Download as ppt, pdf, or txt
You might also like
- HFS HOT Vendors Hfs Hot Vendors Compendium 2018 2021 RS 2106 v1.0FINALDocument211 pagesHFS HOT Vendors Hfs Hot Vendors Compendium 2018 2021 RS 2106 v1.0FINALVidhya Charan PNo ratings yet
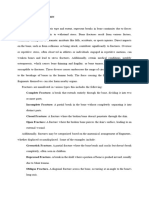
- All About FractureDocument59 pagesAll About FractureJohn John Torres100% (1)
- 3.1 Critical Understanding and Application of Motivation in OrganizationDocument3 pages3.1 Critical Understanding and Application of Motivation in OrganizationApril Mendoza-Conrada0% (1)
- Life 2e - Beginner - Unit 1 Test - WordDocument7 pagesLife 2e - Beginner - Unit 1 Test - WordHuy TrannNo ratings yet
- Part Iv: Development Plans of The Ipcrf (Ipcrf-Dp)Document1 pagePart Iv: Development Plans of The Ipcrf (Ipcrf-Dp)rushel lazaro92% (153)
- 02 Celeste Shichi Da MethodDocument9 pages02 Celeste Shichi Da MethodhiteshcparmarNo ratings yet
- Nursing Care of A Child With FractureDocument40 pagesNursing Care of A Child With FractureSomyee Pachuau100% (2)
- Orthopedic NursingDocument23 pagesOrthopedic Nursinggabrielle magdaraog100% (1)
- Fracturesgoutosteosprain 2Document199 pagesFracturesgoutosteosprain 2Rose Cristille Yeso JocsonNo ratings yet
- Bone FractureDocument10 pagesBone FractureDat boi100% (1)
- Frakktur Kelompok 15 (English) PDFDocument45 pagesFrakktur Kelompok 15 (English) PDFTri WulandariSemester 1BNo ratings yet
- Fractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaDocument50 pagesFractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaJustin Ahorro-DionisioNo ratings yet
- Fracture Nursing Care Management: Study GuideDocument5 pagesFracture Nursing Care Management: Study Guidezahwa ayundaNo ratings yet
- FractureDocument4 pagesFractureCandra P0% (1)
- Fracture: Group 1Document29 pagesFracture: Group 1Louisse Angeli AbucejoNo ratings yet
- Types of FracturesDocument10 pagesTypes of Fracturesazeencancer2003No ratings yet
- Fracture Slide BasisDocument44 pagesFracture Slide BasisKing Aldus ConstantinoNo ratings yet
- تروما محاضرة 1Document58 pagesتروما محاضرة 1202003339No ratings yet
- NCP: Nursing Care Plan For Bone FracturesDocument8 pagesNCP: Nursing Care Plan For Bone FracturesElham TabaoNo ratings yet
- Musculoskeletal Disorders FRACTURESDocument10 pagesMusculoskeletal Disorders FRACTURESرافت العواضيNo ratings yet
- WK 2 NFK 202Document88 pagesWK 2 NFK 202JSeasharkNo ratings yet
- Bone FracturesDocument26 pagesBone FracturesgwynNo ratings yet
- FrakturDocument188 pagesFrakturSiti RaihanatiNo ratings yet
- FractureDocument27 pagesFractureAkio OzaragaNo ratings yet
- Fractures: Types, Complications, and ManagementDocument26 pagesFractures: Types, Complications, and Managementsm - kardmNo ratings yet
- FRACTURESDocument35 pagesFRACTURESMichelle DuNo ratings yet
- Arm:Leg Fracture PDFDocument11 pagesArm:Leg Fracture PDFHannaNo ratings yet
- Fracture Case AbstractDocument27 pagesFracture Case AbstractMaribel Briones JuanNo ratings yet
- Last Updated Thu 30 March 2017 by Christian Nordqvist Reviewed by William Morrison, MDDocument5 pagesLast Updated Thu 30 March 2017 by Christian Nordqvist Reviewed by William Morrison, MDScarlett EscamillaNo ratings yet
- Year 2 Semester 2Document88 pagesYear 2 Semester 2JSeasharkNo ratings yet
- Fracture PresentationDocument58 pagesFracture Presentationshejila c hNo ratings yet
- Care StudyDocument27 pagesCare StudyFavourNo ratings yet
- Dislocation (Def, Etio, Cla, RF, CMD)Document13 pagesDislocation (Def, Etio, Cla, RF, CMD)miftajnh2No ratings yet
- Orthopedic NursingDocument19 pagesOrthopedic NursingDa BondadNo ratings yet
- Fracture PresentationDocument53 pagesFracture Presentationrahul yadav100% (8)
- Skeletal DisorderDocument7 pagesSkeletal Disorderhxqf25mbvvNo ratings yet
- Introduction To Fracture: Parathyroid Hormone CalcitoninDocument36 pagesIntroduction To Fracture: Parathyroid Hormone CalcitoninArlene Ferrer100% (1)
- A Closed Fracture Does Not Penetrate The SkinDocument5 pagesA Closed Fracture Does Not Penetrate The SkinIvan Liquiran Avenado100% (1)
- Types: There Is A Range Of, IncludingDocument15 pagesTypes: There Is A Range Of, IncludingBhossneil Betonio LacadenNo ratings yet
- Bone FractureDocument23 pagesBone FractureClifford GulfanNo ratings yet
- Fracture 01Document42 pagesFracture 01api-19916399No ratings yet
- Fracture and Joint Injuries (Shalter-Chapter 15) - Kelompok C (Dr. Oktavianus, SP - Ot)Document69 pagesFracture and Joint Injuries (Shalter-Chapter 15) - Kelompok C (Dr. Oktavianus, SP - Ot)Heru ChrisNo ratings yet
- Complete FractureDocument10 pagesComplete FractureSimran JosanNo ratings yet
- FractureDocument125 pagesFractureKlara Devina VanessaNo ratings yet
- Bone FractureDocument10 pagesBone Fractureraphael chidiebereNo ratings yet
- Fractures and Low Back Pain: Dr. Lubna DwerijDocument49 pagesFractures and Low Back Pain: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Fractures Pathophysiology Treatment and Nursing CareDocument9 pagesFractures Pathophysiology Treatment and Nursing Careaddica0% (1)
- Principles of Fractures: (Continued)Document44 pagesPrinciples of Fractures: (Continued)Abdi Ñãśìr Møhàmèď ŚàĺàhNo ratings yet
- PEMBAHASAN EnglishDocument12 pagesPEMBAHASAN EnglishEinz Nur Amalyah IdrusNo ratings yet
- Fracture IntroductionDocument21 pagesFracture IntroductionJonathan Delos ReyesNo ratings yet
- 3-Fracture 1Document36 pages3-Fracture 1Radwa TalaatNo ratings yet
- Fracture FinalDocument56 pagesFracture FinalnobelaugustineNo ratings yet
- Fractures and DislocationsDocument53 pagesFractures and Dislocationsagha_sajjad90No ratings yet
- Fracture: Edfran Jed A. Serino MSN 303Document34 pagesFracture: Edfran Jed A. Serino MSN 303Edfran Jed SerinoNo ratings yet
- Orthopaedic SlidesDocument163 pagesOrthopaedic SlidesVivian ChepkemeiNo ratings yet
- Case Reportgode OrifDocument35 pagesCase Reportgode OrifFitaNo ratings yet
- Nursing Care Plan With A FractureDocument11 pagesNursing Care Plan With A FractureHasanah EkaNo ratings yet
- MusculoskelealDocument32 pagesMusculoskelealEbuka AniNo ratings yet
- Musculoskeletal Disorders: Assessment and Diagnostic Test AssessmentDocument10 pagesMusculoskeletal Disorders: Assessment and Diagnostic Test AssessmentAl-Mansor MoayadNo ratings yet
- My Lesson Plan: Closed Fracture Distal 3rd Right Radius Ulna, Secondary To FallDocument6 pagesMy Lesson Plan: Closed Fracture Distal 3rd Right Radius Ulna, Secondary To Fallshenecajean carajayNo ratings yet
- Bone FractureDocument6 pagesBone FractureNetz ProtomartirNo ratings yet
- Saraf LBM 3Document4 pagesSaraf LBM 3cheesekejuNo ratings yet
- Neurologic ExaminationDocument3 pagesNeurologic ExaminationDap Dap DogelioNo ratings yet
- Surgery WorkDocument9 pagesSurgery WorkHigh TechNo ratings yet
- Are You Okay? Sports Injuries: Causes, Types and Treatment - Sports Book 4th Grade | Children's Sports & OutdoorsFrom EverandAre You Okay? Sports Injuries: Causes, Types and Treatment - Sports Book 4th Grade | Children's Sports & OutdoorsNo ratings yet
- 2renr Practice Test 6 FinalDocument14 pages2renr Practice Test 6 Finalta CNo ratings yet
- 2renr Practice Test 5 FinalDocument14 pages2renr Practice Test 5 Finalta C100% (1)
- Neurological 5Document39 pagesNeurological 5ta CNo ratings yet
- Care of The Unconscious PatientDocument33 pagesCare of The Unconscious Patientta CNo ratings yet
- Crisis InterventionDocument11 pagesCrisis Interventionta CNo ratings yet
- Community Assessment MethodsDocument8 pagesCommunity Assessment Methodsta CNo ratings yet
- Cancer Lesson Plan - Tutor1Document7 pagesCancer Lesson Plan - Tutor1ta CNo ratings yet
- Neurological Disorders 1Document110 pagesNeurological Disorders 1ta CNo ratings yet
- Sensory System - Common Traumatic Eye InjuriesDocument17 pagesSensory System - Common Traumatic Eye Injuriesta CNo ratings yet
- Community Health OutlineDocument4 pagesCommunity Health Outlineta CNo ratings yet
- Spinal Cord InjuryDocument9 pagesSpinal Cord Injuryta CNo ratings yet
- Respiratory FailureDocument5 pagesRespiratory Failureta CNo ratings yet
- Growth & Development of An Adolescent (2380)Document8 pagesGrowth & Development of An Adolescent (2380)ta CNo ratings yet
- Cataract Cataracts CataractDocument6 pagesCataract Cataracts Cataractta CNo ratings yet
- Growth & Development of A PreschoolerDocument6 pagesGrowth & Development of A Preschoolerta CNo ratings yet
- Female Reproducvtive DisordersDocument76 pagesFemale Reproducvtive Disordersta CNo ratings yet
- Is (0.1 - 1 MM Thick) Dermis - Contains Blood Vessels, Veins, Nerve Endings, SebaceousDocument10 pagesIs (0.1 - 1 MM Thick) Dermis - Contains Blood Vessels, Veins, Nerve Endings, Sebaceousta CNo ratings yet
- Growth & Development School-AgeDocument9 pagesGrowth & Development School-Ageta CNo ratings yet
- Female ReproductiveDocument13 pagesFemale Reproductiveta CNo ratings yet
- Female and Male Reproductive (2224)Document20 pagesFemale and Male Reproductive (2224)ta CNo ratings yet
- Endometiosis Tutorial: Adult Nursing 2Document9 pagesEndometiosis Tutorial: Adult Nursing 2ta CNo ratings yet
- Coarctation of The Aorta: PathophysiologyDocument2 pagesCoarctation of The Aorta: Pathophysiologyta CNo ratings yet
- Teaching Pack: Cambridge IGCSE Literature in English 0475Document15 pagesTeaching Pack: Cambridge IGCSE Literature in English 0475RoseNo ratings yet
- 2-List of Degree College - Updated PDFDocument20 pages2-List of Degree College - Updated PDFTop ToonsNo ratings yet
- Journal of Advanced Computing and Communication Technologies (ISSNDocument5 pagesJournal of Advanced Computing and Communication Technologies (ISSNzoe regina castroNo ratings yet
- Majestic Interview CallDocument7 pagesMajestic Interview CallAbrar Hussain KhanNo ratings yet
- MlopDocument28 pagesMlopShaileshAgrawalNo ratings yet
- Zoom Masters PDFDocument24 pagesZoom Masters PDFshirin subaidaNo ratings yet
- Clinical Pharmacy Practice: Prepared By: Cedrix Cuaderno RPH, Bs Ind Pharm. Adamson University College of PharmacyDocument30 pagesClinical Pharmacy Practice: Prepared By: Cedrix Cuaderno RPH, Bs Ind Pharm. Adamson University College of PharmacyCedrix CuadernoNo ratings yet
- Master Prospectus 2020Document90 pagesMaster Prospectus 2020Fatima JahangirNo ratings yet
- SLM-E9Q3-MODULE 8 - STestDocument4 pagesSLM-E9Q3-MODULE 8 - STestCarlo MoratallaNo ratings yet
- Article On PrecisDocument3 pagesArticle On PrecisHemantVermaNo ratings yet
- Rough DraftDocument7 pagesRough Draftapi-406028508No ratings yet
- Perspectives On Pedagogical Grammar 0521445302 0521449901 CompressDocument171 pagesPerspectives On Pedagogical Grammar 0521445302 0521449901 CompressKhurram MalikNo ratings yet
- NUR 200 Week 9 Practice Case StudyDocument3 pagesNUR 200 Week 9 Practice Case StudyJB NicoleNo ratings yet
- A List of Highly in Uential Biomedical Researchers Until2011Document27 pagesA List of Highly in Uential Biomedical Researchers Until2011Hua Hidari YangNo ratings yet
- MSC Introduction To Syntax: Lecture 1: What Syntax Is About What Is This Module About?Document6 pagesMSC Introduction To Syntax: Lecture 1: What Syntax Is About What Is This Module About?نور عبداللهNo ratings yet
- Flag Ceremony GuidelinesDocument3 pagesFlag Ceremony GuidelinesRyan Nicolas PastoleroNo ratings yet
- RMA Process Complete Flow SampleDocument2 pagesRMA Process Complete Flow SampleBharathNo ratings yet
- Caregive R Robots: Maha-Abeer OCS:6Document22 pagesCaregive R Robots: Maha-Abeer OCS:6maha abdullahNo ratings yet
- DLL - Science 6 - Q2 - W1Document6 pagesDLL - Science 6 - Q2 - W1carmina duldulaoNo ratings yet
- Eportfolio New CmaDocument2 pagesEportfolio New Cmaapi-318874763No ratings yet
- Philosophical FilmsDocument3 pagesPhilosophical FilmsMaria Diory RabajanteNo ratings yet
- Teste SNAP-IV e SWAN - ManualDocument20 pagesTeste SNAP-IV e SWAN - ManualAnastasio umNo ratings yet
- Test Driven Development - TDD & ATDDDocument23 pagesTest Driven Development - TDD & ATDDWael ANIBA100% (1)
- I Am The GrassDocument4 pagesI Am The GrassAurelian Ovidiu JuncNo ratings yet
- Context Clues PDFDocument48 pagesContext Clues PDFicaNo ratings yet