Download as pptx, pdf, or txt
You might also like
- Auditory Verbal+Therapy+Science,+Research+and+Practice+by+Warren+Estabrooks,+Helen+McCaffrey+Morrison,+Karen+MacIver LuxDocument1,052 pagesAuditory Verbal+Therapy+Science,+Research+and+Practice+by+Warren+Estabrooks,+Helen+McCaffrey+Morrison,+Karen+MacIver LuxAndra Hazaparu100% (1)
- Ganong MCQ + Answer PDFDocument72 pagesGanong MCQ + Answer PDFمحمد عبدالله ابراهيم عبدالله81% (16)
- Sudden Sensorineural Hearing Loss: Christopher D. Muller, M.D. Jeffrey Vrabec, M.DDocument64 pagesSudden Sensorineural Hearing Loss: Christopher D. Muller, M.D. Jeffrey Vrabec, M.DDrKunal KaradeNo ratings yet
- Pearsons Et Al. - 1977 - Speech Levels in Various Noise EnvironmentsDocument82 pagesPearsons Et Al. - 1977 - Speech Levels in Various Noise EnvironmentsRalph MuehleisenNo ratings yet
- Iloilo City Regulation Ordinance 2015-162Document6 pagesIloilo City Regulation Ordinance 2015-162Iloilo City Council100% (4)
- Physical DisabilityDocument18 pagesPhysical DisabilityjessaNo ratings yet
- Reflex Measurements: Quick GuideDocument10 pagesReflex Measurements: Quick GuidefilippobNo ratings yet
- Aspects of Hearing Aids Fitting ProceduresDocument150 pagesAspects of Hearing Aids Fitting ProceduresakNo ratings yet
- Auditory Evoked Potentials - AEPs - Underlying PrinciplesDocument19 pagesAuditory Evoked Potentials - AEPs - Underlying PrinciplesMansi SinghNo ratings yet
- Hearing Losses and Assocated CorealtesDocument3 pagesHearing Losses and Assocated CorealtesAchu SachuNo ratings yet
- Otoacoustic Emissions From MedscapeDocument5 pagesOtoacoustic Emissions From MedscapeMin-Joo Esther ParkNo ratings yet
- Oae Presentation,/ Kunnampallil GejoDocument69 pagesOae Presentation,/ Kunnampallil GejoKUNNAMPALLIL GEJO JOHN100% (1)
- Slow Auditory Evoked Potentials (1 InterligneDocument8 pagesSlow Auditory Evoked Potentials (1 Interligner.boniver524No ratings yet
- ASSR Thresholds PDFDocument7 pagesASSR Thresholds PDFDaniela Garrido GonzálezNo ratings yet
- Craniofacial Osteotomies For Hidden Head & Neck LesionsDocument4 pagesCraniofacial Osteotomies For Hidden Head & Neck LesionsMohammad AkheelNo ratings yet
- Deglutition Reflex - LectureDocument38 pagesDeglutition Reflex - LectureasaadsarfrazNo ratings yet
- Hearing Loss: Mubarak MD Dhawal Mbbs (Iua), Morl (Mak) ENT Lecturer April 2019Document46 pagesHearing Loss: Mubarak MD Dhawal Mbbs (Iua), Morl (Mak) ENT Lecturer April 2019gibreilNo ratings yet
- Audiometric Testing of AdultsDocument6 pagesAudiometric Testing of AdultssofiameNo ratings yet
- Cochlear ImplantDocument5 pagesCochlear ImplantShilpa Singh MohanNo ratings yet
- Evoked PotentialsDocument49 pagesEvoked PotentialsparuNo ratings yet
- DYSPHAGIA Lecture NotesDocument84 pagesDYSPHAGIA Lecture Notesmcmak357No ratings yet
- Cochlear Implant Electrode ArraysDocument10 pagesCochlear Implant Electrode ArraysCitra LyadhaNo ratings yet
- An Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisDocument6 pagesAn Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisSaranya N MuthuNo ratings yet
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocument84 pagesTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimNo ratings yet
- Vertigo Physiology and Clinical AssessmentDocument63 pagesVertigo Physiology and Clinical Assessmentdraseemmishra100% (1)
- Cochlear ImplantationDocument81 pagesCochlear ImplantationHerlangga Fadhillah AkbarNo ratings yet
- Stenger Test GuideDocument2 pagesStenger Test GuideAnonymous iftX7wVPCNo ratings yet
- Auditory Neuropathy MorletDocument20 pagesAuditory Neuropathy MorletOxanaBitcaNo ratings yet
- Dysphagia Diagnosis 1and Treatment (Olle Ekberg) (Z-Lib - Org) (1) - 83-284Document202 pagesDysphagia Diagnosis 1and Treatment (Olle Ekberg) (Z-Lib - Org) (1) - 83-284Macarena Paz ÁlvarezNo ratings yet
- Speech AudiometryDocument9 pagesSpeech AudiometryVarunSharmaNo ratings yet
- Speech AudiometryDocument17 pagesSpeech AudiometryPero Kvržica100% (1)
- Cholesteatoma FinalDocument56 pagesCholesteatoma FinalDr.Bharathi M.BNo ratings yet
- Auditory Brain Stem ImplantsDocument7 pagesAuditory Brain Stem Implantsabirajalakshmix9395No ratings yet
- Flaccid DysarthriaDocument40 pagesFlaccid Dysarthriaaleeza nomanNo ratings yet
- Genetics of Hearing Loss DR NayyarDocument56 pagesGenetics of Hearing Loss DR NayyarSuprit SnNo ratings yet
- Lower Motor Neuron (LMN) Facial Palsy: Department of ENTDocument32 pagesLower Motor Neuron (LMN) Facial Palsy: Department of ENTalfaz lakhani100% (1)
- 2020 - ENT Unit Complete System (Online)Document9 pages2020 - ENT Unit Complete System (Online)Meloudie ValenciaNo ratings yet
- Therapeutic Management of Laryngectomy - PDF / KUNNAMPALLIL GEJO JOHNDocument31 pagesTherapeutic Management of Laryngectomy - PDF / KUNNAMPALLIL GEJO JOHNKUNNAMPALLIL GEJO JOHNNo ratings yet
- Management of Congenital Aural AtresiaDocument22 pagesManagement of Congenital Aural AtresiamelaniNo ratings yet
- Short Increment Sensitivity Index Test (SISI)Document2 pagesShort Increment Sensitivity Index Test (SISI)Anish RajNo ratings yet
- Early Identification and Management of HiDocument32 pagesEarly Identification and Management of Hisruthi sureshNo ratings yet
- Non Organic Hearing LossDocument59 pagesNon Organic Hearing LossAakritiNo ratings yet
- AnatoFisio VestibularDocument17 pagesAnatoFisio VestibularRocío YáñezNo ratings yet
- AIIMS PG Result 2017 Rank WiseDocument47 pagesAIIMS PG Result 2017 Rank WiseVikashKumar100% (1)
- A Double-Blind Randomized Controlled Trial of Normal Saline, Lactated Ringer's, and Hypertonic Saline Nasal Irrigation Solution After Endoscopic Sinus SurgeryDocument7 pagesA Double-Blind Randomized Controlled Trial of Normal Saline, Lactated Ringer's, and Hypertonic Saline Nasal Irrigation Solution After Endoscopic Sinus SurgeryYasdika ImamNo ratings yet
- Bedside Water Swallow Test ArticleDocument4 pagesBedside Water Swallow Test ArticleJU WSDNo ratings yet
- Visual Reinforcement Audiometry 1Document27 pagesVisual Reinforcement Audiometry 1Goesti Yudistira100% (1)
- pp2 Submission FormatDocument4 pagespp2 Submission Formatapi-314413672No ratings yet
- Eustachian Tube Dysfunction Consensus Statement On DefinitionDocument5 pagesEustachian Tube Dysfunction Consensus Statement On DefinitionMarília Barbieri PereiraNo ratings yet
- Cochlear Rotation and Its RelevanceDocument7 pagesCochlear Rotation and Its RelevanceDrTarek Mahmoud Abo KammerNo ratings yet
- Symptomatology and Examination of The Larynx and TracheaDocument42 pagesSymptomatology and Examination of The Larynx and TracheaYibeltalNo ratings yet
- Trans SaVi Oto Lec 03 Diseases of The External and Middle EarDocument13 pagesTrans SaVi Oto Lec 03 Diseases of The External and Middle EarJoherNo ratings yet
- Pfeiffer SyndromeDocument3 pagesPfeiffer SyndromeIfanRomliNo ratings yet
- Voicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffDocument13 pagesVoicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffFernanda MerichesNo ratings yet
- Assr, Vemp, VNG, OaeDocument8 pagesAssr, Vemp, VNG, OaeSuprit Sn100% (1)
- New Born Hearing FactsDocument8 pagesNew Born Hearing FactsAhiawortor Kplorla100% (1)
- CASE REPORT (Nasal Fracture) - Karina Sylvana - EnglishDocument23 pagesCASE REPORT (Nasal Fracture) - Karina Sylvana - EnglishJennifer GabriellaNo ratings yet
- Malignant Otitis Externa 20070821Document0 pagesMalignant Otitis Externa 20070821Suci PramadianiNo ratings yet
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDocument9 pagesAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiNo ratings yet
- Spinal Tumors - A Brief OverviewDocument38 pagesSpinal Tumors - A Brief OverviewRAVIRAJ GHORPADE BELGAUM ADVANCED NEUROSURGERYNo ratings yet
- Untitled 1Document17 pagesUntitled 1Tiberiu CttNo ratings yet
- Quick Review - Fossa of RosenmullerDocument4 pagesQuick Review - Fossa of RosenmullerDavis KallanNo ratings yet
- Acoustic - Stapedius - Reflexes PDFDocument6 pagesAcoustic - Stapedius - Reflexes PDFSOFTMERCURYNo ratings yet
- Rano - JR - SSHLDocument29 pagesRano - JR - SSHLArief FakhrizalNo ratings yet
- Journal ReadingDocument45 pagesJournal ReadingArief FakhrizalNo ratings yet
- Laryngitis: Wahyu Priatmoko 1301 1207 0197 Ilman Fathony 1301 1207 007Document74 pagesLaryngitis: Wahyu Priatmoko 1301 1207 0197 Ilman Fathony 1301 1207 007Arief FakhrizalNo ratings yet
- Skin Prick Test & Modified Quantitative TestDocument27 pagesSkin Prick Test & Modified Quantitative TestArief FakhrizalNo ratings yet
- Atelectasis 2Document12 pagesAtelectasis 2Arief FakhrizalNo ratings yet
- Atelectasis 1Document17 pagesAtelectasis 1Arief FakhrizalNo ratings yet
- Nitric Oxide and OSA FixDocument45 pagesNitric Oxide and OSA FixArief FakhrizalNo ratings yet
- The Preoperative Sinus CT: Avoiding A "Close" Call With Surgical ComplicationDocument28 pagesThe Preoperative Sinus CT: Avoiding A "Close" Call With Surgical ComplicationArief FakhrizalNo ratings yet
- NSR 7 3 22 Corpal KoinDocument10 pagesNSR 7 3 22 Corpal KoinArief FakhrizalNo ratings yet
- Tugas AntonDocument10 pagesTugas AntonArief FakhrizalNo ratings yet
- WD LaryngitisDocument80 pagesWD LaryngitisArief FakhrizalNo ratings yet
- NSR Abses 2 Okt 21Document23 pagesNSR Abses 2 Okt 21Arief FakhrizalNo ratings yet
- Piter - LR - Pure Tone Audiometry and MaskingDocument44 pagesPiter - LR - Pure Tone Audiometry and MaskingArief FakhrizalNo ratings yet
- Pediatric - Hearing - Loss Lau 3-17-10Document45 pagesPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNo ratings yet
- Laryngitis: Yanti NurrokhmawatiDocument73 pagesLaryngitis: Yanti NurrokhmawatiArief FakhrizalNo ratings yet
- Obstructive Sleep Apnea: Arief Fakhrizal Supervisor: Dr. Dr. Sinta Sari Ratunanda, M. Kes., Sp. T.H.T.K.L. (K)Document61 pagesObstructive Sleep Apnea: Arief Fakhrizal Supervisor: Dr. Dr. Sinta Sari Ratunanda, M. Kes., Sp. T.H.T.K.L. (K)Arief FakhrizalNo ratings yet
- LR QOL Qusstionnaire THTKOM WD (Autosaved)Document25 pagesLR QOL Qusstionnaire THTKOM WD (Autosaved)Arief FakhrizalNo ratings yet
- Piter - LR - Peripheral Balance Examination1Document29 pagesPiter - LR - Peripheral Balance Examination1Arief FakhrizalNo ratings yet
- Keamanan Dan Toksisitas Cempedak.Document13 pagesKeamanan Dan Toksisitas Cempedak.Arief FakhrizalNo ratings yet
- Bone and Soft Tissue HealingDocument28 pagesBone and Soft Tissue HealingArief FakhrizalNo ratings yet
- Sejarah Dan Perkembangan Ilmu Bedah September 2017Document18 pagesSejarah Dan Perkembangan Ilmu Bedah September 2017Arief Fakhrizal100% (1)
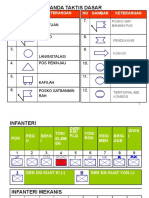
- Tanda Taktis Dasar: 1. Kesatuan 2. Posko 7Document8 pagesTanda Taktis Dasar: 1. Kesatuan 2. Posko 7Arief FakhrizalNo ratings yet
- Original PDF Introduction To Audiology 13th by Frederick N Martin PDFDocument41 pagesOriginal PDF Introduction To Audiology 13th by Frederick N Martin PDFthomas.young516100% (40)
- 2019 Audio Mixing Console Price List-LAIKESI - 副本Document12 pages2019 Audio Mixing Console Price List-LAIKESI - 副本FELIXJAVIERMNo ratings yet
- Third Window Lesions of The Inner Ear Quinton Gopen 9-30-09Document163 pagesThird Window Lesions of The Inner Ear Quinton Gopen 9-30-09Mahmoud Az MostafaNo ratings yet
- L.O ElectronicsDocument8 pagesL.O ElectronicsWagner Quezada IparraguirreNo ratings yet
- Auditory Pathways: Anatomy and Physiology: Handbook of Clinical Neurology March 2015Document24 pagesAuditory Pathways: Anatomy and Physiology: Handbook of Clinical Neurology March 2015florensiaNo ratings yet
- Anatomy and Physiology With PhatophysiologyDocument8 pagesAnatomy and Physiology With PhatophysiologyJustine Mae OyongNo ratings yet
- Hearing Loss in Older AdultsDocument7 pagesHearing Loss in Older AdultsDwiki GumelarNo ratings yet
- Pzab 177Document10 pagesPzab 177LORENZO GABRIEL BANAYONo ratings yet
- 6 - The 4 Ways To Use An EQ PDFDocument1 page6 - The 4 Ways To Use An EQ PDFRohit100% (1)
- Ear Disorder Multiple Choice Questions-RationaleDocument5 pagesEar Disorder Multiple Choice Questions-Rationalemydewyboy83% (6)
- Stuttering and Auditory Functions..pdf/ KUNNAMPALLIL GEJODocument90 pagesStuttering and Auditory Functions..pdf/ KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNNo ratings yet
- A Study of The Causes of The Reading Difficulties of Thirty ChildDocument184 pagesA Study of The Causes of The Reading Difficulties of Thirty Childleizle uretaNo ratings yet
- Soundcraft Efx12 Efx8 MixerDocument20 pagesSoundcraft Efx12 Efx8 MixerDelos Santos Jojo100% (1)
- Hearing Recovery From Deafness Caused by Bromate IntoxicationDocument3 pagesHearing Recovery From Deafness Caused by Bromate IntoxicationFefita lamNo ratings yet
- Neonatal and Infancy PeriodDocument42 pagesNeonatal and Infancy PeriodOhoud ElsheikhNo ratings yet
- ICSE Biology Notes Nervous System For 20 PDFDocument25 pagesICSE Biology Notes Nervous System For 20 PDFMmt RdcNo ratings yet
- Anaphy - SensesDocument4 pagesAnaphy - SensesAthena LeeNo ratings yet
- Anatomy / Physio of The EarDocument58 pagesAnatomy / Physio of The EarRA100% (1)
- Audio TechDocument3 pagesAudio TechAlexNo ratings yet
- Chapter 2 Human Factors & Pilot PerformanceDocument81 pagesChapter 2 Human Factors & Pilot PerformanceShoaib BarreNo ratings yet
- AAASteele BioDocument21 pagesAAASteele Bioceice2013100% (1)
- Daftar PustakaDocument2 pagesDaftar PustakaRia Rizki JayantiNo ratings yet
- TitanDocument12 pagesTitanAnthonyNo ratings yet
- The Microwave Auditory EffectDocument13 pagesThe Microwave Auditory EffectBrian BivinsNo ratings yet
- The EQ and Compression Formula - Learn The Step by Step Way To Use EQ and Compression Together (Aud - Ion, Sound Design & Mixing Audio Series - Book 1) - Nodrm PDFDocument44 pagesThe EQ and Compression Formula - Learn The Step by Step Way To Use EQ and Compression Together (Aud - Ion, Sound Design & Mixing Audio Series - Book 1) - Nodrm PDFGandhi Wasuvitchayagit100% (2)
- Alternate Loudness Balance TestDocument4 pagesAlternate Loudness Balance TestAnish RajNo ratings yet