Download as pptx, pdf, or txt
You might also like
- (Netter) Atlas of Human Anatomy. 8° (2023) - 4Document9 pages(Netter) Atlas of Human Anatomy. 8° (2023) - 4ALEXIS SEDERAPNo ratings yet
- Mouth and Mastication GigiDocument2 pagesMouth and Mastication GigiGondoriyo PkmNo ratings yet
- Function Must Be Understood Before Dysfunction Can Have Any MeaningDocument47 pagesFunction Must Be Understood Before Dysfunction Can Have Any MeaningDapinder BrarNo ratings yet
- Propsy2 - Activity - 6 - Ical, Erica Ann e PDFDocument2 pagesPropsy2 - Activity - 6 - Ical, Erica Ann e PDFErica Ann IcalNo ratings yet
- The Skeletal System: ArticulationsDocument102 pagesThe Skeletal System: ArticulationstiiandiNo ratings yet
- Arches of The FootDocument1 pageArches of The FootCristina MuyargasNo ratings yet
- ELBOWDocument7 pagesELBOWPhoebe DemegilloNo ratings yet
- 3 Wednesday UCSDPG16 Syllabus PDFDocument206 pages3 Wednesday UCSDPG16 Syllabus PDFAmit ShresthaNo ratings yet
- M.15 The Hand Part 1 by DR LaygoDocument9 pagesM.15 The Hand Part 1 by DR LaygoGrape JuiceNo ratings yet
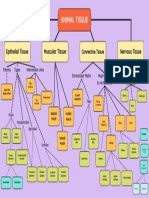
- Concept MapDocument1 pageConcept MapTetra HedronNo ratings yet
- Morning Discussion Juli 2023 PDFDocument1 pageMorning Discussion Juli 2023 PDFIndra Anwari RukmanNo ratings yet
- IGCSE PE (0413) - Anatomy & Physiology Revision Questions FlashcardsDocument3 pagesIGCSE PE (0413) - Anatomy & Physiology Revision Questions FlashcardsbahadurNo ratings yet
- The Temporomandibular Joints, Teeth, and Muscles, and Their FunctionsDocument16 pagesThe Temporomandibular Joints, Teeth, and Muscles, and Their Functionsfalop41797No ratings yet
- Ultrasound Greater TrochanterDocument7 pagesUltrasound Greater TrochanterDr Reza ModarresNo ratings yet
- CH - 05 - THE SKELETAL SYSTEMDocument147 pagesCH - 05 - THE SKELETAL SYSTEMCheska DillupacNo ratings yet
- 1 Ankle Fractures HandoutDocument8 pages1 Ankle Fractures HandoutLuisAngelPonceTorresNo ratings yet
- Ankle and FootDocument10 pagesAnkle and FootGlea PavillarNo ratings yet
- IVUS Image Interpretation Poster (PI-396201-AA)Document2 pagesIVUS Image Interpretation Poster (PI-396201-AA)Anonymous oQtve4o100% (1)
- Ankle ApproachesDocument58 pagesAnkle ApproachesScribdTranslationsNo ratings yet
- Rita Barros - Wrist - And.hand - EULAR TTT 2022Document17 pagesRita Barros - Wrist - And.hand - EULAR TTT 2022Rita BarrosNo ratings yet
- Netter's Atlas of Human Anatomy 6E-1Document4 pagesNetter's Atlas of Human Anatomy 6E-1giselaNo ratings yet
- Foot and Ankle TreatmentDocument59 pagesFoot and Ankle TreatmentKonstantinosKontouvalisNo ratings yet
- BioMat 02Document24 pagesBioMat 02gonvic7411No ratings yet
- Foot and Ankle Anatomy and Physical Examination PART 1Document49 pagesFoot and Ankle Anatomy and Physical Examination PART 1eric sivaneshNo ratings yet
- 2 - Anatomy and Kinesiology of The WristDocument10 pages2 - Anatomy and Kinesiology of The WristLeanna NNo ratings yet
- Equine Lower Limb StructureDocument1 pageEquine Lower Limb Structureapi-306398192No ratings yet
- Magee 6th Edition - OPA - 4 Temporomandibular JointDocument30 pagesMagee 6th Edition - OPA - 4 Temporomandibular JointRonny Araya AbarcaNo ratings yet
- TFCC PDFDocument22 pagesTFCC PDFMayor AnakNo ratings yet
- Biomechanics of Mallet Finger A Case ReportDocument4 pagesBiomechanics of Mallet Finger A Case ReportAkbar GazaliNo ratings yet
- Physical Propertes of Bone, Cartilage and Their Function Adaptation in Various ConditionsDocument15 pagesPhysical Propertes of Bone, Cartilage and Their Function Adaptation in Various ConditionsSwasti PandeyNo ratings yet
- Varma 1st Exam NotesDocument7 pagesVarma 1st Exam NotesKarthick KanagarajNo ratings yet
- BonesDocument14 pagesBonesuthsala7123No ratings yet
- Trail Guide To The Body - Sample PDFDocument4 pagesTrail Guide To The Body - Sample PDFАлексNo ratings yet
- CasePreFinal MC DraftDocument21 pagesCasePreFinal MC DraftJohn Ephraim AlvizNo ratings yet
- Ana - Joints ClassificationsDocument12 pagesAna - Joints ClassificationsMahmoud hilmyNo ratings yet
- Practical 2 - Arthrology of Upper LimbDocument2 pagesPractical 2 - Arthrology of Upper LimbFathimath iba AhmedNo ratings yet
- Anatomy Skeletal System NotesDocument6 pagesAnatomy Skeletal System NotesrincyNo ratings yet
- Anatomy Foot SummaryDocument3 pagesAnatomy Foot SummaryJerico CaragNo ratings yet
- 10 1016@j Cps 2019 02 006Document9 pages10 1016@j Cps 2019 02 006Deborah SalinasNo ratings yet
- The Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic AnatomyDocument50 pagesThe Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic Anatomyspeedy.catNo ratings yet
- HiDocument8 pagesHibaoNo ratings yet
- Maxillary Local AnestheticsDocument2 pagesMaxillary Local Anestheticsnelsona10No ratings yet
- Exercise Science Section 2: The Skeletal System: An Introduction To Health and Physical EducationDocument32 pagesExercise Science Section 2: The Skeletal System: An Introduction To Health and Physical EducationKeren HZNo ratings yet
- Assignment CL7 Hand - 2021-2022Document6 pagesAssignment CL7 Hand - 2021-2022ARYSSA BINTI AZRINo ratings yet
- Foot Muscles ChartsDocument6 pagesFoot Muscles ChartsddNo ratings yet
- Spine: Erector Spinae Group - EsgDocument1 pageSpine: Erector Spinae Group - Esgjmccoy26No ratings yet
- True Oral CavityDocument3 pagesTrue Oral CavityHanneke Du PlessisNo ratings yet
- Ankle: Radiographs : Plates 506, 513, 514Document6 pagesAnkle: Radiographs : Plates 506, 513, 514RenatoNo ratings yet
- 5 - Joints, Muscle Tissue, Muscle SystemDocument227 pages5 - Joints, Muscle Tissue, Muscle SystemTracy NguyenNo ratings yet
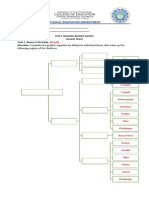
- LUBANG - Israel - BSEE - 1A (P.E)Document5 pagesLUBANG - Israel - BSEE - 1A (P.E)Kathleen MelendrezNo ratings yet
- Epithelial Tissue Connective Tissue: Desmosomes Tight Junctions Gap JunctionsDocument1 pageEpithelial Tissue Connective Tissue: Desmosomes Tight Junctions Gap JunctionsJalen GalvezNo ratings yet
- Hand and Foot AnatomyDocument1 pageHand and Foot AnatomyMike BozinNo ratings yet
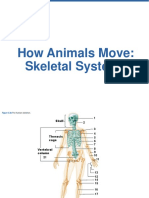
- How Animals Move: Skeletal SystemsDocument60 pagesHow Animals Move: Skeletal SystemsKristel Lao-asNo ratings yet
- JointDocument10 pagesJointmay498550No ratings yet
- Kent Chapter 9 Part 2Document11 pagesKent Chapter 9 Part 2bazingaNo ratings yet
- 07d - Spinal Cord - Reflexes - Ninja Nerd & DR NajeebDocument7 pages07d - Spinal Cord - Reflexes - Ninja Nerd & DR Najeebhiba jasimNo ratings yet
- Mccormick2010 PDFDocument9 pagesMccormick2010 PDFkeang zhuNo ratings yet
- PNS Somatic Motor System (SKELETAL MUSCLE)Document3 pagesPNS Somatic Motor System (SKELETAL MUSCLE)wardahafif00No ratings yet
- BIOS1168 Functional Musculoskeletal Anatomy ADocument23 pagesBIOS1168 Functional Musculoskeletal Anatomy ALachlan NguyenNo ratings yet
- Colouring Tower Bridge Cat and Baby Whale With TitleDocument1 pageColouring Tower Bridge Cat and Baby Whale With TitleFrank MoraNo ratings yet
- Otters: An Action Plan For Their ConservationDocument133 pagesOtters: An Action Plan For Their ConservationFrank MoraNo ratings yet
- Ground Hogs and Their BehaviorDocument4 pagesGround Hogs and Their BehaviorFrank MoraNo ratings yet
- GenMathG11 Q2 Mod10 Logic Version2WO-AKDocument40 pagesGenMathG11 Q2 Mod10 Logic Version2WO-AKFrank MoraNo ratings yet
- Takei 1985Document7 pagesTakei 1985Paula Francisca Moraga HidalgoNo ratings yet
- Wound Healing and Its Complications - 2Document28 pagesWound Healing and Its Complications - 2Devanand KumarNo ratings yet
- Dr. R.K. Behera Medical Referee E.S.I. Corporation, OrissaDocument15 pagesDr. R.K. Behera Medical Referee E.S.I. Corporation, OrissasureesicNo ratings yet
- CATALOG CONMED 2011 - ElectrosurgeryDocument42 pagesCATALOG CONMED 2011 - Electrosurgeryfrancheska bacaNo ratings yet
- BIOPSYDocument7 pagesBIOPSYjmskdlnNo ratings yet
- Aesthetic Zone Shakeel ShahdadDocument3 pagesAesthetic Zone Shakeel ShahdadAhsan NaseerNo ratings yet
- Bone Grafting HCP Spine Marrow Cellution Bma Surgical Technique Guide Pmd018207Document16 pagesBone Grafting HCP Spine Marrow Cellution Bma Surgical Technique Guide Pmd018207Satyam PatelNo ratings yet
- Abdomen-Clinicals - PDF Version 1Document11 pagesAbdomen-Clinicals - PDF Version 1hamzabhayatNo ratings yet
- Abstract 11Document2 pagesAbstract 11LarisjoursNo ratings yet
- CTEV - Physical TherapyDocument16 pagesCTEV - Physical TherapyHUZAIFA YAMAANNo ratings yet
- Tool For Situational Analysis To Assess Emergency and Essential Surgical CareDocument4 pagesTool For Situational Analysis To Assess Emergency and Essential Surgical CareGanashiam NadarasaNo ratings yet
- Test Your Coding Knowledge ResultsDocument7 pagesTest Your Coding Knowledge ResultsPra Vî ThaNo ratings yet
- Cataract: LEO Clinical Topic UpdateDocument25 pagesCataract: LEO Clinical Topic UpdateRaúl Plasencia SaliniNo ratings yet
- Eras PPDocument24 pagesEras PPkiemdinhit7No ratings yet
- Surgery-First Orthognathic Approach For The Correction of FacialDocument8 pagesSurgery-First Orthognathic Approach For The Correction of FacialMario CastellanosNo ratings yet
- Operation Theatre ComplexDocument26 pagesOperation Theatre ComplexS AkashNo ratings yet
- Literature Review On Effective Use of Modern Modalities in Management of Intra-Axial Brain LesionsDocument11 pagesLiterature Review On Effective Use of Modern Modalities in Management of Intra-Axial Brain LesionsScientific PapersNo ratings yet
- ICD9CM (Gandi)Document39 pagesICD9CM (Gandi)casemik RSUDKarangasemNo ratings yet
- Icd 9 CM Keterangan Di Icd 9 CM: Drainage Abscess Pada Mandibula / Sub MandibulaDocument2 pagesIcd 9 CM Keterangan Di Icd 9 CM: Drainage Abscess Pada Mandibula / Sub Mandibulanoerrekmed_816409184No ratings yet
- 3 PROXIMAL BOX ELEVATIONAND BIOLOGICAL WIDTH CLINICAL R2 TECHNIQUE Frese2013 PDFDocument10 pages3 PROXIMAL BOX ELEVATIONAND BIOLOGICAL WIDTH CLINICAL R2 TECHNIQUE Frese2013 PDFjhon HanselNo ratings yet
- Comparison of MMS and CL GradingDocument8 pagesComparison of MMS and CL GradingIndhu SubbuNo ratings yet
- Litrature & Case StudyDocument74 pagesLitrature & Case Studynaol buloNo ratings yet
- The Skull3Document10 pagesThe Skull3Mokhtar SinanNo ratings yet
- PaperHospital Frontiers Capacity ManagementDocument58 pagesPaperHospital Frontiers Capacity ManagementCOVID RSHJNo ratings yet
- Endo SurgeryDocument5 pagesEndo Surgeryahmed muhammadNo ratings yet
- Cleveland Clinic Summer Scholars ProgramDocument6 pagesCleveland Clinic Summer Scholars Programrsk619504No ratings yet
- Evaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss A Systematic Review and Meta-AnalysisDocument9 pagesEvaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss A Systematic Review and Meta-AnalysisJuan Andres EspinozaNo ratings yet
- Sialolithiasis: Vi Ugboko Fmcds FwacsDocument47 pagesSialolithiasis: Vi Ugboko Fmcds FwacsAkeem Alawode50% (2)
- Bailey Loves Short Practice of Surgery 25th EditiDocument2 pagesBailey Loves Short Practice of Surgery 25th EditiSpiderman EvansNo ratings yet
- 封面Document5 pages封面xiaoxin zhang100% (1)