Download as pptx, pdf, or txt
You might also like
- Truss Analysis and Shear Centre Lab ReportDocument33 pagesTruss Analysis and Shear Centre Lab ReportHamoodNo ratings yet
- Estacio Vs EstacioDocument14 pagesEstacio Vs EstacioWilfredo100% (2)
- PSY 441 Global Psychology PrePost Test National UniversityDocument7 pagesPSY 441 Global Psychology PrePost Test National UniversityTammy Smith67% (3)
- Nuero and Musculo Set B Answer KeyDocument15 pagesNuero and Musculo Set B Answer KeyChristopher SarsozaNo ratings yet
- Hypokalemia PDFDocument1 pageHypokalemia PDFJanedear PasalNo ratings yet
- Lesson Plan in Mathematics 7Document6 pagesLesson Plan in Mathematics 7Pomendia PaulrolandNo ratings yet
- TAMU EssaysDocument7 pagesTAMU EssaysAnakin Skywalker100% (2)
- Day 1 - Well Bore PositioningV2Document64 pagesDay 1 - Well Bore PositioningV2wwwNo ratings yet
- Diabetic Ketoacidosis Case StudyDocument5 pagesDiabetic Ketoacidosis Case StudyJully GaciasNo ratings yet
- Foreign Body Airway ObstructionDocument4 pagesForeign Body Airway ObstructionYanuar AdityaNo ratings yet
- Foreign Body Airway ObstructionDocument15 pagesForeign Body Airway ObstructionKristine Anne SorianoNo ratings yet
- Pathophysiology of Shock Sepsis and Organ Failure PDFDocument1,179 pagesPathophysiology of Shock Sepsis and Organ Failure PDFNotInterested100% (1)
- Acute Upper Airway ObstructionDocument2 pagesAcute Upper Airway ObstructionBudy CaecarianNo ratings yet
- Competency Appraisal 1Document30 pagesCompetency Appraisal 1mirai desuNo ratings yet
- NCM 118 Medsurg EndtermDocument25 pagesNCM 118 Medsurg EndtermJmarie Brillantes PopiocoNo ratings yet
- Acute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDDocument76 pagesAcute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDSamapriya Pasan Hewawasam100% (2)
- NCM 111 Nursing Research Reviewer PrelimsDocument8 pagesNCM 111 Nursing Research Reviewer PrelimsKIRSTEN CHAVEZNo ratings yet
- Nursing Care of Clients in Emergency Situation 2Document108 pagesNursing Care of Clients in Emergency Situation 2Mary Joy FrancoNo ratings yet
- Risk For Bleeding - Cirrhosis NCPDocument2 pagesRisk For Bleeding - Cirrhosis NCPPaula AbadNo ratings yet
- UTI (Urinary Tract Infection)Document9 pagesUTI (Urinary Tract Infection)Carson BirthNo ratings yet
- Submitted By: Bsn-Iv A Submitted To: Clinical Instructor: Cabatbat, Wyen CDocument5 pagesSubmitted By: Bsn-Iv A Submitted To: Clinical Instructor: Cabatbat, Wyen CWyen CabatbatNo ratings yet
- Medical-Surgical Nursing 3Document2 pagesMedical-Surgical Nursing 3Charissa Magistrado De LeonNo ratings yet
- Drugs Used To Treat Diabetes - MellitusDocument37 pagesDrugs Used To Treat Diabetes - MellitusjisooNo ratings yet
- Integrated Management of Childhood Illness (IMCI) : Guide For Clinical PracticeDocument79 pagesIntegrated Management of Childhood Illness (IMCI) : Guide For Clinical PracticeCAREZAMBIA100% (1)
- Prof. AdjustmentDocument111 pagesProf. AdjustmentDianne Kate CadioganNo ratings yet
- COPARDocument5 pagesCOPAREdezer CariasNo ratings yet
- NCM 100 Case AnaDocument3 pagesNCM 100 Case AnaCharissa Magistrado De LeonNo ratings yet
- Example of A Healthy Meal Plan For A 45 Year Old ManDocument12 pagesExample of A Healthy Meal Plan For A 45 Year Old ManzyloexNo ratings yet
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaNo ratings yet
- Case Study 1 PediaDocument7 pagesCase Study 1 PediaXeyanNo ratings yet
- Hematologic ManagementDocument17 pagesHematologic ManagementAlyssa MontimorNo ratings yet
- Insulin EffectsDocument24 pagesInsulin Effectsvag taoNo ratings yet
- Hirschprungs DiseaseDocument26 pagesHirschprungs DiseaseAndrian PramanaNo ratings yet
- Case Study 34 Closed Head InjuryDocument11 pagesCase Study 34 Closed Head Injuryapi-262963527No ratings yet
- Choking: by Jawad AhmedDocument25 pagesChoking: by Jawad Ahmedjawad_ahmedNo ratings yet
- Different Types of TriageDocument28 pagesDifferent Types of Triageanda3003No ratings yet
- VerA Ok-Prelim Ncm104 (Autosaved) VeraDocument30 pagesVerA Ok-Prelim Ncm104 (Autosaved) Verajesperdomincilbayaua100% (1)
- Multiple Choice Test QuestionsDocument6 pagesMultiple Choice Test QuestionsNicole MaeNo ratings yet
- Cardiovascular HealthDocument20 pagesCardiovascular HealthChrrieNo ratings yet
- Hepatocellula R CarcinomaDocument45 pagesHepatocellula R Carcinomamhean azneitaNo ratings yet
- CaseDocument7 pagesCaseAia JavierNo ratings yet
- Sample QuestionGITDocument3 pagesSample QuestionGITAli Zezo100% (1)
- Pleural Fluid Analysis: How The Test Is PerformedDocument4 pagesPleural Fluid Analysis: How The Test Is PerformedKevin LlorenteNo ratings yet
- Pulmonary Contusion - WikipediaDocument15 pagesPulmonary Contusion - WikipediaRony OktarizalNo ratings yet
- Case Presentation: Patient Chart - Mary JohnsonDocument12 pagesCase Presentation: Patient Chart - Mary Johnsonivoneeh_16100% (1)
- Postmortem Care: Rigor MortisDocument2 pagesPostmortem Care: Rigor Mortisqwerty24No ratings yet
- Nursing Management Pancreatic CancerDocument2 pagesNursing Management Pancreatic CancerKit NameKo100% (2)
- GI Diagnostic TestsDocument7 pagesGI Diagnostic TestspatzieNo ratings yet
- Volume ImpairmentDocument32 pagesVolume ImpairmentAcohCChaoNo ratings yet
- Gordons TypologyDocument37 pagesGordons TypologyJo PigarNo ratings yet
- Cholelithiasis NCP FINALDocument6 pagesCholelithiasis NCP FINALShreshthi VermaNo ratings yet
- Geriatric OPD and Grand Rounds JournalDocument2 pagesGeriatric OPD and Grand Rounds JournalOrlea Francisco-SisioNo ratings yet
- Colonic Carcinoma Case StudyDocument23 pagesColonic Carcinoma Case StudyGlaiza Claire Am-amlan OlayanNo ratings yet
- G3 IAH and ACSDocument29 pagesG3 IAH and ACSRoshin Mae E. TejeroNo ratings yet
- Philippine Nursing Law of 2002 Ra # 9173Document15 pagesPhilippine Nursing Law of 2002 Ra # 9173Michael Maunda AmpuanNo ratings yet
- Anecdotal ReportDocument12 pagesAnecdotal ReportNikko PayawalNo ratings yet
- Course Description: 3. Communities (Community Service)Document35 pagesCourse Description: 3. Communities (Community Service)April Mae Magos LabradorNo ratings yet
- RENAP 2009 Training SchedulesDocument3 pagesRENAP 2009 Training SchedulesNoel100% (4)
- FrostbiteDocument19 pagesFrostbiteKhadim Hussain Shah100% (1)
- Nursing Care of Clients With Ventilation DisordersDocument6 pagesNursing Care of Clients With Ventilation DisordersLuna MarieNo ratings yet
- Neurological Disorders Key NotesDocument31 pagesNeurological Disorders Key NotesHannah aswiniNo ratings yet
- Cushing's SyndromeDocument5 pagesCushing's SyndromesummerduskNo ratings yet
- What Is Hypertensive NephropathyDocument11 pagesWhat Is Hypertensive NephropathyIvy Pamanian DeldaNo ratings yet
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- Healthcare Reflections, Insights, and Lessons: Proactive/ReactiveFrom EverandHealthcare Reflections, Insights, and Lessons: Proactive/ReactiveNo ratings yet
- ICP Head InjuryDocument57 pagesICP Head InjuryWengel RedkissNo ratings yet
- Xi. Pathophysiology Benign Tumors of The UterusDocument1 pageXi. Pathophysiology Benign Tumors of The UterusWengel RedkissNo ratings yet
- Pulmonary FailureDocument29 pagesPulmonary FailureWengel RedkissNo ratings yet
- 6 Problem List NCP Progress NotesDocument14 pages6 Problem List NCP Progress NotesWengel RedkissNo ratings yet
- Laboratory and Diagnostic ResultsDocument1 pageLaboratory and Diagnostic ResultsWengel RedkissNo ratings yet
- Xi. Pathophysiology Benign Tumors of The UterusDocument1 pageXi. Pathophysiology Benign Tumors of The UterusWengel RedkissNo ratings yet
- 7 Progress NotesDocument1 page7 Progress NotesWengel RedkissNo ratings yet
- Ultrasound AUBDocument1 pageUltrasound AUBWengel RedkissNo ratings yet
- 7 Progress NotesDocument1 page7 Progress NotesWengel RedkissNo ratings yet
- White Blood CellDocument3 pagesWhite Blood CellWengel RedkissNo ratings yet
- Ultrasound AUBDocument1 pageUltrasound AUBWengel RedkissNo ratings yet
- Perioperative Nursing: Kennedy C. Bangan, RN, MSN, HAAD-RNDocument81 pagesPerioperative Nursing: Kennedy C. Bangan, RN, MSN, HAAD-RNWengel RedkissNo ratings yet
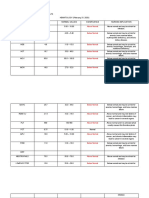
- Xii. Laboratory and Diagnostic Results HEMATOLOGY (February 21, 2020) CBC Result Normal Values Significance Nursing ImplicationDocument7 pagesXii. Laboratory and Diagnostic Results HEMATOLOGY (February 21, 2020) CBC Result Normal Values Significance Nursing ImplicationWengel RedkissNo ratings yet
- Breastfeeding FinalDocument25 pagesBreastfeeding FinalWengel RedkissNo ratings yet
- Content and Contextual Analysis of The Parisian LifeDocument7 pagesContent and Contextual Analysis of The Parisian LifeSowla sidoNo ratings yet
- Unit IV. Communication in Pharmacy Practice PDFDocument54 pagesUnit IV. Communication in Pharmacy Practice PDFGeannea Mae LeañoNo ratings yet
- Docslide - Us - Siae Alfo Plus User Manual PDFDocument110 pagesDocslide - Us - Siae Alfo Plus User Manual PDFh2ck3rNo ratings yet
- Sample Term PaperDocument15 pagesSample Term Paperalchwarizmi abubakarNo ratings yet
- Design and Analysis of AlgorithmsDocument200 pagesDesign and Analysis of AlgorithmsChitra RNo ratings yet
- Winton Oil Color ChartDocument1 pageWinton Oil Color ChartfreshjuiceNo ratings yet
- Who Coined The Term "PHILOSOPHY"? A) PythagorasDocument42 pagesWho Coined The Term "PHILOSOPHY"? A) PythagorasMosalas CompanyNo ratings yet
- 1 s2.0 S0888327017305654 MainDocument10 pages1 s2.0 S0888327017305654 MainchinnavenkateswarluNo ratings yet
- Software Manual Ifm 7391009UKDocument19 pagesSoftware Manual Ifm 7391009UKpatriciobenavidesmNo ratings yet
- Kvs Split Up of Syllabus Class I & IIDocument9 pagesKvs Split Up of Syllabus Class I & IISanjeev MachalNo ratings yet
- Leadership Styles For 5 StagesDocument18 pagesLeadership Styles For 5 Stagesbimal.greenroadNo ratings yet
- SNAKE PLANT (Sansevieria Trifasciata) FIBER AS A POTENTIAL SOURCE OF PAPERDocument38 pagesSNAKE PLANT (Sansevieria Trifasciata) FIBER AS A POTENTIAL SOURCE OF PAPERandrei100% (1)
- Project Management Plan Template ProcessDocument7 pagesProject Management Plan Template ProcessShanekia Lawson-WellsNo ratings yet
- Final Project ThermalDocument21 pagesFinal Project ThermalArizap MoltresNo ratings yet
- Pag254 Grammar and Vocabulary For Cambridge Advanced and Proficiency - LongmanDocument1 pagePag254 Grammar and Vocabulary For Cambridge Advanced and Proficiency - LongmandanielitoNo ratings yet
- Jackson's Deceptive Lottery. A Literary AnalysisDocument2 pagesJackson's Deceptive Lottery. A Literary Analysisapi-314072190No ratings yet
- Circular 20210129214120 Vi-FinalDocument4 pagesCircular 20210129214120 Vi-FinalAmandeep SinghNo ratings yet
- Assignment 1Document3 pagesAssignment 1Hafez MohammedNo ratings yet
- The Walkthrough Method:an Approach To The Study OfappsDocument27 pagesThe Walkthrough Method:an Approach To The Study Ofappstan nguyenNo ratings yet
- tóm tắt sách atomic habitDocument3 pagestóm tắt sách atomic habitPeter SmithNo ratings yet
- Small Round Cell TumorsDocument131 pagesSmall Round Cell TumorschinnnababuNo ratings yet
- O'Reilly - Managing Ip Networks With Cisco RoutersDocument366 pagesO'Reilly - Managing Ip Networks With Cisco RoutersJavier ColucciNo ratings yet
- Unit 8 Lesson 1: Parts of The BodyDocument2 pagesUnit 8 Lesson 1: Parts of The BodyNguyễn PhúcNo ratings yet
- Astro GramaDocument4 pagesAstro GramageorgemihailNo ratings yet