Download as pptx, pdf, or txt
You might also like
- Masturbation Free EbookDocument5 pagesMasturbation Free EbookVishal Pandey75% (4)
- Steam Tracing With MS ExcelDocument14 pagesSteam Tracing With MS ExcelRaul Bautista100% (2)
- Squeezed by Alissa Quart "Why Our Families Can't Afford America"Document6 pagesSqueezed by Alissa Quart "Why Our Families Can't Afford America"Zahra AfikahNo ratings yet
- Neurologic Disorders Part 4Document99 pagesNeurologic Disorders Part 4Aly RiveraNo ratings yet
- Pathology of Cns InfectionsDocument39 pagesPathology of Cns Infectionsskin_docNo ratings yet
- Enchepalitis UkdiDocument13 pagesEnchepalitis Ukdinabila maulidianaNo ratings yet
- Presentation On MeningitisDocument51 pagesPresentation On Meningitissushma shresthaNo ratings yet
- Neurologic Disorders Part 4Document53 pagesNeurologic Disorders Part 4Charlyn JenselNo ratings yet
- Session 39 MeningitisDocument25 pagesSession 39 MeningitisJohn MoshaNo ratings yet
- RashidDocument18 pagesRashidpathan rashid khanNo ratings yet
- Infectious and Inflammatory Diseases of Brain and Spinal CordDocument50 pagesInfectious and Inflammatory Diseases of Brain and Spinal CordKeerthana BNo ratings yet
- Viral MeningitisDocument19 pagesViral MeningitisUneebNo ratings yet
- #3 Infectious and Inflammatory - MeningitisDocument28 pages#3 Infectious and Inflammatory - MeningitisDessy Christiani Part IINo ratings yet
- Viral Diseases of The Central Nervous SystemDocument18 pagesViral Diseases of The Central Nervous System46nv7gphxzNo ratings yet
- Blank 10Document7 pagesBlank 10Leomer Calderon jr.No ratings yet
- Meningitis &encephalitisDocument9 pagesMeningitis &encephalitisSnIP StandredNo ratings yet
- CNS InfectionsDocument20 pagesCNS InfectionsAhmad Alzu3beNo ratings yet
- Inflammation of CNSDocument38 pagesInflammation of CNSTauqeer AhmedNo ratings yet
- D17B PresentationDocument28 pagesD17B PresentationBruno KandatamNo ratings yet
- Meningitis - Introduction and ManagementDocument27 pagesMeningitis - Introduction and ManagementAmmo KhanNo ratings yet
- Meningitis and Dementia: Dr. Lubna DwerijDocument52 pagesMeningitis and Dementia: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Neurological InfectionsDocument21 pagesNeurological Infectionsfortuneholiness11No ratings yet
- EncephalitisDocument37 pagesEncephalitisPRADEEPNo ratings yet
- Intracranial Infection - Prof SunartiniDocument12 pagesIntracranial Infection - Prof SunartiniFranciscus BuwanaNo ratings yet
- MeningitisDocument11 pagesMeningitisManggara Surya DharmaNo ratings yet
- Central Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPDocument72 pagesCentral Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPBenjamin PrabhuNo ratings yet
- Meningit IS: Vicjane A. Gabuco BSN 3A-Group 2 Manuel S. Enverga University Foundation San Lazaro HospitalDocument15 pagesMeningit IS: Vicjane A. Gabuco BSN 3A-Group 2 Manuel S. Enverga University Foundation San Lazaro Hospitaluchiha japeNo ratings yet
- Acute Bacterial MeningitisDocument15 pagesAcute Bacterial MeningitisOana StefanNo ratings yet
- Neuro InfectionsDocument71 pagesNeuro Infectionssrushtideokar0537No ratings yet
- MeningitisDocument64 pagesMeningitisubafran92No ratings yet
- LP EncephalitisDocument28 pagesLP EncephalitisAmar DoanxNo ratings yet
- MeningitisDocument12 pagesMeningitisDany100% (5)
- Infection of CNSDocument6 pagesInfection of CNSsagessenguegangNo ratings yet
- Brain InfectionDocument61 pagesBrain Infectionmanisha paikarayNo ratings yet
- Pathology of The Central Nervous SystemDocument78 pagesPathology of The Central Nervous Systemعلي عليNo ratings yet
- Infectious Diseases - 03Document23 pagesInfectious Diseases - 03Arthur YanezNo ratings yet
- EncephalitisDocument39 pagesEncephalitisSANYA KUNDRA dpsruNo ratings yet
- Cerebrospinal MeningitisDocument11 pagesCerebrospinal Meningitisraphael chidiebereNo ratings yet
- Meningitis - Practice Essentials, Background, PathophysiologyDocument26 pagesMeningitis - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- MeningitisDocument23 pagesMeningitisPutri RamadhaniNo ratings yet
- Central Nervous System (CNS) InfectionsDocument42 pagesCentral Nervous System (CNS) Infectionsapi-3699361100% (3)
- Bacterial Meningitis: Etiology and PathophysiologyDocument9 pagesBacterial Meningitis: Etiology and PathophysiologyIndra Dwi VerawatiNo ratings yet
- Report Kay Sir MeningDocument2 pagesReport Kay Sir MeningPeter John CaballejosNo ratings yet
- 2020 11 20 CNS Infections MitsiasDocument75 pages2020 11 20 CNS Infections MitsiasΖέτα ΤσίρκαNo ratings yet
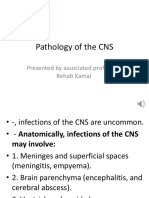
- Pathology of The CNS: Presented by Associated Professor/ Rehab KamalDocument25 pagesPathology of The CNS: Presented by Associated Professor/ Rehab KamalAhmed TarekNo ratings yet
- B.I.Sharapov - Thefounderofthemoldavian Neurologicalschool: of PrimaryDocument4 pagesB.I.Sharapov - Thefounderofthemoldavian Neurologicalschool: of PrimaryDoina CneagnitchiNo ratings yet
- BffsDocument60 pagesBffsdrewantaNo ratings yet
- College of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisDocument9 pagesCollege of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisAmlan jyoti thanapati100% (1)
- MENINGITISDocument55 pagesMENINGITISmulengaamos495No ratings yet
- Dr. Dede Gunawan - CURRENT MANAGEMENT OF VIRAL ENCEPHALITIS (Rev)Document28 pagesDr. Dede Gunawan - CURRENT MANAGEMENT OF VIRAL ENCEPHALITIS (Rev)Adnin NugrohoNo ratings yet
- Meningitis & EncephalitisDocument18 pagesMeningitis & EncephalitisZola Ismu ArjunantoNo ratings yet
- CPPP PP P PP PPPPPPP PPDocument3 pagesCPPP PP P PP PPPPPPP PPangelieballesterosNo ratings yet
- Encephalitis and MeningitisDocument37 pagesEncephalitis and MeningitisSri Ram 07No ratings yet
- MeningitisDocument42 pagesMeningitisRajesh YadavNo ratings yet
- Viral Encephalitis: A Clinician's Guide: Practical NeurologyDocument19 pagesViral Encephalitis: A Clinician's Guide: Practical NeurologyCésar Vásquez Aguilar100% (1)
- EncephalitisDocument20 pagesEncephalitisBenita Putri MDNo ratings yet
- Inflammatory Conditions of The BrainDocument52 pagesInflammatory Conditions of The Brainanju rachel joseNo ratings yet
- Tuberculosis of The Central NsDocument74 pagesTuberculosis of The Central Nsderarataye6No ratings yet
- Neurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANDocument33 pagesNeurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANJeremiash Noblesala Dela CruzNo ratings yet
- Ali - CNS InfectionsDocument129 pagesAli - CNS InfectionsMichael BortzNo ratings yet
- Infections of The Central: Nervous SystemDocument92 pagesInfections of The Central: Nervous SystemIsabel CastilloNo ratings yet
- Encephalitis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandEncephalitis, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (16)
- OlanzapineDocument1 pageOlanzapineKallie ChartrandNo ratings yet
- Short Table of Muscle Control Exercises - The MaxaldingDocument48 pagesShort Table of Muscle Control Exercises - The MaxaldingHugo Mantilla90% (10)
- Riko Technical Brochure PDFDocument29 pagesRiko Technical Brochure PDFGrigoreOzonNo ratings yet
- SPE 13932 Wettability Part2 AndersonDocument17 pagesSPE 13932 Wettability Part2 AndersonSergio EduardoNo ratings yet
- Material Sub Group Item CodeDocument2,818 pagesMaterial Sub Group Item Codegouri gouriNo ratings yet
- Emotional IntelligenceDocument43 pagesEmotional IntelligenceMelody ShekharNo ratings yet
- Parent Medical CoverageDocument9 pagesParent Medical CoveragecampeonNo ratings yet
- SDS Hardener 2750 EN 221004Document10 pagesSDS Hardener 2750 EN 221004juprykaNo ratings yet
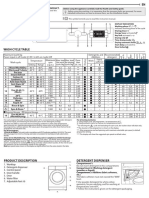
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Rice Sector PACRA - 1604759631Document29 pagesRice Sector PACRA - 1604759631Huzefa SarayiNo ratings yet
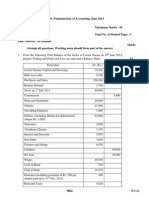
- Capinew Account June13Document7 pagesCapinew Account June13ashwinNo ratings yet
- Medical Entrance Exam - 2022: Test No. 3Document20 pagesMedical Entrance Exam - 2022: Test No. 3soyel afridiNo ratings yet
- Analise de Agua e EfluentesDocument28 pagesAnalise de Agua e EfluentesFabiano Luiz NavesNo ratings yet
- Lock Out Tag Out: Review QuestionsDocument37 pagesLock Out Tag Out: Review QuestionsMansoor AliNo ratings yet
- CSF PDFDocument58 pagesCSF PDFVas KannanNo ratings yet
- Mina NEGRA HUANUSHA 2 ParteDocument23 pagesMina NEGRA HUANUSHA 2 ParteRoberto VillegasNo ratings yet
- ME Lab 2 LectureDocument5 pagesME Lab 2 LectureIan Paul TongolNo ratings yet
- Critikon Dinamap MPS - Product Description PDFDocument9 pagesCritikon Dinamap MPS - Product Description PDFJulio Benancio ZuluagaNo ratings yet
- Developments in The Internal Dosimetry of Radiopharmaceuticals.Document6 pagesDevelopments in The Internal Dosimetry of Radiopharmaceuticals.Edis ĐedovićNo ratings yet
- BWT - HandbookDocument16 pagesBWT - HandbookDarko DuiloNo ratings yet
- Activated Carbon MSDS PDFDocument6 pagesActivated Carbon MSDS PDFRIANG TRIANDONONo ratings yet
- Dan Sof TG 0122Document30 pagesDan Sof TG 0122Erick Trujillo100% (1)
- It's A Safe World After All : TÜV FS EngineerDocument5 pagesIt's A Safe World After All : TÜV FS Engineerizadi1979No ratings yet
- Soil Acidity and LimingDocument12 pagesSoil Acidity and LimingEloi Carlos GoveNo ratings yet
- Automatic Control Basic Course: Exercises 2021Document124 pagesAutomatic Control Basic Course: Exercises 2021Duc-Duy Pham NguyenNo ratings yet
- On Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Document9 pagesOn Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Ansh MishraNo ratings yet
- Acceptance Criteria of Weld Defects As Per Different CodesDocument17 pagesAcceptance Criteria of Weld Defects As Per Different CodesMidhun K Chandrabose96% (25)