Download as ppt, pdf, or txt
You might also like
- Full Ebook of Foundations of Behavioral Neuroscience 10Th Edition Neil Carlson Online PDF All ChapterDocument69 pagesFull Ebook of Foundations of Behavioral Neuroscience 10Th Edition Neil Carlson Online PDF All Chapterjohngross404580100% (8)
- Handout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisDocument2 pagesHandout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisValentina IerotheouNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Anamnesis & PemfisDocument81 pagesAnamnesis & PemfisFikriYTNo ratings yet
- Cardiac AsthmaDocument12 pagesCardiac AsthmaNeupane KsabNo ratings yet
- Arrhythmias and Conduction DisordersDocument23 pagesArrhythmias and Conduction Disordersxaalam easyNo ratings yet
- Feedback Systems in The BodyDocument13 pagesFeedback Systems in The Bodymrmr92No ratings yet
- ShockDocument63 pagesShockAhmedNo ratings yet
- Standard Treatment Protocol of Emergency Health Service PackageDocument279 pagesStandard Treatment Protocol of Emergency Health Service Packagekapil khanalNo ratings yet
- PEEP (Positive-End Expiratory Pressure)Document5 pagesPEEP (Positive-End Expiratory Pressure)Valcrist BalderNo ratings yet
- PICU Common ProblemDocument49 pagesPICU Common ProblemRawabi rawabi1997No ratings yet
- 8.the Atls ProtocolDocument57 pages8.the Atls ProtocolReuben DutiNo ratings yet
- Advanced Life Support EMS ScenariosDocument147 pagesAdvanced Life Support EMS Scenariosfidelurtecho4881No ratings yet
- 1.congenital Heart DiseaseDocument60 pages1.congenital Heart Diseasemerzi farooq ahmadkhanNo ratings yet
- Myocardial ProtectionDocument36 pagesMyocardial ProtectionRheecha JoshiNo ratings yet
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocument15 pagesPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNo ratings yet
- Insulin and Oral Hypoglycemic AgentsDocument27 pagesInsulin and Oral Hypoglycemic Agentsapi-19916399100% (1)
- Pulmonary HypertensionDocument26 pagesPulmonary Hypertensionakoeljames8543No ratings yet
- Cardiovascular Pathology 1:: Blood VesselsDocument48 pagesCardiovascular Pathology 1:: Blood VesselsRaiver CadenNo ratings yet
- Cad ....Document94 pagesCad ....AnanthibalaNo ratings yet
- Lung Sounds: An Assessment of The Patient in Respiratory DistressDocument40 pagesLung Sounds: An Assessment of The Patient in Respiratory DistressJoseph Rodney de LeonNo ratings yet
- Cor PulmonaleDocument8 pagesCor PulmonaleAymen OmerNo ratings yet
- Oxygen SupplementationDocument15 pagesOxygen SupplementationEloisa BretañaNo ratings yet
- Surgical Implications of Low Cardiac Output Syndrome After Myocardial InfarctionDocument5 pagesSurgical Implications of Low Cardiac Output Syndrome After Myocardial Infarctionrandomized1234No ratings yet
- Antiarrythmic Drugs: Dr.V.Krishnan MD C.DiabDocument28 pagesAntiarrythmic Drugs: Dr.V.Krishnan MD C.Diabdevita oktaviani salsabilla kiranaNo ratings yet
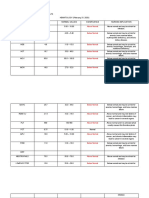
- Antiarrhythmic Drugs - Classification and Mechanism of Action.Document1 pageAntiarrhythmic Drugs - Classification and Mechanism of Action.SUMIT KUMAR DASNo ratings yet
- Auto PEEPDocument16 pagesAuto PEEPVishwajith Murthy100% (1)
- ATLSDocument92 pagesATLSRendi MuflihNo ratings yet
- Patofisiologi AritmiaDocument27 pagesPatofisiologi AritmiaVedora Angelia GultomNo ratings yet
- Drug Class Mechanism of Action Example: ThiazideDocument2 pagesDrug Class Mechanism of Action Example: ThiazideLyod BalagasayNo ratings yet
- Kyphoscoliosis 2018 ARCDocument36 pagesKyphoscoliosis 2018 ARCLOK rNo ratings yet
- Pulmonary HypertensionDocument43 pagesPulmonary Hypertensiong1381821No ratings yet
- Beta BlockerDocument8 pagesBeta BlockerZiedTriki100% (1)
- Difficult Weaning From Cardiopulmonary Bypass Final Edit LiaDocument41 pagesDifficult Weaning From Cardiopulmonary Bypass Final Edit LiaYuri SadewoNo ratings yet
- KegawatdaruratanDocument164 pagesKegawatdaruratanmeida astriani gozaziNo ratings yet
- Cardiac Action PotentialDocument41 pagesCardiac Action PotentialRadijska Postaja KoprivnicaNo ratings yet
- Intravenous Fluid Therapy For 2nd Year ConceptDocument83 pagesIntravenous Fluid Therapy For 2nd Year ConceptMay Chelle ErazoNo ratings yet
- Posterior Cranial Fossa Anesthetic ManagementDocument48 pagesPosterior Cranial Fossa Anesthetic ManagementDivya Rekha KolliNo ratings yet
- Cardiopulmonary Bypass: Dr. Ravi Gadani MS, FmasDocument24 pagesCardiopulmonary Bypass: Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- Ischemic Heart DiseaseDocument116 pagesIschemic Heart DiseaseAndrew OrlovNo ratings yet
- A Clinical Approach To SyncopeDocument8 pagesA Clinical Approach To Syncopepuskesmas tarik100% (1)
- Respiratory Failure: Barry WardleDocument28 pagesRespiratory Failure: Barry Wardleapi-19826220No ratings yet
- Perioperative AnaphylaxisDocument23 pagesPerioperative AnaphylaxiscrackernetNo ratings yet
- CardiologyDocument62 pagesCardiologysee yinNo ratings yet
- Pericardial EffusionDocument3 pagesPericardial EffusionNita Hurek100% (1)
- "Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareDocument51 pages"Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareSohil ElfarNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- Ent Emergencies Epistaxis (Nose Bleed)Document4 pagesEnt Emergencies Epistaxis (Nose Bleed)Penny_Teoh_3451No ratings yet
- Abdominal IncisionDocument4 pagesAbdominal IncisionMohit KumarNo ratings yet
- Intravenous FluidsDocument19 pagesIntravenous Fluidsblack pink in ur area 21100% (1)
- Terminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke ManagementDocument28 pagesTerminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke Managementbusiness911No ratings yet
- Electrolyte AbnormalitiesDocument74 pagesElectrolyte Abnormalitiesbluecrush1No ratings yet
- Respiratory Failure PresentationDocument13 pagesRespiratory Failure PresentationHusnain Irshad AlviNo ratings yet
- Dka Vs Hhs Edit 1Document25 pagesDka Vs Hhs Edit 1Razeen RiyasatNo ratings yet
- Mechanical Ventilation and Intracranial PressureDocument30 pagesMechanical Ventilation and Intracranial PressureFlavius AnghelNo ratings yet
- Pulsus Paradoxus - Wikip PDFDocument4 pagesPulsus Paradoxus - Wikip PDFAniket MittalNo ratings yet
- Cardiac ArrestDocument54 pagesCardiac ArrestIdha FitriyaniNo ratings yet
- Anaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangDocument15 pagesAnaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangTeguh PambudiNo ratings yet
- SyncopeDocument4 pagesSyncopeLakshay Chanana100% (1)
- What Is Respiratory Alkalosis?Document3 pagesWhat Is Respiratory Alkalosis?Lorenn AdarnaNo ratings yet
- Pulmonary FailureDocument29 pagesPulmonary FailureWengel RedkissNo ratings yet
- Xi. Pathophysiology Benign Tumors of The UterusDocument1 pageXi. Pathophysiology Benign Tumors of The UterusWengel RedkissNo ratings yet
- Metabolic EmergenciesDocument53 pagesMetabolic EmergenciesWengel Redkiss100% (1)
- 6 Problem List NCP Progress NotesDocument14 pages6 Problem List NCP Progress NotesWengel RedkissNo ratings yet
- Laboratory and Diagnostic ResultsDocument1 pageLaboratory and Diagnostic ResultsWengel RedkissNo ratings yet
- Xi. Pathophysiology Benign Tumors of The UterusDocument1 pageXi. Pathophysiology Benign Tumors of The UterusWengel RedkissNo ratings yet
- 7 Progress NotesDocument1 page7 Progress NotesWengel RedkissNo ratings yet
- Ultrasound AUBDocument1 pageUltrasound AUBWengel RedkissNo ratings yet
- 7 Progress NotesDocument1 page7 Progress NotesWengel RedkissNo ratings yet
- White Blood CellDocument3 pagesWhite Blood CellWengel RedkissNo ratings yet
- Ultrasound AUBDocument1 pageUltrasound AUBWengel RedkissNo ratings yet
- Perioperative Nursing: Kennedy C. Bangan, RN, MSN, HAAD-RNDocument81 pagesPerioperative Nursing: Kennedy C. Bangan, RN, MSN, HAAD-RNWengel RedkissNo ratings yet
- Xii. Laboratory and Diagnostic Results HEMATOLOGY (February 21, 2020) CBC Result Normal Values Significance Nursing ImplicationDocument7 pagesXii. Laboratory and Diagnostic Results HEMATOLOGY (February 21, 2020) CBC Result Normal Values Significance Nursing ImplicationWengel RedkissNo ratings yet
- Breastfeeding FinalDocument25 pagesBreastfeeding FinalWengel RedkissNo ratings yet
- Attenuation of 3,4-Methylenedioxymethamphetamine (MDMA) Induced Neurotoxicity With The Serotonin Precursors Tryptophan and 5-HydroxytryptophanDocument6 pagesAttenuation of 3,4-Methylenedioxymethamphetamine (MDMA) Induced Neurotoxicity With The Serotonin Precursors Tryptophan and 5-HydroxytryptophanflaminglawyerNo ratings yet
- Somatosensory CortexDocument19 pagesSomatosensory Cortexusamabangash943No ratings yet
- DIV 15 Combat Mindset PDFDocument9 pagesDIV 15 Combat Mindset PDFNelson RamirezNo ratings yet
- Habit Interference: Athulya, Anu, Mahreen, Medhavi, Sandhya, Sanjana, Sunethra, VaishaliDocument17 pagesHabit Interference: Athulya, Anu, Mahreen, Medhavi, Sandhya, Sanjana, Sunethra, VaishaliSanjana Vijaynidhi 18PJW043100% (1)
- Assessment and Treatment of Movement Disorders in Children With Cerebral PalsyDocument11 pagesAssessment and Treatment of Movement Disorders in Children With Cerebral PalsyLizza Mora RNo ratings yet
- Sistem Pakar Diagnosa Mental Ilness Psikosis Dengan Menggunakan Metode Certainty FactorDocument5 pagesSistem Pakar Diagnosa Mental Ilness Psikosis Dengan Menggunakan Metode Certainty FactorRektorat UnbrahNo ratings yet
- Neuroleptic Malignant SyndromeDocument21 pagesNeuroleptic Malignant SyndromeAndreea BujorNo ratings yet
- Neurologic Complications of Critical Illness Contemporary Neurology Series Team Ira 4Th Edition Eelco F M Wijdicks Full ChapterDocument52 pagesNeurologic Complications of Critical Illness Contemporary Neurology Series Team Ira 4Th Edition Eelco F M Wijdicks Full Chaptermary.scriven487100% (9)
- Gait Abnormalities Assessment and CausesDocument12 pagesGait Abnormalities Assessment and CausesMudassar SattarNo ratings yet
- Cortical Vs Subcortical DementiaDocument3 pagesCortical Vs Subcortical DementiaCami Sánchez SalinasNo ratings yet
- Peripheral Neuropathy Clinical ApproachDocument19 pagesPeripheral Neuropathy Clinical ApproachNur Nadzifah Zainal AbidinNo ratings yet
- Os 1Document4 pagesOs 1rizwanNo ratings yet
- European Neuropsychopharmacology Volume 27 Issue 2017 (Doi 10.1016/s0924-977x (17) 31470-0) Pans Molina, I. Regli Rojas, E. Peralta Gallego, F.J. Piña B - Prevalence and Characteristics of PatDocument1 pageEuropean Neuropsychopharmacology Volume 27 Issue 2017 (Doi 10.1016/s0924-977x (17) 31470-0) Pans Molina, I. Regli Rojas, E. Peralta Gallego, F.J. Piña B - Prevalence and Characteristics of PatAlma AcevedoNo ratings yet
- Presentasi DR Baskoro Stroke Day Door To NeedleDocument30 pagesPresentasi DR Baskoro Stroke Day Door To NeedleagengNo ratings yet
- Psychopathology Madjirova PDFDocument400 pagesPsychopathology Madjirova PDFandrehpNo ratings yet
- Thesis For WeeblyDocument11 pagesThesis For Weeblyapi-608954316No ratings yet
- Organic Mental Disorders: Zoltán HidasiDocument30 pagesOrganic Mental Disorders: Zoltán HidasiEleoner RamirezNo ratings yet
- Copia de 1000 Preguntas de Autoevaluacion PDFDocument658 pagesCopia de 1000 Preguntas de Autoevaluacion PDFAnonymous FUrdgw75% (4)
- Language and The BrainDocument33 pagesLanguage and The BrainRaymond CayabyabNo ratings yet
- Merritt's NeurologyDocument2,929 pagesMerritt's Neurologys.oana90No ratings yet
- Print - Chapter 2. Neurohumoral Regulation of Gastrointestinal FunctionDocument19 pagesPrint - Chapter 2. Neurohumoral Regulation of Gastrointestinal FunctionbelaginaNo ratings yet
- Impaired Physical MobilityDocument1 pageImpaired Physical MobilitySheena Yen de Pano-PagdalianNo ratings yet
- Kjellin Practise Pronunciation W Audacity PDFDocument21 pagesKjellin Practise Pronunciation W Audacity PDFNamNo ratings yet
- Extract From Anatomy Course LectureDocument5 pagesExtract From Anatomy Course LectureMumuh Moe' MuhtadinNo ratings yet
- Solution Manual For Vanders Human Physiology 15th Edition Eric Widmaier and Hershel Raff and Kevin StrangDocument17 pagesSolution Manual For Vanders Human Physiology 15th Edition Eric Widmaier and Hershel Raff and Kevin StrangDanielKimqnob100% (38)
- Educ 3.0Document2 pagesEduc 3.0shanna paduaNo ratings yet
- Pavlov - Conditioned Reflexes An Investigation of The Physiological Activity of The Cerebral CortexDocument442 pagesPavlov - Conditioned Reflexes An Investigation of The Physiological Activity of The Cerebral CortexfrontroNo ratings yet
- Biological Basis of Human BehaviorDocument27 pagesBiological Basis of Human BehaviorAnanta ChaliseNo ratings yet