Download as ppt, pdf, or txt
You might also like
- 157 Research Papers Supporting The Vaccine - Autism Link - Autism Spectrum - AutismDocument171 pages157 Research Papers Supporting The Vaccine - Autism Link - Autism Spectrum - AutismDMDONo ratings yet
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- Sop For Controlled DrugsDocument75 pagesSop For Controlled DrugsBalaji Pharmacy - GMNo ratings yet
- Clinical Pharmacology in Special PopulationsDocument57 pagesClinical Pharmacology in Special PopulationsNomar CapoyNo ratings yet
- Anesthesia For Geriatric PatientsDocument45 pagesAnesthesia For Geriatric PatientsIDI Bangka BaratNo ratings yet
- Aminoglycoside PharmacokineticsDocument13 pagesAminoglycoside PharmacokineticsLama SaudNo ratings yet
- Geriatric Clinical Pharmacology and Clinical Trials in The ElderlyDocument6 pagesGeriatric Clinical Pharmacology and Clinical Trials in The ElderlyMaria SpatariNo ratings yet
- Dosage Adjustment in Renal Failure: Dr. Parminder Nain Professor & Head (Pharmd) MMCP, MmduDocument145 pagesDosage Adjustment in Renal Failure: Dr. Parminder Nain Professor & Head (Pharmd) MMCP, Mmduparminder.nain29No ratings yet
- Geriartry and AnethesiaDocument5 pagesGeriartry and AnethesiaDavidVictoriousLukasNo ratings yet
- Hepatitis B KronikDocument15 pagesHepatitis B KronikSiti NcitNo ratings yet
- Jurnal 5 - 2007jhdgfzdjDocument3 pagesJurnal 5 - 2007jhdgfzdjELa NovianaNo ratings yet
- Bliss LNDocument37 pagesBliss LNNeelam Devi MaraviNo ratings yet
- List The Factors Influencing The Interpretation of TDM ReportDocument3 pagesList The Factors Influencing The Interpretation of TDM ReportOdyNo ratings yet
- Dosing of Gentamicin in Patients With End-Stage Renal Disease Receiving HemodialysisDocument10 pagesDosing of Gentamicin in Patients With End-Stage Renal Disease Receiving HemodialysisLuciana OliveiraNo ratings yet
- Emergency Physician-Initiated Resuscitative Extracorporeal Membrane OxygenationDocument13 pagesEmergency Physician-Initiated Resuscitative Extracorporeal Membrane Oxygenationshiffa ramadhantiNo ratings yet
- Clinical Pharmacokinetics Therapeutic Drug MonitoringDocument41 pagesClinical Pharmacokinetics Therapeutic Drug MonitoringTrifena Prisca MosseNo ratings yet
- Pediatric Physiology: Presented By: Mohammad El-Masri Moderated By: Dr. Omar AbabnehDocument41 pagesPediatric Physiology: Presented By: Mohammad El-Masri Moderated By: Dr. Omar AbabnehMorad SatariNo ratings yet
- نسخة Report A4 Week 7...Document8 pagesنسخة Report A4 Week 7...Amasi Al-khiderNo ratings yet
- Overview of Total Intravenous Anesthesia in ChildrenDocument12 pagesOverview of Total Intravenous Anesthesia in ChildrenJosibel OcantoNo ratings yet
- Nutritional Status Among Peritoneal Dialysis Patients After Oral Supplement With ONCE Dialyze FormulaDocument7 pagesNutritional Status Among Peritoneal Dialysis Patients After Oral Supplement With ONCE Dialyze FormulanuvitaNo ratings yet
- Principles of Preoperative and Operative SurgeryDocument71 pagesPrinciples of Preoperative and Operative SurgeryRajarshi KumarNo ratings yet
- Geriatrics Dr. Bereket Molla TigabuDocument27 pagesGeriatrics Dr. Bereket Molla Tigabuphoto copyhemnNo ratings yet
- Pediatric Pharmacology - Dr. JangiDocument29 pagesPediatric Pharmacology - Dr. JangiBashar Khalil100% (1)
- Laboratory Testing in PsychiatryDocument29 pagesLaboratory Testing in PsychiatrySera ChunNo ratings yet
- Clinial Pharmacokinetics of CyclosporineDocument14 pagesClinial Pharmacokinetics of CyclosporineUmair MazharNo ratings yet
- 29732181: Optimising Drug Dosing in Patients Receiving Extracorporeal Membrane OxygenationDocument13 pages29732181: Optimising Drug Dosing in Patients Receiving Extracorporeal Membrane OxygenationEward Rod SalNo ratings yet
- Antidepressants 266: JSS College of Pharmacy, MysuruDocument68 pagesAntidepressants 266: JSS College of Pharmacy, MysurucrissNo ratings yet
- CANT3 Onco-Nephrology - Core Curriculum 2015Document15 pagesCANT3 Onco-Nephrology - Core Curriculum 2015alam25No ratings yet
- 1 s2.0 S2468024921010329 MainDocument11 pages1 s2.0 S2468024921010329 Maindavid garciaNo ratings yet
- Drug Dosing Renal Failure PDFDocument41 pagesDrug Dosing Renal Failure PDFWildan Wisnu WardayaNo ratings yet
- 2995 - 158180 - Aplikasi Farmakokinetika Pada Neonate Pediatrik GeriatrikDocument50 pages2995 - 158180 - Aplikasi Farmakokinetika Pada Neonate Pediatrik GeriatriksuhantoroNo ratings yet
- Drug Induced Kidney Disease: Dr. Hamid SaeedDocument42 pagesDrug Induced Kidney Disease: Dr. Hamid SaeedKhadija KamranNo ratings yet
- PLB 1 B 8 Rianti NovalianaDocument21 pagesPLB 1 B 8 Rianti NovalianavikaseptideyaniNo ratings yet
- Hepatic Encephalopathy: DR Sadath HussainDocument32 pagesHepatic Encephalopathy: DR Sadath Hussain966342No ratings yet
- 1.1. Adv. Biopharma.-A-Dose Adjustment in Renal & Hepatic Failure - by M.firoz KhanDocument38 pages1.1. Adv. Biopharma.-A-Dose Adjustment in Renal & Hepatic Failure - by M.firoz KhanRaju NiraulaNo ratings yet
- Hippokratia 11 175 PDFDocument3 pagesHippokratia 11 175 PDFRahma WatiNo ratings yet
- Harm: Critical Appraisal: Perpetual Help Medical Center-Biñan Uph-Dr. Jose G. Tamayo Medical University Foundation, IncDocument34 pagesHarm: Critical Appraisal: Perpetual Help Medical Center-Biñan Uph-Dr. Jose G. Tamayo Medical University Foundation, IncKim Adarem Joy ManimtimNo ratings yet
- Pharmacokinetics of Anti-Epileptic Drugs and Their Clinical SignificanceDocument12 pagesPharmacokinetics of Anti-Epileptic Drugs and Their Clinical Significancerozina mulatNo ratings yet
- 2012 Best Parctice Medical O Grady TH en FHADocument7 pages2012 Best Parctice Medical O Grady TH en FHASol Del Mar SarmientoNo ratings yet
- JC AaDocument31 pagesJC AaNaeem AbbasNo ratings yet
- Challenges Diuretics CasebasedDocument13 pagesChallenges Diuretics CasebasedDaniel MelendezNo ratings yet
- Fol Firin OxDocument11 pagesFol Firin OxGuilherme SalgadoNo ratings yet
- CRRT Antibiotic DosingDocument8 pagesCRRT Antibiotic DosingFranz Josef TariganNo ratings yet
- JCPT 12081Document7 pagesJCPT 12081belqis ratuNo ratings yet
- EMEA Guideline On The Evaluation of The Pharmacokinetics DISFUNCTION HEEPATICDocument10 pagesEMEA Guideline On The Evaluation of The Pharmacokinetics DISFUNCTION HEEPATICAccung BuccuNo ratings yet
- Ratih Sumirat - Kegawatdaruratan Klinik ATLS UpdateDocument16 pagesRatih Sumirat - Kegawatdaruratan Klinik ATLS UpdateRatih Nurdiany SumiratNo ratings yet
- 11-Clarke - Pharmacokinetics and TDMDocument54 pages11-Clarke - Pharmacokinetics and TDMMiski AghniaNo ratings yet
- Approach ConsiderationsDocument12 pagesApproach ConsiderationsTyna Mew-mewNo ratings yet
- Precision Med PPT ExplainationDocument2 pagesPrecision Med PPT ExplainationSeemron BiswalNo ratings yet
- Anesthesia For TURP: Maimouna Bah and Michael Stuart GreenDocument3 pagesAnesthesia For TURP: Maimouna Bah and Michael Stuart GreenRio Taruna JatiNo ratings yet
- Drug Dosage in The Elderly Is It Rational?: Klaus TrunheimDocument16 pagesDrug Dosage in The Elderly Is It Rational?: Klaus TrunheimM Yosa EffendiNo ratings yet
- Drug Dosage in The Elderly Is It Rational?: Klaus TrunheimDocument16 pagesDrug Dosage in The Elderly Is It Rational?: Klaus TrunheimM Yosa EffendiNo ratings yet
- Sepsis and Septic Shock Guidelines: DR Mahesh KumarDocument45 pagesSepsis and Septic Shock Guidelines: DR Mahesh KumarMahesh RajwalNo ratings yet
- Treatment of Electrolyte Disorders in Adult Patients in The Intensive Care UnitDocument21 pagesTreatment of Electrolyte Disorders in Adult Patients in The Intensive Care UnitBuat TugasNo ratings yet
- PDIS - Calculation of Medication DosesDocument41 pagesPDIS - Calculation of Medication DosesMark Angelo JaurigueNo ratings yet
- Intravenous Mel Dex July 08 Checked in Date Oct 2011Document2 pagesIntravenous Mel Dex July 08 Checked in Date Oct 2011GabrielNo ratings yet
- 21223lbl PDFDocument11 pages21223lbl PDFMelia Fatrani RufaidahNo ratings yet
- Nutritional Management in Critically Ill ConditionDocument30 pagesNutritional Management in Critically Ill Conditiondwi ayieNo ratings yet
- Manejo de La Sepsis 2Document5 pagesManejo de La Sepsis 2Rachmi Pratiwi Febrita PartiNo ratings yet
- phar.2858Document12 pagesphar.2858Mohammed VHNo ratings yet
- Geriatric Pharmacology. Journal of The American Podriatric Medical AssociationDocument8 pagesGeriatric Pharmacology. Journal of The American Podriatric Medical AssociationJose Fernando Díez ConchaNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Pediatric and Adult ECMO TalkDocument58 pagesPediatric and Adult ECMO TalkPERFUZIJANo ratings yet
- ECMO Cannulae, Cannulation, Components, Pumps and Set-UP UKEDocument23 pagesECMO Cannulae, Cannulation, Components, Pumps and Set-UP UKEPERFUZIJANo ratings yet
- MISTRAL PresentationDocument13 pagesMISTRAL PresentationPERFUZIJANo ratings yet
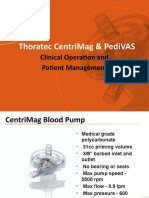
- Thoratec Centrimag & Pedivas: Clinical Operation and Patient ManagementDocument11 pagesThoratec Centrimag & Pedivas: Clinical Operation and Patient ManagementPERFUZIJANo ratings yet
- Ecmo Cannulation: Ignacio Malagon Frca, PHD, Fficm Consultant Cardiac AnaesthesiaDocument29 pagesEcmo Cannulation: Ignacio Malagon Frca, PHD, Fficm Consultant Cardiac AnaesthesiaPERFUZIJANo ratings yet
- Mir Asturias ManualsDocument1 pageMir Asturias ManualsScribdTranslationsNo ratings yet
- FARM Note CarePlansDocument11 pagesFARM Note CarePlansbrain bareNo ratings yet
- Abubakar Zubeidi MCVU 2020Document22 pagesAbubakar Zubeidi MCVU 2020annisNo ratings yet
- Forensic NursingDocument3 pagesForensic NursingJoras Joy Yu Gregorio-AntojadoNo ratings yet
- 4.5 Biopharmaceutics and Pharmacokinetics (Theory)Document2 pages4.5 Biopharmaceutics and Pharmacokinetics (Theory)Kushani DesaiNo ratings yet
- TABLANZA - FINALS ACTIVTY 2 (LAB) .EditedDocument2 pagesTABLANZA - FINALS ACTIVTY 2 (LAB) .Editedtrust nobodyNo ratings yet
- Constipation Risk Assessment ToolDocument2 pagesConstipation Risk Assessment ToolAnggie Anggriyana100% (1)
- Peripheral IV Catheters ChartDocument1 pagePeripheral IV Catheters ChartTitus Lesmana100% (1)
- Ijcpd 11 490Document6 pagesIjcpd 11 490MayerNo ratings yet
- Efficacy of Fennel and Combined Oral Contraceptive On Depot Medroxyprogesterone Acetate-Induced AmenorrheaDocument7 pagesEfficacy of Fennel and Combined Oral Contraceptive On Depot Medroxyprogesterone Acetate-Induced Amenorrhearestu pangestutiNo ratings yet
- 1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileDocument6 pages1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileValdemar Caumo JuniorNo ratings yet
- LorazepamDocument6 pagesLorazepamIanDiel ParagosoNo ratings yet
- Consent and Information FormDocument2 pagesConsent and Information FormChiNo ratings yet
- MetforminDocument2 pagesMetforminEdem LeeNo ratings yet
- Word Brochure Template 7 InsideDocument1 pageWord Brochure Template 7 InsideAnonymous ejce48emNo ratings yet
- Kejang Pada Gigitan Ular Berbisa: Laporan KasusDocument10 pagesKejang Pada Gigitan Ular Berbisa: Laporan KasusHerlina Sabe HaringNo ratings yet
- Myths, Facts and Misconceptions About HIV and AIDSDocument5 pagesMyths, Facts and Misconceptions About HIV and AIDSwilliam joabNo ratings yet
- Group 5 - English - A14-A KeperawatanDocument11 pagesGroup 5 - English - A14-A KeperawatanNi luh ade dwi AntariNo ratings yet
- DGHS IPHS Sub-Dist Hosps 31 To 50Document113 pagesDGHS IPHS Sub-Dist Hosps 31 To 50shanmugapriyasankarNo ratings yet
- Radiation TherapyDocument2 pagesRadiation Therapyapi-390677852No ratings yet
- Drug Study: Lidocaine: Generic Name: Lidocaine Pharmacologic: Mechanism of ActionDocument6 pagesDrug Study: Lidocaine: Generic Name: Lidocaine Pharmacologic: Mechanism of ActionShara Lailanie A. AzisNo ratings yet
- Revised 2016 AMA Code of Ethics 2004.Document7 pagesRevised 2016 AMA Code of Ethics 2004.rana sampurnaNo ratings yet
- Imaging in Otosclerosis: A Pictorial ReviewDocument8 pagesImaging in Otosclerosis: A Pictorial ReviewChlo14No ratings yet
- Bioav 3Document264 pagesBioav 3Sabiruddin Mirza DipuNo ratings yet
- Case Study: International Journal of Current ResearchDocument2 pagesCase Study: International Journal of Current ResearchUtami MayasariNo ratings yet
- Saba Ali ResumeDocument2 pagesSaba Ali Resumeapi-310400780No ratings yet
- Communication Scenarios (Healthcare)Document19 pagesCommunication Scenarios (Healthcare)nketjimotswaledi100% (1)
- Ivyx Z Fvbivm I Ivyx Z JVBF F VKWMB ..Document2 pagesIvyx Z Fvbivm I Ivyx Z JVBF F VKWMB ..Arafat RinkyNo ratings yet