Download as pptx, pdf, or txt
You might also like
- Harrison MCQ NephrologyDocument7 pagesHarrison MCQ Nephrologydrtpk80% (15)
- 9 Base Pairing Worksheet PDFDocument4 pages9 Base Pairing Worksheet PDFWESLEY ARCONNo ratings yet
- Protein Metabolism Dental and Physiotherapy Part 1Document17 pagesProtein Metabolism Dental and Physiotherapy Part 1Nada Atef KoraitemNo ratings yet
- Chapter X - Mechanism of Protein MetabolismDocument30 pagesChapter X - Mechanism of Protein MetabolismAngelo AngelesNo ratings yet
- HyperammonemiaDocument10 pagesHyperammonemiaAsfoor gake1No ratings yet
- Wa0028.Document46 pagesWa0028.Ziyadan AtiqueNo ratings yet
- Physical Properties of ProteinsDocument46 pagesPhysical Properties of ProteinsTasneem AhmedNo ratings yet
- Inborn Errors of Protein MetabolismDocument48 pagesInborn Errors of Protein MetabolismChudasama DhruvrajsinhNo ratings yet
- Explain The Ff. Manifestations in The Different Cases That Are Discused BelowDocument29 pagesExplain The Ff. Manifestations in The Different Cases That Are Discused BelowRodel Paulo Tangunan GarciaNo ratings yet
- Urea Cycle and Disorders - RM - F2014Document18 pagesUrea Cycle and Disorders - RM - F2014Leon WarrenNo ratings yet
- Investigation of Amino Acids DisordersDocument4 pagesInvestigation of Amino Acids Disorderskiedd_04100% (1)
- Ammonia PDFDocument5 pagesAmmonia PDFiulia100% (1)
- Ammonia (Plasma, Blood) : 1 Name and Description of AnalyteDocument5 pagesAmmonia (Plasma, Blood) : 1 Name and Description of AnalyteiuliaNo ratings yet
- 4 Protein ReviewDocument87 pages4 Protein Reviewmika de guzmanNo ratings yet
- Neonatal HyperammonaemiaDocument12 pagesNeonatal HyperammonaemiaGawri AbeyNo ratings yet
- UAS KARBOHIDRAT 2-DikonversiDocument18 pagesUAS KARBOHIDRAT 2-DikonversiumayaNo ratings yet
- Lecture 5 Protein Metabolism 2 GD 3Document20 pagesLecture 5 Protein Metabolism 2 GD 3beneficialboxer9237No ratings yet
- Amino Acidss & AminoacidopathiesDocument55 pagesAmino Acidss & AminoacidopathiesMustafa KhandgawiNo ratings yet
- PCH 201 L 3Document14 pagesPCH 201 L 3KellyNo ratings yet
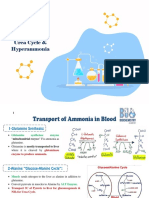
- Urea Cycle & HyperammoniaDocument6 pagesUrea Cycle & HyperammoniaSal TlsNo ratings yet
- Urea CycleDocument39 pagesUrea Cycledrismailkm20No ratings yet
- 1.15 Amino Acid MetabolismDocument16 pages1.15 Amino Acid MetabolismnkhomaslaterNo ratings yet
- Lecture 3 Urea Cycle DisordersDocument27 pagesLecture 3 Urea Cycle Disordersamjadm2002No ratings yet
- HYPERAMMONEMIADocument10 pagesHYPERAMMONEMIANaisha JNo ratings yet
- Proteins and Liver Function TestsDocument56 pagesProteins and Liver Function TestsjoanNo ratings yet
- Ammoniacal EncephalopathyDocument26 pagesAmmoniacal Encephalopathykhaled khalifaNo ratings yet
- Urea CycleDocument3 pagesUrea CycleSundaralingam RajNo ratings yet
- Urea Cycle and Protein MetabolismDocument39 pagesUrea Cycle and Protein Metabolismikramullahkhan211No ratings yet
- Inborn Error of MetabolismDocument27 pagesInborn Error of MetabolismNarayan GhimireNo ratings yet
- Inborn Errors of Urea SynthesisDocument14 pagesInborn Errors of Urea SynthesisDaryl Jacob Bigay100% (1)
- hyperammonemia^Jنور الهدى الهدى حسين الماسDocument7 pageshyperammonemia^Jنور الهدى الهدى حسين الماسMohammed MNo ratings yet
- Hyperammonemia: Department of BiochemistryDocument7 pagesHyperammonemia: Department of BiochemistryMohammed MNo ratings yet
- Hyperammonemia: Department of BiochemistryDocument7 pagesHyperammonemia: Department of BiochemistryMohammed MNo ratings yet
- Inborn Errors of Metabolism: Intensive Care Nursery House Staff ManualDocument5 pagesInborn Errors of Metabolism: Intensive Care Nursery House Staff ManualwarishNo ratings yet
- Ojemekele o Blood Chemistry Blood As A Tissue and PorphyrinsDocument47 pagesOjemekele o Blood Chemistry Blood As A Tissue and PorphyrinsAbdulateef AdebisiNo ratings yet
- Protein and Amino Acids: Metabolism and AnalysisDocument35 pagesProtein and Amino Acids: Metabolism and AnalysisWindi MoseNo ratings yet
- Enzymes: M. Zaharna Clin. Chem. 2009Document32 pagesEnzymes: M. Zaharna Clin. Chem. 2009Ahmed GaberNo ratings yet
- Planea Tu Viaje Guía Moderno Con Rectángulos Negros Con Fondo Blanco InfografíaDocument2 pagesPlanea Tu Viaje Guía Moderno Con Rectángulos Negros Con Fondo Blanco InfografíaDavid Cagua CuadrosNo ratings yet
- Aminacid MetabolismDocument84 pagesAminacid MetabolismAaronJose100% (1)
- Hyperammonemia in ReviewDocument16 pagesHyperammonemia in ReviewIka KusumaNo ratings yet
- Metabolisme Protein: Oleh: Gusliani Eka Putri, M.SiDocument65 pagesMetabolisme Protein: Oleh: Gusliani Eka Putri, M.Sipuskesmas patamuanNo ratings yet
- Uric PDFDocument28 pagesUric PDFNgân TrươngNo ratings yet
- Amino Acids: M. Zaharna Clin. Chem. 2009Document39 pagesAmino Acids: M. Zaharna Clin. Chem. 2009Ahmed GaberNo ratings yet
- Chemical Pathology BS-MLT 5Th SemesterDocument36 pagesChemical Pathology BS-MLT 5Th SemesterMuhammad AbdullahNo ratings yet
- 5692 - Lecture 2Document18 pages5692 - Lecture 2bloodstoragecentersuryaNo ratings yet
- Hypomagnesemia & HypermagnesemiaDocument18 pagesHypomagnesemia & HypermagnesemiaLanzen DragneelNo ratings yet
- MBBS II Ammonia MetabolismDocument25 pagesMBBS II Ammonia MetabolismamareaneneNo ratings yet
- Urea Cycle and Its DefectsDocument48 pagesUrea Cycle and Its DefectsStevia NdoeNo ratings yet
- Urine Screening For Metabolic DisordersDocument55 pagesUrine Screening For Metabolic DisordersGlormina Asprec AvenaNo ratings yet
- Lecture 5 - Synthesis of Non-Essential AADocument17 pagesLecture 5 - Synthesis of Non-Essential AAciyace7849No ratings yet
- Metabolic Disorder Obtain Plasma Ammonia High Normal Obtain Blood PH and C02 Obtain Blood PH and C02Document14 pagesMetabolic Disorder Obtain Plasma Ammonia High Normal Obtain Blood PH and C02 Obtain Blood PH and C02Grace LazarragaNo ratings yet
- M5 3 HypokalemiaDocument6 pagesM5 3 HypokalemiaVishal KumarNo ratings yet
- 6 BodyDocument110 pages6 Bodysinte beyuNo ratings yet
- 8 Endocrine Metabolic and Lipid Disorders - 2012 - Small Animal Clinical Diagnosis by Laboratory Methods Fifth EditionDocument35 pages8 Endocrine Metabolic and Lipid Disorders - 2012 - Small Animal Clinical Diagnosis by Laboratory Methods Fifth EditionNarvarte Hospital Veterinario de EspecialidadesNo ratings yet
- (Biochemistry) Onsite Assignment No8 - Group XDocument33 pages(Biochemistry) Onsite Assignment No8 - Group XV THNo ratings yet
- Aminoleban 8% Amino Acid: For Intravenous AdministrationDocument4 pagesAminoleban 8% Amino Acid: For Intravenous AdministrationDietisien MHKNNo ratings yet
- Biochemistry Final Key NotesDocument11 pagesBiochemistry Final Key NotesShirel YehezkelNo ratings yet
- Hyperammonemia: Fatin Salina Zainal Abidin BMD103011Document2 pagesHyperammonemia: Fatin Salina Zainal Abidin BMD103011Hanis Afiqah Violet MeowNo ratings yet
- Hypomagnesemia: Presented by Shreya JhaDocument44 pagesHypomagnesemia: Presented by Shreya JhaGregory LitangNo ratings yet
- Bacterial Growth CurveDocument3 pagesBacterial Growth CurveGampa Vijaykumar100% (1)
- 1 SurgeryDocument85 pages1 SurgeryKresnie Anne BautistaNo ratings yet
- CoenzymesDocument14 pagesCoenzymessmollorenaNo ratings yet
- Antioxidants in The Prevention of Cerebrovasculer Disease: SuryadiDocument11 pagesAntioxidants in The Prevention of Cerebrovasculer Disease: SuryadirarazkanthapamenangNo ratings yet
- Brothers: Integration of Metabolism and Metabolic Processes in Fed, Fasting and Starvation StatesDocument14 pagesBrothers: Integration of Metabolism and Metabolic Processes in Fed, Fasting and Starvation StatesNischal DhNo ratings yet
- Advanced BIochemistry PPT I SemDocument469 pagesAdvanced BIochemistry PPT I Semkratikaagrawal50No ratings yet
- Energy Expenditure at Rest and During ExerciseDocument10 pagesEnergy Expenditure at Rest and During ExerciseJulio JuarezNo ratings yet
- Biocorrosion: H.A. Videla and L.K. Herrera BDocument26 pagesBiocorrosion: H.A. Videla and L.K. Herrera Bcanmert kocaNo ratings yet
- Iso TemplateDocument5 pagesIso TemplateShiella Mae Baltazar BulauitanNo ratings yet
- (Derita, Marcos G. Rai, Mahendra Zacchino, Susan (B-Ok - Xyz) PDFDocument327 pages(Derita, Marcos G. Rai, Mahendra Zacchino, Susan (B-Ok - Xyz) PDFKima MadNo ratings yet
- Crystal - Res.ku - Edu Taksnotes Biol 638 Notes CHP 16Document19 pagesCrystal - Res.ku - Edu Taksnotes Biol 638 Notes CHP 16shahjafferNo ratings yet
- Quiz-4-Storage Mechanisms and Control in Carbohydrate MetabolismDocument5 pagesQuiz-4-Storage Mechanisms and Control in Carbohydrate Metabolismaichiii.bearNo ratings yet
- Nutrition in Plants - Mineral Nutrition: Module - 2Document13 pagesNutrition in Plants - Mineral Nutrition: Module - 2keerthyNo ratings yet
- Biologia Celular y Moleculas - TallerDocument2 pagesBiologia Celular y Moleculas - TallerJulieth Karina Mendoza AcostaNo ratings yet
- Metabolic Pathways in Higher Plants and Their Determination: Unit-IDocument8 pagesMetabolic Pathways in Higher Plants and Their Determination: Unit-ISarvan ManiNo ratings yet
- Job Options: B.Sc. (Food Science, Nutrition & Dietetics) - UonDocument10 pagesJob Options: B.Sc. (Food Science, Nutrition & Dietetics) - Uonpaul machariaNo ratings yet
- Chloroplast PanabangiDocument7 pagesChloroplast PanabangiPatrick Rómulo CabilingNo ratings yet
- Citrulline, Arginine and High Intensity Exercise PerformanceDocument2 pagesCitrulline, Arginine and High Intensity Exercise PerformanceLuis Castro XtrmNo ratings yet
- Bioprocess 1 SBT 2132Document13 pagesBioprocess 1 SBT 2132Biotechnology IIUM Kuantan100% (2)
- Photosynthesis in Higher PlantsDocument16 pagesPhotosynthesis in Higher PlantsMohammed ArifuddinNo ratings yet
- Ecosystem Life EnergyDocument34 pagesEcosystem Life EnergyKeith C CabbabNo ratings yet
- Ubiquinone Biosynthesis of QuinoneDocument12 pagesUbiquinone Biosynthesis of QuinoneFrancisco EspinosaNo ratings yet
- Fermentation: University of Diyala College of Engineering Department of Chemical EngineeringDocument13 pagesFermentation: University of Diyala College of Engineering Department of Chemical EngineeringEnegineer HusseinNo ratings yet
- Vitamins PowerpointDocument37 pagesVitamins Powerpointerika paduaNo ratings yet
- Urea Cycle Illustration AtfDocument1 pageUrea Cycle Illustration Atfkecixa7414No ratings yet
- Active Principle: Lecture 10 Pharm Sci/Chem 177, University of California, IrvineDocument52 pagesActive Principle: Lecture 10 Pharm Sci/Chem 177, University of California, IrvineVivian PhamNo ratings yet
- Medicines by Design: U.S. Department of Health and Human ServicesDocument60 pagesMedicines by Design: U.S. Department of Health and Human ServicesChandru SNo ratings yet
- Grapevine Nutrition AmendedDocument32 pagesGrapevine Nutrition AmendedDavid GluhićNo ratings yet
- Latihan Chap 7 f4Document3 pagesLatihan Chap 7 f4Faizal PejerNo ratings yet