Download as pptx, pdf, or txt
You might also like
- Scribe Letter 1 - 10082021104121Document4 pagesScribe Letter 1 - 10082021104121Bob LeeNo ratings yet
- Important Questions Answers Why This Matters:: IndividualDocument7 pagesImportant Questions Answers Why This Matters:: Individualsashank varmaNo ratings yet
- Book 9-10 DelhiDocument19 pagesBook 9-10 DelhiDrnuzhat FatemaNo ratings yet
- AHM-250 Day IIIDocument77 pagesAHM-250 Day IIIArnabNo ratings yet
- Health Economics Note Chapter 12Document12 pagesHealth Economics Note Chapter 12Farian Tahrim VikiNo ratings yet
- Lva1 App6891Document63 pagesLva1 App6891Anil Kumar ARSNo ratings yet
- Whose Patient Is ItDocument3 pagesWhose Patient Is ItSean RNo ratings yet
- PremiumPlus 2023 Benefit Guide 1Document36 pagesPremiumPlus 2023 Benefit Guide 1Ntando MpiyakheNo ratings yet
- Lva1 App6891Document63 pagesLva1 App6891Anil Kumar ARSNo ratings yet
- MediValue 2023 Benefit GuideDocument36 pagesMediValue 2023 Benefit GuideTalita JonkerNo ratings yet
- What Is Managed CareDocument18 pagesWhat Is Managed CareYOGESHNo ratings yet
- MCO - Financial ArragementsDocument5 pagesMCO - Financial ArragementsharshakarnaNo ratings yet
- AHM250 PPOsAndOtherPlanTypesDocument6 pagesAHM250 PPOsAndOtherPlanTypesMohit SainiNo ratings yet
- AHM 250 4 Provider CompensationDocument16 pagesAHM 250 4 Provider Compensationdeepakraj610No ratings yet
- Health Economics - Lecture Ch12Document61 pagesHealth Economics - Lecture Ch12Katherine SauerNo ratings yet
- Bestmed Guide To Prescribed Minimum Benefits 2023 V100 20230316 WebDocument8 pagesBestmed Guide To Prescribed Minimum Benefits 2023 V100 20230316 WebMpumeleloNo ratings yet
- Bronze-7-Epo-1 1 22-12 31 22Document8 pagesBronze-7-Epo-1 1 22-12 31 22PSC RFQNo ratings yet
- United Healthcare Insurance PlansDocument16 pagesUnited Healthcare Insurance PlansMavisNo ratings yet
- 16 Chapter 7Document62 pages16 Chapter 7Sairaj SankpalNo ratings yet
- Managed Care - Premi - Permbayaran - PPK PDFDocument29 pagesManaged Care - Premi - Permbayaran - PPK PDFulfah mNo ratings yet
- Chapter 6 - Capitation in Provider ReimbursementDocument23 pagesChapter 6 - Capitation in Provider ReimbursementAdityaNo ratings yet
- NHCX PresentationDocument7 pagesNHCX Presentationfoxan67683No ratings yet
- Module 1 - RCMDocument66 pagesModule 1 - RCMaiithulee.itsmeNo ratings yet
- Basics of HealthCare DomainDocument4 pagesBasics of HealthCare DomainRajivNo ratings yet
- Medical HealthDocument50 pagesMedical HealthHihiNo ratings yet
- Chapter 8 - Managed Care PlansDocument0 pagesChapter 8 - Managed Care PlansJonathon CabreraNo ratings yet
- Allowed Amount Balance Billing Coinsurance Copayment Deductible ProviderDocument7 pagesAllowed Amount Balance Billing Coinsurance Copayment Deductible Providergary kornegayNo ratings yet
- MIS PricesDocument50 pagesMIS PricesAndy GuraNo ratings yet
- 1009 Swigert PDFDocument143 pages1009 Swigert PDFMayraNo ratings yet
- INA CBGs Dan PPK7.ppt (Compatibility Mode)Document65 pagesINA CBGs Dan PPK7.ppt (Compatibility Mode)Casemix rsudwaledNo ratings yet
- Health Insurance Contract-GisselleDocument10 pagesHealth Insurance Contract-GisselleMariz BallonNo ratings yet
- 15 Chapter 6Document35 pages15 Chapter 6Sairaj SankpalNo ratings yet
- SHBP SBC Twin Cities Campus Student Only 2017-2018Document8 pagesSHBP SBC Twin Cities Campus Student Only 2017-2018hotshinhwanatecomNo ratings yet
- Hca Health Services of Georgia, Inc. v. Employers Health Insurance Company, 240 F.3d 982, 11th Cir. (2001)Document37 pagesHca Health Services of Georgia, Inc. v. Employers Health Insurance Company, 240 F.3d 982, 11th Cir. (2001)Scribd Government DocsNo ratings yet
- Health Insurance 2Document7 pagesHealth Insurance 2Esra AljabriNo ratings yet
- Health Insurance Domain Basics PDFDocument47 pagesHealth Insurance Domain Basics PDFGautam Kumar DwivedyNo ratings yet
- Textbook of Urgent Care Management: Chapter 22, Health Plan ContractingFrom EverandTextbook of Urgent Care Management: Chapter 22, Health Plan ContractingNo ratings yet
- Who Is Driving The Interest in OualityDocument10 pagesWho Is Driving The Interest in Oualitymzahid7823No ratings yet
- Nsa Health Insurance BasicsDocument7 pagesNsa Health Insurance BasicsMaliNo ratings yet
- HDHPDocument10 pagesHDHPAnonymous KnnAxcNo ratings yet
- Contemporary Nursing Issues Trends and Management 5th Edition Cherry Test BankDocument39 pagesContemporary Nursing Issues Trends and Management 5th Edition Cherry Test Bankseeressgroined3djz100% (17)
- Chapter 1 Key Terms: Accountable Care Organization (ACO)Document3 pagesChapter 1 Key Terms: Accountable Care Organization (ACO)bruhNo ratings yet
- Healthcare GlossaryDocument18 pagesHealthcare GlossaryKalagara Mohan KrishnaNo ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersGeraldine HerreraNo ratings yet
- © Benefitexpress 2016Document31 pages© Benefitexpress 2016Vicente TorresNo ratings yet
- ANIKET ARYAN 2211380 HETPSection1 Aniket Aryan 129618 38254896Document2 pagesANIKET ARYAN 2211380 HETPSection1 Aniket Aryan 129618 38254896SANo ratings yet
- Important Points About Your Cover BHF 10689Document17 pagesImportant Points About Your Cover BHF 10689ijas ahmedNo ratings yet
- Mediplus: 2019 Benefit GuideDocument24 pagesMediplus: 2019 Benefit GuideBruce FerreiraNo ratings yet
- InsuranceDocument24 pagesInsurancekanikabagariaNo ratings yet
- Beat 3 Product Brochure 2022ENG 20210902 WebDocument16 pagesBeat 3 Product Brochure 2022ENG 20210902 WebKamogelo NtsokoNo ratings yet
- Healthcare BasicsDocument57 pagesHealthcare BasicsManickavel Manoharan100% (2)
- Health Insurance 2Document32 pagesHealth Insurance 2roquiemayursaizNo ratings yet
- AM Organisational Overview of GEMS PDFDocument26 pagesAM Organisational Overview of GEMS PDFAmit SharmaNo ratings yet
- Health Services Health Financing Health UtilizationDocument14 pagesHealth Services Health Financing Health UtilizationRizki YulisetiawanNo ratings yet
- MIS AssignmentDocument3 pagesMIS AssignmentMOHAMAD FERDIANSYAH ARIFIN BIN OMER SA'AIB STUDENTNo ratings yet
- Math - Mental IllnessDocument5 pagesMath - Mental Illnessapi-493788043No ratings yet
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersQFQEWFWQEFwqNo ratings yet
- Aligning Reimbursement With Value - Institute For Strategy and Competitiveness - Harvard Business SchoolDocument1 pageAligning Reimbursement With Value - Institute For Strategy and Competitiveness - Harvard Business SchoolTuan Nguyen DangNo ratings yet
- Glossary of Billing TermsDocument8 pagesGlossary of Billing Termsnallaakhil741No ratings yet
- Important Questions Answers Why This Matters:: (G3970/P2364) (G3971/P2364)Document8 pagesImportant Questions Answers Why This Matters:: (G3970/P2364) (G3971/P2364)JskNo ratings yet
- Aetna SBC 2024 Standard Plan Express ScriptsDocument15 pagesAetna SBC 2024 Standard Plan Express Scriptskatika3011No ratings yet
- Third Party Administrator: Submitted By: Tiyasa Mukherjee Pallabi Palit Shramana Ghosh Debapriya MukherjeeDocument13 pagesThird Party Administrator: Submitted By: Tiyasa Mukherjee Pallabi Palit Shramana Ghosh Debapriya MukherjeeTiyasa Kaaju MukherjeeNo ratings yet
- BUSINESS MATHEMATICS Lesson 5 IONDocument9 pagesBUSINESS MATHEMATICS Lesson 5 IONPurple. Queen95100% (2)
- Hike - Participant WaiverDocument2 pagesHike - Participant Waiverlimber dameciousNo ratings yet
- Quarter 1 Lesson 1-2 ReviewerDocument4 pagesQuarter 1 Lesson 1-2 ReviewerVenice SolverNo ratings yet
- Health 10 Health Professionals and FacilitiesDocument33 pagesHealth 10 Health Professionals and FacilitiesJM GuerreroNo ratings yet
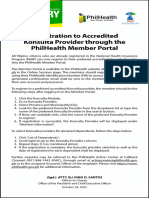
- PhilHealth Advisory No. 2022-0036 Registration To Konsulta ProviderDocument1 pagePhilHealth Advisory No. 2022-0036 Registration To Konsulta ProviderElmer NeriNo ratings yet
- Test Bank For Understanding Hospital Coding and Billing 3rd Edition by DiamondDocument6 pagesTest Bank For Understanding Hospital Coding and Billing 3rd Edition by DiamondJames Colon100% (30)
- Health Care Reform Research Paper OutlineDocument7 pagesHealth Care Reform Research Paper Outlinevguomivnd100% (1)
- Page - 1Document3 pagesPage - 1SHAIK SHABEENANo ratings yet
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument9 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- Company Name Contact OwnerDocument135 pagesCompany Name Contact OwnerShahriar KabirNo ratings yet
- Jurnal PRBDocument5 pagesJurnal PRBJoanne AngelinaNo ratings yet
- Star PREMIUM CHART 18%Document5 pagesStar PREMIUM CHART 18%Rajat GuptaNo ratings yet
- Prospective PaymentDocument68 pagesProspective PaymentBassam AlqadasiNo ratings yet
- Health Insurance Term PaperDocument4 pagesHealth Insurance Term Paperafdtslawm100% (1)
- Health Promotion Throughout The Life Span 7th Edition Edelman Test BankDocument11 pagesHealth Promotion Throughout The Life Span 7th Edition Edelman Test BankJosephJohnsonfmixo100% (14)
- Health Care Delivery System 1Document21 pagesHealth Care Delivery System 1Carson BirthNo ratings yet
- Lesson 2 Consumer Health EducationDocument36 pagesLesson 2 Consumer Health EducationJerick SubadNo ratings yet
- Claims ProcessDocument1 pageClaims ProcessRutvik ShahNo ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- Analysis of A Pertinent Healthcare IssueDocument6 pagesAnalysis of A Pertinent Healthcare Issuejossy MulingeNo ratings yet
- Instructors Manual 6th EditionDocument120 pagesInstructors Manual 6th EditionSean BokelmannNo ratings yet
- Claim Form My Health Suraksha Oct 2020 HEHIDocument5 pagesClaim Form My Health Suraksha Oct 2020 HEHIMOHNISH MANCHALWARNo ratings yet
- Child Care Emergency Contact Information and Consent Form Template-79400Document1 pageChild Care Emergency Contact Information and Consent Form Template-79400Thriftyshop StoreNo ratings yet
- Tanzania UHI Act 2023 Policy BriefDocument6 pagesTanzania UHI Act 2023 Policy Briefgeophrey kajokiNo ratings yet
- Dental Safety Net Facilities - 2023Document5 pagesDental Safety Net Facilities - 2023dashahutchinsonNo ratings yet
- SuperSHIP - Smart Super Health Insurance PolicyDocument28 pagesSuperSHIP - Smart Super Health Insurance PolicyNitin GuptaNo ratings yet
- NATHEALTH HealthFinancing ThoughtLeadershipPaperDocument48 pagesNATHEALTH HealthFinancing ThoughtLeadershipPaperVansh AggarwalNo ratings yet
- NURS FPX 6618 Assessment 2 Mobilizing Care For An Immigrant PopulationDocument5 pagesNURS FPX 6618 Assessment 2 Mobilizing Care For An Immigrant Populationfarwaamjad771No ratings yet