Download as ppt, pdf, or txt
You might also like
- Bone and Soft Tissue SarcomaDocument67 pagesBone and Soft Tissue SarcomaSalmanArifNo ratings yet
- Sustainable Agricultural Landscapes LabDocument2 pagesSustainable Agricultural Landscapes LabArtNo ratings yet
- Ipil-Ipil As An Alternative Source of Floorwax - Lazaro, Et - Al.Document65 pagesIpil-Ipil As An Alternative Source of Floorwax - Lazaro, Et - Al.YLreveb Camacho80% (44)
- VATS Bypass ModuleDocument3 pagesVATS Bypass ModuleSHOOTEENo ratings yet
- Solved Problems On Mass Transfer PDFDocument12 pagesSolved Problems On Mass Transfer PDFProtim DasNo ratings yet
- 3 Ecmo Post Grad SJH 2019 - Final DR LeeDocument133 pages3 Ecmo Post Grad SJH 2019 - Final DR LeerisanataliasiburianNo ratings yet
- "Pediatric Radiation Oncology": R. Miralbell Hôpitaux Universitaires, GenèveDocument118 pages"Pediatric Radiation Oncology": R. Miralbell Hôpitaux Universitaires, GenèveRus Paul OvidiuNo ratings yet
- Ecmo 2017Document19 pagesEcmo 2017Josefina Daza SantamaríaNo ratings yet
- A Review of Spontaneous Closure of Ventricular Septal DefectDocument5 pagesA Review of Spontaneous Closure of Ventricular Septal DefectMarina RotaruNo ratings yet
- Otite Si SinDocument29 pagesOtite Si Sinminerva_stanciuNo ratings yet
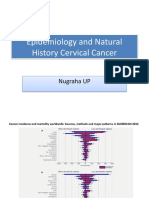
- Epidemiology and Natural History Cervical CancerDocument30 pagesEpidemiology and Natural History Cervical Cancermuhammadnurul asmiNo ratings yet
- Pediatric Extracorporeal Cardiopulmonary.2Document9 pagesPediatric Extracorporeal Cardiopulmonary.2Lesley RoaNo ratings yet
- Abhishek Vaidya - NOG - LarynxDocument42 pagesAbhishek Vaidya - NOG - LarynxAbhishek VaidyaNo ratings yet
- Pakkirmasthan A, Kurakula S: Introducti OnDocument5 pagesPakkirmasthan A, Kurakula S: Introducti Oneka waraNo ratings yet
- Malignant Pleural Effusion PrevalenceDocument72 pagesMalignant Pleural Effusion PrevalenceAkbar SyarialNo ratings yet
- Pediatric Pituitary Adenomas: Sandeep Kunwar and Charles B. WilsonDocument6 pagesPediatric Pituitary Adenomas: Sandeep Kunwar and Charles B. WilsonJhalasNo ratings yet
- Outcomes of Lung Transplantation in Pah: Vijil RahulanDocument92 pagesOutcomes of Lung Transplantation in Pah: Vijil RahulanvrahulanNo ratings yet
- Ecmo and SepsisDocument37 pagesEcmo and SepsisMarckus BrodyNo ratings yet
- Update in Paediatric Resuscitation: 2005 International Guidelines: Recommendations From NRCDocument32 pagesUpdate in Paediatric Resuscitation: 2005 International Guidelines: Recommendations From NRCapi-3760283No ratings yet
- Treatmentof Pediatric Acute Lymphoblastic Leukemiaand Recent AdvancesDocument17 pagesTreatmentof Pediatric Acute Lymphoblastic Leukemiaand Recent AdvancesRizkaNo ratings yet
- New VTE Terbaru FixDocument68 pagesNew VTE Terbaru FixSurya MahardikaNo ratings yet
- Fondaparinux VTE (JCU 2018)Document54 pagesFondaparinux VTE (JCU 2018)sofiNo ratings yet
- Khan 2023 Outcomes of Surgical Repair of Tetralogy of Fallot Child and AdultDocument6 pagesKhan 2023 Outcomes of Surgical Repair of Tetralogy of Fallot Child and AdultElfrida AuliaNo ratings yet
- 2019 ESMO Preceptorship Breast Neo Adj Endocrine Therapy Special Populations PrudenceDocument60 pages2019 ESMO Preceptorship Breast Neo Adj Endocrine Therapy Special Populations PrudencemrsilNo ratings yet
- Cancer de Plaman Cu Celule MiciDocument84 pagesCancer de Plaman Cu Celule MiciANDREEA GRIGORASNo ratings yet
- Caldeira 2018Document6 pagesCaldeira 2018Engels Yeltsin Ponce GonzalesNo ratings yet
- Progress in Retinal and Eye ResearchDocument33 pagesProgress in Retinal and Eye ResearchNabita AuliaNo ratings yet
- Task 11 (600 Words)Document5 pagesTask 11 (600 Words)Nadia RiazNo ratings yet
- 2 PBDocument4 pages2 PBSuryati HusinNo ratings yet
- Duygu 2020Document4 pagesDuygu 2020Aditya HendraNo ratings yet
- European Guidelines On Perioperative Venous.8Document7 pagesEuropean Guidelines On Perioperative Venous.8ionut.andruscaNo ratings yet
- SOP Pemeriksaan BerkalaDocument74 pagesSOP Pemeriksaan BerkalaRian SasmitaNo ratings yet
- Meckel'S Diverticulum in The Adult: SciencedirectDocument7 pagesMeckel'S Diverticulum in The Adult: SciencedirectLeokádio BarrosoNo ratings yet
- Tumori Bubrega U DeceDocument45 pagesTumori Bubrega U Deceplavusa-blNo ratings yet
- Outcomes of Surgery For Infective Endocarditis in Children: A 30-Year ExperienceDocument12 pagesOutcomes of Surgery For Infective Endocarditis in Children: A 30-Year ExperienceMehdi285858No ratings yet
- Endometrial Ablation Experience in SFHDocument36 pagesEndometrial Ablation Experience in SFHElham MNo ratings yet
- Paediatric Trauma Protocols: WWW - Rcr.ac - UkDocument25 pagesPaediatric Trauma Protocols: WWW - Rcr.ac - UkMehranNasrallaNo ratings yet
- Small Cell Lung Cancer (SCLC) and Tkis in NSCLCDocument73 pagesSmall Cell Lung Cancer (SCLC) and Tkis in NSCLCAgi Azhari SandiniNo ratings yet
- Congenital Diaphragmatic Hernia: Trials and Tribulations: Roman Sydorak, MD, MPHDocument76 pagesCongenital Diaphragmatic Hernia: Trials and Tribulations: Roman Sydorak, MD, MPHoNo ratings yet
- Congenital Diaphragmatic Hernia: Trials and Tribulations: Roman Sydorak, MD, MPHDocument76 pagesCongenital Diaphragmatic Hernia: Trials and Tribulations: Roman Sydorak, MD, MPHoNo ratings yet
- Bone and Soft Tissue SarcomasDocument57 pagesBone and Soft Tissue SarcomasTerseah MuNo ratings yet
- Ewing's Sarcoma Review ArticleDocument9 pagesEwing's Sarcoma Review ArticleSayan DasNo ratings yet
- Overview PADDocument98 pagesOverview PADAstrid PramudyaaNo ratings yet
- EMSOS19. Abstract BookDocument440 pagesEMSOS19. Abstract BookSisay GirmaNo ratings yet
- Agnes Lee Thrombosis PresentationDocument37 pagesAgnes Lee Thrombosis Presentationari naNo ratings yet
- AnotherDocument11 pagesAnotherTudor DumitrascuNo ratings yet
- Papini SIBIU 2018Document53 pagesPapini SIBIU 2018Alina Ioana PaduraruNo ratings yet
- 12 Bone and Soft Tissue Sarcomas 200609 v2Document58 pages12 Bone and Soft Tissue Sarcomas 200609 v2dr. Ahmad MuhsininNo ratings yet
- VTE: 2016 ACCP Update With Best Evidence and Best PracticesDocument78 pagesVTE: 2016 ACCP Update With Best Evidence and Best Practicesagustina mereNo ratings yet
- Adenosquamous JournalDocument2 pagesAdenosquamous JournalirfanNo ratings yet
- Head and Neck Mucosal MelanomaDocument5 pagesHead and Neck Mucosal MelanomaHAMIDNo ratings yet
- SWAIMANDocument18 pagesSWAIMANVan John MagallanesNo ratings yet
- Venous Thrombosis in Children BJH - 2011Document12 pagesVenous Thrombosis in Children BJH - 2011Chenuri Annamarie RanasingheNo ratings yet
- CML PresentationDocument55 pagesCML PresentationИван НегарэNo ratings yet
- Meyers 2012Document10 pagesMeyers 2012Dra Cinthya Paredes BarzolaNo ratings yet
- Dream Trial Journal PresentationDocument30 pagesDream Trial Journal PresentationRam Kumar ShresthaNo ratings yet
- Endoscopy in The ElderlyDocument7 pagesEndoscopy in The ElderlyFebyan AbotNo ratings yet
- Epidemiology of Intratemporal Complications of Otitis MediaDocument7 pagesEpidemiology of Intratemporal Complications of Otitis MediaMoerdono PambudiNo ratings yet
- What Is The Role of Localized Therapies in Metastatic RCC?: Axel Bex, MD, PHDDocument35 pagesWhat Is The Role of Localized Therapies in Metastatic RCC?: Axel Bex, MD, PHDchandni mittalNo ratings yet
- Sepsis NewDocument17 pagesSepsis Newapi-363606423No ratings yet
- Diabetic Foot UlcersDocument40 pagesDiabetic Foot UlcersRajaRafianNo ratings yet
- Segel 2008Document15 pagesSegel 2008valentina rojasNo ratings yet
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceFrom EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Pharmaceutical Considerations During Ecmo: John Mcguinness - Cardiothoracic Critical Care PharmacistDocument25 pagesPharmaceutical Considerations During Ecmo: John Mcguinness - Cardiothoracic Critical Care PharmacistPERFUZIJANo ratings yet
- ECMO Cannulae, Cannulation, Components, Pumps and Set-UP UKEDocument23 pagesECMO Cannulae, Cannulation, Components, Pumps and Set-UP UKEPERFUZIJANo ratings yet
- MISTRAL PresentationDocument13 pagesMISTRAL PresentationPERFUZIJANo ratings yet
- Thoratec Centrimag & Pedivas: Clinical Operation and Patient ManagementDocument11 pagesThoratec Centrimag & Pedivas: Clinical Operation and Patient ManagementPERFUZIJANo ratings yet
- Ecmo Cannulation: Ignacio Malagon Frca, PHD, Fficm Consultant Cardiac AnaesthesiaDocument29 pagesEcmo Cannulation: Ignacio Malagon Frca, PHD, Fficm Consultant Cardiac AnaesthesiaPERFUZIJANo ratings yet
- Laparoscopic Bilateral Tubal LigationDocument2 pagesLaparoscopic Bilateral Tubal Ligationapi-3712326100% (1)
- Instrucciones MicroondasDocument92 pagesInstrucciones MicroondasPatriiciiaTomlinsonNo ratings yet
- EC Lab ManualDocument5 pagesEC Lab ManualsruthyNo ratings yet
- Why Transformers ExplodeDocument15 pagesWhy Transformers ExplodesasahitoNo ratings yet
- MESL - Algebra 2Document7 pagesMESL - Algebra 2Mark-Lorie Duculan NonesNo ratings yet
- The Organization of Modern KitchensDocument9 pagesThe Organization of Modern KitchensJohnson Macayan FernándezNo ratings yet
- 8189473158Document326 pages8189473158sharan100% (6)
- Optimum Frying PDFDocument13 pagesOptimum Frying PDFcindy tia hasanahNo ratings yet
- COSC PresentationDocument80 pagesCOSC PresentationLydia DePillisNo ratings yet
- Gad AccomplishementxlsxDocument4 pagesGad AccomplishementxlsxDenielle DelosoNo ratings yet
- Part 4 Hoisting SystemDocument35 pagesPart 4 Hoisting SystemJood SultanNo ratings yet
- February 21, 2014 Strathmore TimesDocument28 pagesFebruary 21, 2014 Strathmore TimesStrathmore TimesNo ratings yet
- Orion 920DX UkDocument2 pagesOrion 920DX UkVinícius Leite BandeiraNo ratings yet
- TuberculosisDocument9 pagesTuberculosisIdasari DewiNo ratings yet
- Pregnancy TestDocument2 pagesPregnancy TestOsinachi WilsonNo ratings yet
- This Study Resource Was: Piramal - E - Swasthya Case SubmissionDocument4 pagesThis Study Resource Was: Piramal - E - Swasthya Case SubmissiondjNo ratings yet
- Deep Sea Mining PresentationDocument14 pagesDeep Sea Mining Presentationganesh100% (1)
- Physical Science Chapter 5 Ionic BondingDocument4 pagesPhysical Science Chapter 5 Ionic Bondingluis martinezNo ratings yet
- Diagnosis and Management of Intrahepatic Cholangiocarcinoma: A Comprehensive Update For The RadiologistDocument22 pagesDiagnosis and Management of Intrahepatic Cholangiocarcinoma: A Comprehensive Update For The RadiologistNadia HamdaniNo ratings yet
- NR 34 - Off Shore WorkDocument27 pagesNR 34 - Off Shore WorkMárcio DiasNo ratings yet
- Baypren® 320-1 Safety Data SheetDocument10 pagesBaypren® 320-1 Safety Data SheetXiaofeng MengNo ratings yet
- Examination of The Child With CerebralpalsyDocument52 pagesExamination of The Child With CerebralpalsyRiaz KhanNo ratings yet
- Cii-Sorabji Green Business CentreDocument46 pagesCii-Sorabji Green Business CentremadhuNo ratings yet
- Fruits Washing & SanitationDocument43 pagesFruits Washing & SanitationMuhammad RamzanNo ratings yet
- IDC 4U2 - Unit 3 Task 5 - SSDocument4 pagesIDC 4U2 - Unit 3 Task 5 - SSsavannah.e.stonehouseNo ratings yet
- Iso 27001 ChecklistDocument8 pagesIso 27001 ChecklistALEX COSTA CRUZNo ratings yet