Download as pptx, pdf, or txt
You might also like
- Day 1 Mission NEETPGDocument142 pagesDay 1 Mission NEETPGKalyan SagarNo ratings yet
- Case PresentationDocument25 pagesCase PresentationMuhammad Hammad100% (1)
- Anatomy & Physiology URINARY TRACTDocument28 pagesAnatomy & Physiology URINARY TRACTabdullatifNo ratings yet
- Gross Anatomy and Histolgy of UrinarysystemDocument81 pagesGross Anatomy and Histolgy of UrinarysystemIncredible DivineNo ratings yet
- Anatomy of Urinary Bladder and UrethraDocument41 pagesAnatomy of Urinary Bladder and UrethraHemanta PunNo ratings yet
- Nephron CompressDocument91 pagesNephron CompressAlligator ZNo ratings yet
- 7.1 Urinary f2f s1b2-23Document47 pages7.1 Urinary f2f s1b2-23shlokNo ratings yet
- Renal&Urinary System 2012Document64 pagesRenal&Urinary System 2012Meilani PutriNo ratings yet
- Yuniarti: Anatomy Department Faculty of Medicine UnisbaDocument40 pagesYuniarti: Anatomy Department Faculty of Medicine UnisbaalgutNo ratings yet
- Lect 4 Urinary SystemDocument42 pagesLect 4 Urinary Systemnightter4No ratings yet
- Anatomy of Urinary SystemDocument43 pagesAnatomy of Urinary SystemIrfan Ali JunejoNo ratings yet
- 1 KidneyDocument49 pages1 Kidneywcbkk4vt9fNo ratings yet
- URS SummaryDocument26 pagesURS SummaryMohamed HaridyNo ratings yet
- Anatomy of The Kidney & Ureter - NewDocument42 pagesAnatomy of The Kidney & Ureter - NewHaider Nadhem AL-rubai0% (1)
- Urinary SystemDocument19 pagesUrinary Systemadnanahmed9107No ratings yet
- DR Laxman Khanal Bpkihs 07-06-2013Document86 pagesDR Laxman Khanal Bpkihs 07-06-2013Bilal YimamNo ratings yet
- Urinary SystemDocument55 pagesUrinary SystemChristian UdaundoNo ratings yet
- Urinary System: Prepared By: Ma. Concepcion F. Columbres, MNDocument38 pagesUrinary System: Prepared By: Ma. Concepcion F. Columbres, MNAl Serenoso100% (1)
- 4urinarysystem 170708071824Document42 pages4urinarysystem 170708071824Pooja DesaiNo ratings yet
- Urinary SystemDocument30 pagesUrinary SystemTamiru KetemaNo ratings yet
- Gross Anatomy Urinary SystemDocument43 pagesGross Anatomy Urinary SystemMay LacdaoNo ratings yet
- L31 - Renal SystemDocument30 pagesL31 - Renal SystemsairahhannahNo ratings yet
- Anatomy and Physiology of Urinary SystemDocument53 pagesAnatomy and Physiology of Urinary SystemArathy KalathingalNo ratings yet
- 4.kidneys, Ureters and Suprarenal GlandsDocument57 pages4.kidneys, Ureters and Suprarenal GlandsIshimwe TheotimeNo ratings yet
- UT AnatomyDocument35 pagesUT AnatomyAngel SaraNo ratings yet
- UGS - MaleDocument44 pagesUGS - MaleSʌɩĸʌt PʌʋɭNo ratings yet
- Urinary System: Mr. Visanth V S Mayo School of Nursing LucknowDocument42 pagesUrinary System: Mr. Visanth V S Mayo School of Nursing LucknowJoshua RuntuweneNo ratings yet
- Urinary SystemDocument31 pagesUrinary SystemAyro Business CenterNo ratings yet
- Pancreas 2017Document53 pagesPancreas 2017yasrul izadNo ratings yet
- Renal Physiology 1 1aDocument88 pagesRenal Physiology 1 1afentaw melkieNo ratings yet
- Urinary System: DR Eid Nassar Ali Anatomy Department Taibah UniversityDocument18 pagesUrinary System: DR Eid Nassar Ali Anatomy Department Taibah UniversityAbdulrahman MohammedNo ratings yet
- UrinaryDocument76 pagesUrinaryJasmin StojadinovicNo ratings yet
- 6 - Renal SystemDocument32 pages6 - Renal Systemmaraym AbdullAalhNo ratings yet
- Abdomen Dan PelvisDocument64 pagesAbdomen Dan PelvisRachmad RasidinNo ratings yet
- RENALDocument29 pagesRENALJenica SorianoNo ratings yet
- Anatomy of GALL BLADDER PANCREAS 2016Document32 pagesAnatomy of GALL BLADDER PANCREAS 2016Omar Ali AyoubkhanNo ratings yet
- The Urinary SystemDocument66 pagesThe Urinary Systemapi-26587879No ratings yet
- Lect4 PelvisDocument26 pagesLect4 PelvisasakingofhNo ratings yet
- The Anatomy, Histology and Development of The Kidney PDFDocument14 pagesThe Anatomy, Histology and Development of The Kidney PDFredderdatNo ratings yet
- Kidney and Ureter For Paramedical StudentsDocument53 pagesKidney and Ureter For Paramedical Studentslakshmiraman1770No ratings yet
- Anatomy RCR1 RenalDocument3 pagesAnatomy RCR1 RenaleamcrawleyNo ratings yet
- Renal Calculi SangeetaDocument43 pagesRenal Calculi Sangeetadilraj77177No ratings yet
- Urogenital SystemDocument106 pagesUrogenital SystemBen MasungcadNo ratings yet
- Anatomy of Excretory SystemDocument12 pagesAnatomy of Excretory SystemSANJEEVA REDDYNo ratings yet
- 2 Ureter, Urinary Bladder and Urethra XJGDocument51 pages2 Ureter, Urinary Bladder and Urethra XJGwcbkk4vt9fNo ratings yet
- The Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin UniversityDocument44 pagesThe Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin UniversityRahmawati HamudiNo ratings yet
- Urinary System ArlendsDocument55 pagesUrinary System ArlendslionioniNo ratings yet
- General Anatomy of Urinary SystemDocument62 pagesGeneral Anatomy of Urinary SystemSARABIA, ARVIN JR.No ratings yet
- Anatomy of The Renal SystemDocument67 pagesAnatomy of The Renal SystemRIUNGU PENINAH GATWIRINo ratings yet
- Apparatus Uro Genital IsDocument32 pagesApparatus Uro Genital IsNelli NémethNo ratings yet
- Retroperitonium: Yosef TadesseDocument94 pagesRetroperitonium: Yosef Tadessetesfaye mekonnenNo ratings yet
- Jigjiga University College of Veterinary Medicine: by DR Mahamud A. (DVM, MSC)Document56 pagesJigjiga University College of Veterinary Medicine: by DR Mahamud A. (DVM, MSC)Shemsu LoveNo ratings yet
- Urinary SystemDocument71 pagesUrinary SystemyewollolijfikreNo ratings yet
- GUS1 - K2 - Hystology Kul Gus 2012Document62 pagesGUS1 - K2 - Hystology Kul Gus 2012Thamarai SomuNo ratings yet
- Anatomy of Urinary SystemDocument43 pagesAnatomy of Urinary Systemandrea titus100% (1)
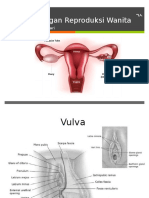
- 01 Anatomy of Female Genital System DR - OsmaDocument69 pages01 Anatomy of Female Genital System DR - OsmaAyalewNo ratings yet
- Renal SysDocument38 pagesRenal Syscharlesnti1990No ratings yet
- Urinary System PearsonsDocument13 pagesUrinary System Pearsonsblando.shaneNo ratings yet
- 1 Anatomi Organ PanggulDocument45 pages1 Anatomi Organ PanggulHutomo Budi Hasnian SyahNo ratings yet
- Cardiology Board Review 2E Mar 21 2023 - 1119814944 - Wiley Blackwell Ramdas G Pai Full ChapterDocument51 pagesCardiology Board Review 2E Mar 21 2023 - 1119814944 - Wiley Blackwell Ramdas G Pai Full Chapterdouglas.zimmer226100% (19)
- Pharmacology Cardiovascular DrugsDocument27 pagesPharmacology Cardiovascular DrugsMitzel AlvaranNo ratings yet
- Clinical Microscopy Handouts2016Document23 pagesClinical Microscopy Handouts2016Leila PasigadoNo ratings yet
- Cardiac Function: Unice L. Padilla, RMT, MSMTDocument15 pagesCardiac Function: Unice L. Padilla, RMT, MSMTShiki Asagami BrunestedNo ratings yet
- Unit 1 AnswerDocument22 pagesUnit 1 Answerii Dr3slNo ratings yet
- Body Systems: By: Veda PurnithaDocument60 pagesBody Systems: By: Veda PurnithaVeda PurnithaNo ratings yet
- Case Study On Bilateral NephrolithiasisDocument85 pagesCase Study On Bilateral NephrolithiasisShoixi ⎝⓿⏝⓿⎠100% (1)
- 12 Lead Electrocardiogram (Ecg) Placement: Module DescriptionDocument11 pages12 Lead Electrocardiogram (Ecg) Placement: Module DescriptionHanna La MadridNo ratings yet
- Indian Journal of Physiotherapy and Occupational Therapy July-Sep 2009 PDFDocument116 pagesIndian Journal of Physiotherapy and Occupational Therapy July-Sep 2009 PDFAshoka VanjareNo ratings yet
- TDM of DigoxinDocument13 pagesTDM of DigoxinMounika16 PedamalluNo ratings yet
- 2.health AssessmentDocument7 pages2.health Assessment2BGrp3Plaza, Anna MaeNo ratings yet
- Guía AASLD DG, Evaluación y Manejo de Ascitis, PBE y SHR HepatologyDocument27 pagesGuía AASLD DG, Evaluación y Manejo de Ascitis, PBE y SHR Hepatologyjavier GarcíaNo ratings yet
- Nonopiod Analgesics - Salicylates and Non SalicylatesDocument6 pagesNonopiod Analgesics - Salicylates and Non Salicylatesaday25No ratings yet
- Comparitive Study of Commercial Antacids CBSE Class 12 ProjectDocument34 pagesComparitive Study of Commercial Antacids CBSE Class 12 ProjectROMAN REIGNSNo ratings yet
- Cardiac PacemakerDocument24 pagesCardiac PacemakerRitima JainNo ratings yet
- Anaesthetic Concern For One Lung Ventilation: By-Dr - Bhushan Kinge, M.D. Ims - Bhu, VaranasiDocument57 pagesAnaesthetic Concern For One Lung Ventilation: By-Dr - Bhushan Kinge, M.D. Ims - Bhu, VaranasifaisalnaseemkhanNo ratings yet
- Hypertension in Adolescents and Young Adults Referred To A Tertiary Hypertension Clinic in Cape Town, South AfricaDocument5 pagesHypertension in Adolescents and Young Adults Referred To A Tertiary Hypertension Clinic in Cape Town, South AfricahanifahNo ratings yet
- Anatomy and Physiology GMCDocument15 pagesAnatomy and Physiology GMCsamantha tanoNo ratings yet
- Perioperative Medicines Management V8Document7 pagesPerioperative Medicines Management V8Waleed Ahmad.No ratings yet
- Cardiovascular SystemDocument10 pagesCardiovascular SystemitsmesuvekshaNo ratings yet
- DVT and TestsDocument4 pagesDVT and TestsvishwanathNo ratings yet
- Cor Pulmonale - Introduction To Cor Pulmonale, Etiology and Pathophysiology of Cor Pulmonale, Epidemiology of Cor PulmonaleDocument18 pagesCor Pulmonale - Introduction To Cor Pulmonale, Etiology and Pathophysiology of Cor Pulmonale, Epidemiology of Cor PulmonaleRicky SpideyNo ratings yet
- USMLE WORLD QUESTIONS QuizletDocument87 pagesUSMLE WORLD QUESTIONS QuizletPatricio AlexanderNo ratings yet
- Management of Acute Heart Failure: Anna Fuji Rahimah M. Saifur RohmanDocument27 pagesManagement of Acute Heart Failure: Anna Fuji Rahimah M. Saifur Rohmanwwn thokNo ratings yet
- Blood Groups and Blood TransfusionDocument18 pagesBlood Groups and Blood TransfusionAbdul HafeezNo ratings yet
- Journal Reading Ilmu Penyakit DalamDocument15 pagesJournal Reading Ilmu Penyakit DalamSeffia riandiniNo ratings yet
- Anatomical Descriptive Source - Integumentary Skin, Tissue, and CellsDocument6 pagesAnatomical Descriptive Source - Integumentary Skin, Tissue, and CellsGURPARABJOT KAURNo ratings yet
- Latihan Abbreviation 2Document2 pagesLatihan Abbreviation 2Sherly AmeliaNo ratings yet