EdDocument2,754 pagesRyan's Retina 6th EdGarsa Garnol100% (2)
- Retina 5e Volume 1Document796 pagesRetina 5e Volume 1Oana Koppandi100% (1)
- Retinal Applications of Swept Source Optical Coherence Tomography (OCT) and Optical Coherence Tomography Angiography (OCTA)Document52 pagesRetinal Applications of Swept Source Optical Coherence Tomography (OCT) and Optical Coherence Tomography Angiography (OCTA)zhu zhuotingNo ratings yet
- Cirrus 6000 en 31 010 0047iDocument12 pagesCirrus 6000 en 31 010 0047iAung Kyaw ZawNo ratings yet
- Kuhn 2016Document548 pagesKuhn 2016Karan Kumarswamy100% (1)
- Dr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityDocument31 pagesDr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityRey AlwiwikhNo ratings yet
- OCT NotesDocument34 pagesOCT NotesTNo ratings yet
- RetinaDocument42 pagesRetinaAhmed Omara100% (2)
- Dutta 3Document601 pagesDutta 3Jeel GaralaNo ratings yet
- Dutta 2Document671 pagesDutta 2Jeel GaralaNo ratings yet
- Blurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocDocument15 pagesBlurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocRea Dominique CabanillaNo ratings yet
- Dutta 1Document667 pagesDutta 1Jeel GaralaNo ratings yet
- Retinal - Detachment Priciples and Practice 3rd EditionDocument277 pagesRetinal - Detachment Priciples and Practice 3rd EditionAni ArdiantiNo ratings yet
- ZEISS AngioPlex Clinical Compendium US 31 025 0070IDocument4 pagesZEISS AngioPlex Clinical Compendium US 31 025 0070Idarkspawn69No ratings yet
- Vol 2 Retinal AtlasDocument252 pagesVol 2 Retinal AtlasDra. Mitzy Torres - RetinólogaNo ratings yet
- Trabeculectomy TechniqueDocument8 pagesTrabeculectomy TechniqueJose Antonio Fuentes VegaNo ratings yet
- Pars Plana VitrectomyDocument6 pagesPars Plana VitrectomyAndreas OctavianoNo ratings yet
- Silicone Oil in Vitreoretinal SurgeryDocument30 pagesSilicone Oil in Vitreoretinal SurgeryBhumika RathNo ratings yet
- @MBS MedicalBooksStore 2018 Surgical PDFDocument181 pages@MBS MedicalBooksStore 2018 Surgical PDFDavid AndresNo ratings yet
- Cataract Surgery in Retina PatientsDocument21 pagesCataract Surgery in Retina PatientsAnonymous 4OnqyBErNo ratings yet
- Trabeculectomy CME 2022Document28 pagesTrabeculectomy CME 2022Allan AllenNo ratings yet
- Field Guide To Visual and Ophthalmic Optics PDFDocument120 pagesField Guide To Visual and Ophthalmic Optics PDFRani AprianiNo ratings yet
- en Face OCT Angiography Demonstrates Flow in Early Type 3 Neovascularization (Retinal Angiomatous Proliferation) PDFDocument4 pagesen Face OCT Angiography Demonstrates Flow in Early Type 3 Neovascularization (Retinal Angiomatous Proliferation) PDFThomas Sanhueza VásquezNo ratings yet
- Retinitis Pigmentosa: Prepared By: Aditya SaxenaDocument17 pagesRetinitis Pigmentosa: Prepared By: Aditya Saxenaaditya0% (1)
- Atlas of Retinal OCTDocument211 pagesAtlas of Retinal OCTVianka García LópezNo ratings yet
- Retinal DetachmentDocument16 pagesRetinal DetachmentCandice Lim Swee LingNo ratings yet
- Ocular TraumaDocument67 pagesOcular TraumaRenita Siwi M WNo ratings yet
- 09 LensDocument37 pages09 LensFrederica Mutiara100% (1)
- Olympus CLH 250Document2 pagesOlympus CLH 250Vinicius Belchior da Silva0% (1)
- StrabismusDocument19 pagesStrabismusSoumya Ranjan PandaNo ratings yet
- Ocular Anatomy PhysiologyDocument101 pagesOcular Anatomy PhysiologyĐạt VũNo ratings yet
- Ophthalmic Instruments Catalog: + ConsumablesDocument248 pagesOphthalmic Instruments Catalog: + ConsumablespamelasaldiviaNo ratings yet
- OCT Notes 3Document30 pagesOCT Notes 3TNo ratings yet
- Retinal Detachment SlideDocument54 pagesRetinal Detachment SlideHerin NataliaNo ratings yet
- Anisometropia in Children and Its ProblemDocument37 pagesAnisometropia in Children and Its ProblemekaNo ratings yet
- The Retinal Muller Cell PDFDocument293 pagesThe Retinal Muller Cell PDFkemalasari8818No ratings yet
- Ocular ExaminationDocument2 pagesOcular ExaminationMuhammad HaziqNo ratings yet
- Ophthalmic Lenses. Ajay Kumar BhootraDocument14 pagesOphthalmic Lenses. Ajay Kumar BhootraSutrishna PramanikNo ratings yet
- Retinal AnatomyDocument86 pagesRetinal AnatomySean ScogginsNo ratings yet
- Slit Lamp and CLs Complications HandoutDocument24 pagesSlit Lamp and CLs Complications HandoutRaeesah MehmoodNo ratings yet
- Divergent Strabismus (1) - 10Document65 pagesDivergent Strabismus (1) - 10Lavanya MadabushiNo ratings yet
- A Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyDocument7 pagesA Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyIJAR JOURNALNo ratings yet
- S3-05 Ophthalmology Red Eye (v2) PDFDocument12 pagesS3-05 Ophthalmology Red Eye (v2) PDFAl SyNo ratings yet
- Surgical Management of Third Nerve PalsyDocument7 pagesSurgical Management of Third Nerve Palsyhanaddul100% (1)
- American Optometric Association. Glaucoma HTTP - WWW - Aoa.org - Glaucoma - Xml.Document8 pagesAmerican Optometric Association. Glaucoma HTTP - WWW - Aoa.org - Glaucoma - Xml.Adriana Falla100% (1)
- Eye Care IntroductionDocument66 pagesEye Care IntroductionEdeti RoneNo ratings yet
- Ocular TraumaDocument50 pagesOcular TraumafatimaNo ratings yet
- Pars Plana Vitrectomy Surgery and AftercareDocument7 pagesPars Plana Vitrectomy Surgery and AftercareAAmit KumarNo ratings yet
- ZEISS AngioPlex Case Reports US 31 150 0032IDocument12 pagesZEISS AngioPlex Case Reports US 31 150 0032Idarkspawn69No ratings yet
- DomsDocument67 pagesDomsBook CoolNo ratings yet
- Ptosis Definition of Eyelid Ptosis: Abnormally Low Position of The Upper Eyelid Margin Caused by PoorDocument6 pagesPtosis Definition of Eyelid Ptosis: Abnormally Low Position of The Upper Eyelid Margin Caused by PoortiamaharaniNo ratings yet
- Notes: GlaucomaDocument175 pagesNotes: GlaucomasasaNo ratings yet
- Corneal Topography: Presented by Maj Anjani Kumar Resident (Ophth)Document71 pagesCorneal Topography: Presented by Maj Anjani Kumar Resident (Ophth)Yaman MuhaisenNo ratings yet
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- New Horizons in Osteoporosis Management: Yasser El MiedanyDocument903 pagesNew Horizons in Osteoporosis Management: Yasser El Miedanyglennys carelaNo ratings yet
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocument8 pagesCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanNo ratings yet
- CORNEA Vision2020 DR - RajarathnaDocument7 pagesCORNEA Vision2020 DR - Rajarathnaadi100% (1)
- Orbital Fractures/Orbital Blowout Fractures: Christina Gillespie, MDDocument40 pagesOrbital Fractures/Orbital Blowout Fractures: Christina Gillespie, MDaseel11No ratings yet
- GLUACOMADocument43 pagesGLUACOMAJoanna RachelNo ratings yet
- TrabeculectomyDocument28 pagesTrabeculectomyAlfu RafdiNo ratings yet
- Plastics 2Document5 pagesPlastics 2Jocel CastilloNo ratings yet
- 16.retinal Detachment PDFDocument42 pages16.retinal Detachment PDFFrederica MutiaraNo ratings yet
- Principles of Vitreoretinal Surgery - Scleral Buckle: Dr. Sumit Kumar MishraDocument49 pagesPrinciples of Vitreoretinal Surgery - Scleral Buckle: Dr. Sumit Kumar MishraSriniwasNo ratings yet
- Faros Making The Difference With Leading Innovation: Eye Surgery. Swiss MadeDocument32 pagesFaros Making The Difference With Leading Innovation: Eye Surgery. Swiss MadebellasatriawanNo ratings yet
- Diabetic RetinopathyDocument48 pagesDiabetic Retinopathykaran.A.K100% (1)
- Macular Hole - EyeWikiDocument4 pagesMacular Hole - EyeWikiRaesoo90210No ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityDocument11 pagesPhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityChrysanthus HerreraNo ratings yet
- Instrumentation R4aahDocument25 pagesInstrumentation R4aahMohammad Abdullah BawtagNo ratings yet
- Ocular USG of Post EyeDocument14 pagesOcular USG of Post EyeAL MARIA MEDNo ratings yet
- MasonDocument208 pagesMasongdvfwqeguewguqfgNo ratings yet
- Impact of Age On Scleral Buckling Surgery For Rhegmatogenous Retinal DetachmentDocument8 pagesImpact of Age On Scleral Buckling Surgery For Rhegmatogenous Retinal Detachmentdwi purwantiNo ratings yet
- Prevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati UpadhyayDocument42 pagesPrevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati Upadhyaypranaya mallNo ratings yet
- Bhardwaj 2018Document6 pagesBhardwaj 2018evilelagNo ratings yet
- Retinal DetachmentDocument7 pagesRetinal Detachmentjay dewanagnNo ratings yet
- Gui ListedTherapies PDFDocument263 pagesGui ListedTherapies PDFSampath KumarNo ratings yet
- List of Surgeries: AbdomenDocument35 pagesList of Surgeries: AbdomenSaurav SaikiaNo ratings yet
- Sarojini Devi Eye Hospital Hyderabad (OP Timings and Address)Document1 pageSarojini Devi Eye Hospital Hyderabad (OP Timings and Address)mrs.shweta4444No ratings yet
- Diabetic Retinopathy: Clinical Findings and Management: Review ArticleDocument4 pagesDiabetic Retinopathy: Clinical Findings and Management: Review ArticlewadejackNo ratings yet
- Vaga Hospital - LUC005 - Aditya BirlaDocument7 pagesVaga Hospital - LUC005 - Aditya BirlajaipalNo ratings yet
- Machular HoleDocument14 pagesMachular HoleRaymond FrazierNo ratings yet
- Ophth TestsDocument48 pagesOphth TestsAkakpo ReindolfNo ratings yet
- Case RRDDocument56 pagesCase RRDRana AhmedNo ratings yet
- Presentation DR Tourville - IGSDocument7 pagesPresentation DR Tourville - IGSadesamboraNo ratings yet
- Use of The Delphi Process in Paediatric Cataract Management: Clinical ScienceDocument5 pagesUse of The Delphi Process in Paediatric Cataract Management: Clinical ScienceYanjinlkham KhNo ratings yet
- Vitrectomy For Endophthalmitis: 5-Year Study of Outcomes and ComplicationsDocument8 pagesVitrectomy For Endophthalmitis: 5-Year Study of Outcomes and ComplicationsqisthiNo ratings yet
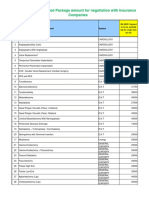
- IMA NHB Suggested Package Amount For Negotiation With Insurance CompaniesDocument5 pagesIMA NHB Suggested Package Amount For Negotiation With Insurance Companiesmonikparmar1No ratings yet
- DT - Normal Eyes With Sudden Painless Loss of VisionDocument34 pagesDT - Normal Eyes With Sudden Painless Loss of VisionIzzatul Yazidah100% (1)
- Advances in Pneumatic Retinopexy Challenges and InnovationsDocument11 pagesAdvances in Pneumatic Retinopexy Challenges and Innovationsnurulmasruroh250No ratings yet
- Ryans Retina 7Th Edition Srinivas R Sadda MD Editor Full Chapter PDFDocument69 pagesRyans Retina 7Th Edition Srinivas R Sadda MD Editor Full Chapter PDFdesjandiabel100% (5)
- Vitreous HemorrhageDocument7 pagesVitreous HemorrhageindahNo ratings yet