Download as pptx, pdf, or txt
You might also like
- Pictorial Atlas of Botulinum Toxin Injection. Dosage Localization Application. (1) PDF PDFDocument2 pagesPictorial Atlas of Botulinum Toxin Injection. Dosage Localization Application. (1) PDF PDFTeng Lip Yuen40% (5)
- Post-Traumatic Elbow Stiffness - Arthrolysis and Mechanical DistractionDocument31 pagesPost-Traumatic Elbow Stiffness - Arthrolysis and Mechanical DistractionAna-Maria ȘtefanNo ratings yet
- GKS Prime Flex ATTITUDE Instrument Set - ENDocument32 pagesGKS Prime Flex ATTITUDE Instrument Set - ENosama abdulrhman100% (1)
- Reflexology Charts and Relaxation TechniquesDocument12 pagesReflexology Charts and Relaxation TechniquesJanetOllman100% (13)
- What Is Traction?Document5 pagesWhat Is Traction?Tweenie DalumpinesNo ratings yet
- Cast/Splint Choice and Application: Worku K. (MD)Document15 pagesCast/Splint Choice and Application: Worku K. (MD)Worku KifleNo ratings yet
- CTEVDocument24 pagesCTEVwildanmalikNo ratings yet
- "Must Know" Classifications: Gustillo Salter-HarrisDocument4 pages"Must Know" Classifications: Gustillo Salter-HarrisHo Yong WaiNo ratings yet
- (Upgraded) Damage Control Orthopaedics DR Bambang SpOTDocument37 pages(Upgraded) Damage Control Orthopaedics DR Bambang SpOTroroNo ratings yet
- Biomechanics of Fractures and FixationDocument87 pagesBiomechanics of Fractures and FixationShreya AgarwalNo ratings yet
- The Tamil Nadu Dr. M.G.R Medical University: Dissertation Submitted ToDocument129 pagesThe Tamil Nadu Dr. M.G.R Medical University: Dissertation Submitted ToAmmar AlnajjarNo ratings yet
- ORP Handout English External Fixation NlogoDocument9 pagesORP Handout English External Fixation NlogotripodegrandeNo ratings yet
- Basinga Idys C ZPDocument26 pagesBasinga Idys C ZPruiduartNo ratings yet
- Dermatology NLC DR Manish Soni 2021Document94 pagesDermatology NLC DR Manish Soni 2021akashineeNo ratings yet
- Funda Lab Mod 5-7Document13 pagesFunda Lab Mod 5-7Liane BartolomeNo ratings yet
- 05 Fractures of The Upper Extremity Part 2 - Dr. TanDocument75 pages05 Fractures of The Upper Extremity Part 2 - Dr. TanMonique BorresNo ratings yet
- New Price List Suture Fy21Document72 pagesNew Price List Suture Fy21OPERATING THEATER PHSBNo ratings yet
- Arthritis: Septic Arthritis and Tuberculosis ArthritisDocument10 pagesArthritis: Septic Arthritis and Tuberculosis Arthritistaufikoling100% (1)
- 12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFDocument7 pages12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFTolo CantallopsNo ratings yet
- Tibia and Fibula Shaft Fracture in Pediatric Case (Ola)Document20 pagesTibia and Fibula Shaft Fracture in Pediatric Case (Ola)Junarto Putra Tandiarrang100% (1)
- Pharmacological Treatment of Vertigo: Timothy C. Hain and Mohammed UddinDocument16 pagesPharmacological Treatment of Vertigo: Timothy C. Hain and Mohammed UddinFan AccountNo ratings yet
- A AaaaaaaDocument6 pagesA AaaaaaaAnonymous d9Bzr1No ratings yet
- Amputation, Surgery and RehabilitationDocument46 pagesAmputation, Surgery and RehabilitationPatrick WandellahNo ratings yet
- Interface Pressure Between Socket - Using TekscanDocument207 pagesInterface Pressure Between Socket - Using TekscanSérgio SilvaNo ratings yet
- Suprapubic CathetherisationDocument33 pagesSuprapubic CathetherisationWahyuWNo ratings yet
- Anatomy of The EarDocument63 pagesAnatomy of The EargabrielNo ratings yet
- Journeyii CR 00344v1 UsDocument40 pagesJourneyii CR 00344v1 UsSufyanNo ratings yet
- Lateral Condyle FractureDocument4 pagesLateral Condyle Fracturesaraswaty710No ratings yet
- 2020-07-07 Reconstructive Ladder FlapDocument96 pages2020-07-07 Reconstructive Ladder FlapTonie AbabonNo ratings yet
- Pharma Handouts Rev 3Document34 pagesPharma Handouts Rev 3Aphrill Pearl PacisNo ratings yet
- Amputation RehabilitationDocument59 pagesAmputation RehabilitationAnushree DatarNo ratings yet
- Ankle Distraction ArthroplastyDocument15 pagesAnkle Distraction ArthroplastyJon Hook100% (1)
- 3 Soft Tissue Injury HabtamuDocument80 pages3 Soft Tissue Injury HabtamuWasihunNo ratings yet
- Evaluacion Inicial Del Paciente QuemadoDocument12 pagesEvaluacion Inicial Del Paciente QuemadoRyan BNo ratings yet
- Jude's Quadriceps Plasty For Stiff KneeDocument6 pagesJude's Quadriceps Plasty For Stiff KneeRaviNo ratings yet
- SJAMS 43B 750 754 Thesis Tibial PlateauDocument5 pagesSJAMS 43B 750 754 Thesis Tibial PlateauNisheshJainNo ratings yet
- Bone BankDocument2 pagesBone BankMd Ahsanuzzaman PinkuNo ratings yet
- Elbow ApproachesDocument1 pageElbow ApproachesSaad Allah KabbanyNo ratings yet
- Current Concepts in Lower Extremity Reconstruction.36Document15 pagesCurrent Concepts in Lower Extremity Reconstruction.36Aura RivasNo ratings yet
- Shoulder and Elbow Scored and Recorded Self-Assessment ExaminationDocument73 pagesShoulder and Elbow Scored and Recorded Self-Assessment ExaminationZia Ur RehmanNo ratings yet
- External Fixation: Nursing Best Practice GuidelinesDocument25 pagesExternal Fixation: Nursing Best Practice GuidelinesDoneva Lyn MedinaNo ratings yet
- Block 1 OMM Written Exam 1 ReviewDocument20 pagesBlock 1 OMM Written Exam 1 Reviewjoe doweNo ratings yet
- Inverted L OsteotomyDocument9 pagesInverted L OsteotomyhaneefmdfNo ratings yet
- Clavo para ClaviculaDocument12 pagesClavo para ClaviculaMartinLydenNo ratings yet
- Trans SaVi Oto Lec 03 Diseases of The External and Middle EarDocument13 pagesTrans SaVi Oto Lec 03 Diseases of The External and Middle EarJoherNo ratings yet
- Amputation: Sites of Amputation: UEDocument6 pagesAmputation: Sites of Amputation: UEChristine PilarNo ratings yet
- Case ReportDocument19 pagesCase Reportrizaldy syahNo ratings yet
- Kuliah Spine TraumaDocument91 pagesKuliah Spine Traumatutor tujuhNo ratings yet
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsDocument7 pagesTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersNo ratings yet
- Early Total Care To Early Appropriate Care What.2Document8 pagesEarly Total Care To Early Appropriate Care What.2ChrisNo ratings yet
- Care of Patient With CastDocument31 pagesCare of Patient With Castيلا كورة شوت beIn sportNo ratings yet
- Difficult Debriefing Situations A Toolbox For Simulation EducatorsDocument11 pagesDifficult Debriefing Situations A Toolbox For Simulation Educatorsdanfer_99100% (1)
- SUTGMultiLocJ9981A PDFDocument60 pagesSUTGMultiLocJ9981A PDFLouis MiuNo ratings yet
- Quiet QuittingDocument2 pagesQuiet Quittingavy28No ratings yet
- Forearm Fractures FinalDocument8 pagesForearm Fractures FinalApolinar González HernándezNo ratings yet
- Papineau TechniqueDocument12 pagesPapineau TechniqueDito WadhikoNo ratings yet
- Bandaging and SplintingDocument88 pagesBandaging and Splintinggbsreg gbsregNo ratings yet
- Principles in Fracture ManagementDocument60 pagesPrinciples in Fracture ManagementNge NgeNo ratings yet
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDocument20 pagesDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNo ratings yet
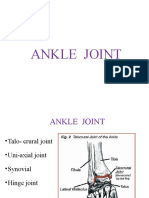
- Ankle JointDocument29 pagesAnkle JointRamakrishnanNo ratings yet
- BandagingDocument42 pagesBandagingMuhammad Shahzad ChandiaNo ratings yet
- Health Assistant ClassDocument47 pagesHealth Assistant ClassAbhishek TandonNo ratings yet
- Range of MotionDocument59 pagesRange of MotionIsrael Jiel Fedelicio100% (1)
- Rheumatoid ArthritisDocument52 pagesRheumatoid ArthritisArun NingarajappaNo ratings yet
- Facial Spaces of HandDocument15 pagesFacial Spaces of HandcrossNo ratings yet
- CylinderDocument15 pagesCylinderJacob LanesNo ratings yet
- Paid Orthobullet MCQs - HandDocument130 pagesPaid Orthobullet MCQs - HandShiKid COMIX-GAMENo ratings yet
- Baseline 3 Piece Hand Evaluation Set User ManualDocument2 pagesBaseline 3 Piece Hand Evaluation Set User ManualphcproductsNo ratings yet
- Is 15836-3 (2008) ISO 15534-3 2000 Ergonomic Design For The Safety of Machinery, Part 3 Anthropometric DataDocument10 pagesIs 15836-3 (2008) ISO 15534-3 2000 Ergonomic Design For The Safety of Machinery, Part 3 Anthropometric DataSiva Kumar PLNo ratings yet
- Muscles of The Upper Limb - Listed Alphabetically Muscle Origin Insertion Action Innervation Artery NotesDocument10 pagesMuscles of The Upper Limb - Listed Alphabetically Muscle Origin Insertion Action Innervation Artery NotesAjay Pal NattNo ratings yet
- Myoelectric Prosthetic Hand With A Proprioceptive Feedback SystemDocument8 pagesMyoelectric Prosthetic Hand With A Proprioceptive Feedback SystemLaura PasqualNo ratings yet
- Upper Limbs NOTES - BRS Anatomy, Table of Muscles and BRS Questions With Answers ExplainedDocument14 pagesUpper Limbs NOTES - BRS Anatomy, Table of Muscles and BRS Questions With Answers ExplainedJustyna PoznanskaNo ratings yet
- Muscles of Back of ForearmDocument15 pagesMuscles of Back of ForearmInsyirah JohariNo ratings yet
- Mobile Phones & Tablets Tips: Accounting For TouchDocument5 pagesMobile Phones & Tablets Tips: Accounting For TouchAjay KumarNo ratings yet
- IN OUR HANDS e BookDocument60 pagesIN OUR HANDS e BookBeffaraNo ratings yet
- Fascia of Upper LimbDocument45 pagesFascia of Upper LimbZaineb FarooqNo ratings yet
- Hand and UE Injuries ArthritisDocument2 pagesHand and UE Injuries ArthritisOlivia MNo ratings yet
- Goniometry RevisedDocument12 pagesGoniometry RevisedKali AceñaNo ratings yet
- Tabel KinesiologiDocument4 pagesTabel KinesiologiMohammad Jofa Rachman PNo ratings yet
- Successful Beginnings: Lesson 1Document25 pagesSuccessful Beginnings: Lesson 1lucidekeNo ratings yet
- A 3D Printed, Bionic Hand Powered by EMG Signals and Controlled by An Online Neural NetworkDocument33 pagesA 3D Printed, Bionic Hand Powered by EMG Signals and Controlled by An Online Neural NetworkDr Edward PeterNo ratings yet
- Playing Djembe PDFDocument63 pagesPlaying Djembe PDFpbanerjeeNo ratings yet
- Technique Packet-TenorsDocument10 pagesTechnique Packet-Tenorsapi-186882135No ratings yet
- Orthopedics Nerve InjuryDocument6 pagesOrthopedics Nerve InjuryPravinNo ratings yet
- Module 5 - THXDocument13 pagesModule 5 - THXZgama AbdulrahmanNo ratings yet
- Active and Passive InsufficiencyDocument25 pagesActive and Passive Insufficiencydina sharafNo ratings yet
- The Contents of Anatomical Snuff Box AreDocument3 pagesThe Contents of Anatomical Snuff Box AreZimam ZamriNo ratings yet
- Brachial Plexus PowerpointDocument32 pagesBrachial Plexus PowerpointZulkarnain Syamsuri100% (1)
- Exam Table For Hand Wrist ForearmDocument22 pagesExam Table For Hand Wrist ForearmLouie OkayNo ratings yet
- Donning of Gloves and GownDocument3 pagesDonning of Gloves and GownArmie Joy Embat Cariazo100% (1)