Download as pptx, pdf, or txt
You might also like
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- Dyslipdiemia 2022Document75 pagesDyslipdiemia 2022LeeNo ratings yet
- Slide Himawan Liphantyl Febr 2021Document43 pagesSlide Himawan Liphantyl Febr 2021Muliani AwalNo ratings yet
- Kelompok 1Document14 pagesKelompok 1Aurent WidjanarkoNo ratings yet
- Roseday EZ Webinar SlidesDocument35 pagesRoseday EZ Webinar SlidesPragnesh ShahNo ratings yet
- DyslipidemiaDocument53 pagesDyslipidemiaRey AlwiwikhNo ratings yet
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocument6 pagesNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaNo ratings yet
- Understanding The Needs of The High Productive DyslipidemiaDocument47 pagesUnderstanding The Needs of The High Productive DyslipidemiachchchchkNo ratings yet
- Dislipid 2 PDFDocument4 pagesDislipid 2 PDFWahyuningsih HamidNo ratings yet
- The Importance of Potential Statin in High Risk PatientDocument56 pagesThe Importance of Potential Statin in High Risk PatientAidil Fittriani AyuNo ratings yet
- Cholesterol Guidelines Review 2020Document6 pagesCholesterol Guidelines Review 2020oriannaocantoNo ratings yet
- Applicability of Recent Dyslipidemia Guidelines in Clinical PracticeDocument4 pagesApplicability of Recent Dyslipidemia Guidelines in Clinical PracticeDokter FebyanNo ratings yet
- Dyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016Document31 pagesDyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016aprinaaaNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- Dyslipidemia 2018Document8 pagesDyslipidemia 2018R JannahNo ratings yet
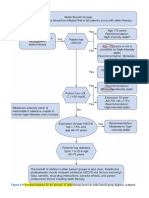
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- TX LipidosDocument14 pagesTX Lipidosxander trujilloNo ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Diabetes and Dsylipidemia SalinanDocument38 pagesDiabetes and Dsylipidemia SalinanAnonymous xnVguFYNo ratings yet
- Small Dense Low-Density Lipoprotein As Risk Factor For Atherosclerosis in Type 2 Diabetes MellitusDocument4 pagesSmall Dense Low-Density Lipoprotein As Risk Factor For Atherosclerosis in Type 2 Diabetes Mellitusjamal khanNo ratings yet
- ACC Handbook Ascvd Type 2 Diabetes: On andDocument10 pagesACC Handbook Ascvd Type 2 Diabetes: On andZH. omg sarNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Arb in Hypertension Management: Focused On Telmisartan: Akhtar Fajar MuzakkirDocument40 pagesArb in Hypertension Management: Focused On Telmisartan: Akhtar Fajar MuzakkirFidel Martua MarpaungNo ratings yet
- Cholesterol-Lowering Agents Statins-For Everyone? 2019Document10 pagesCholesterol-Lowering Agents Statins-For Everyone? 2019Luis Alberto Alvarez AnkassNo ratings yet
- New Developments in The Management of DyslipidemiaDocument63 pagesNew Developments in The Management of DyslipidemiaM Azmi HNo ratings yet
- RosuvastatinDocument62 pagesRosuvastatinEileen del RosarioNo ratings yet
- Ann Soehee - Tctap2021 - SPCDocument43 pagesAnn Soehee - Tctap2021 - SPCSaad KhanNo ratings yet
- Atherothrombosis Drugs Compendium: Cholesterol-Lowering AgentsDocument17 pagesAtherothrombosis Drugs Compendium: Cholesterol-Lowering AgentsSri MaryatiNo ratings yet
- Undangan Rapat PJ UnitDocument1 pageUndangan Rapat PJ UnitDwi HartatiNo ratings yet
- Simpo 2.1Document40 pagesSimpo 2.1chandraNo ratings yet
- Diabetes and DsylipidemiaDocument38 pagesDiabetes and Dsylipidemiafais123No ratings yet
- Narsum 1 Tatalaksana DislipidemiaDocument32 pagesNarsum 1 Tatalaksana DislipidemiabimaNo ratings yet
- Drug Treatment of Lipid Disorders. NIACINA. NIACINDocument14 pagesDrug Treatment of Lipid Disorders. NIACINA. NIACINpaoloaltoeNo ratings yet
- 9.metabolik Sindrome - DR PalgunadiDocument46 pages9.metabolik Sindrome - DR PalgunadiAjeng RetnoNo ratings yet
- A Review of Efficacy RosuvastatinDocument11 pagesA Review of Efficacy RosuvastatindunhowhNo ratings yet
- Dislipidemia Final PresentasikirimulangDocument40 pagesDislipidemia Final PresentasikirimulangZurlin DwirostantinNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- 27 FullDocument6 pages27 FullKrishna R KhanalNo ratings yet
- Cardiometabolic RiskDocument1 pageCardiometabolic RiskVaidya Priyanka SharmaNo ratings yet
- Peroxisome Proliferato-Activated Receptor AlphaDocument10 pagesPeroxisome Proliferato-Activated Receptor Alphaadam shingeNo ratings yet
- CCRR 1 114 PDFDocument3 pagesCCRR 1 114 PDFBruno Mario AngelNo ratings yet
- Austin AndrologyDocument4 pagesAustin AndrologyAustin Publishing GroupNo ratings yet
- Statins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiDocument17 pagesStatins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiMamad TrihatmowidjoyoNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- Cardiovascular Disorders: Annette HaynesDocument69 pagesCardiovascular Disorders: Annette HaynesBinh Yen Quach TranNo ratings yet
- 1 s2.0 S2213177917305358 MainDocument10 pages1 s2.0 S2213177917305358 MainMayar HassanNo ratings yet
- Evidence For Changing Lipid Management Strategy To Focus On Non-High Density Lipoprotein CholesterolDocument7 pagesEvidence For Changing Lipid Management Strategy To Focus On Non-High Density Lipoprotein CholesterolJeje MystearicaNo ratings yet
- Hypertriglyceridemia - Common Causes, Prevention and Treatment StrategiesDocument10 pagesHypertriglyceridemia - Common Causes, Prevention and Treatment Strategiesfaqihu rizkyNo ratings yet
- Jaha 116 004909 PDFDocument8 pagesJaha 116 004909 PDFLisbeth MarbunNo ratings yet
- Unmeet Need Is LDL-C Lowering When Regular Statin Wont DoDocument40 pagesUnmeet Need Is LDL-C Lowering When Regular Statin Wont Doyan salvianto100% (1)
- Reviews: Statins in The Primary Prevention of Cardiovascular DiseaseDocument12 pagesReviews: Statins in The Primary Prevention of Cardiovascular DiseaseCrischentian BrinzaNo ratings yet
- SummaryDocument2 pagesSummarychiprovin4308No ratings yet
- Guidelines DyslipidDocument49 pagesGuidelines Dyslipidnoveldycb89No ratings yet
- Life-Style-Induced Metabolic Derangement and Epigenetic Changes Promote Diabetes and Oxidative Stress Leading To NASH and Atherosclerosis SeverityDocument11 pagesLife-Style-Induced Metabolic Derangement and Epigenetic Changes Promote Diabetes and Oxidative Stress Leading To NASH and Atherosclerosis SeverityAulia Nurul IzzahNo ratings yet
- Edit Virtual HR Managing Dyslipidemia in Special PopulationDocument38 pagesEdit Virtual HR Managing Dyslipidemia in Special PopulationIkmah FauzanNo ratings yet
- Journal Hypertension and Diabetes Type 2Document20 pagesJournal Hypertension and Diabetes Type 2Andi SusiloNo ratings yet
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDocument6 pagesEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaNo ratings yet
- New Developments in The Management of Dyslipidemia: Widjanarko. W MDDocument62 pagesNew Developments in The Management of Dyslipidemia: Widjanarko. W MDyulanda fitrianaNo ratings yet
- Dr. A. Samy TAG Upper Limb - 1Document20 pagesDr. A. Samy TAG Upper Limb - 1DRAHMEDFAHMYORTHOCLINICNo ratings yet
- Etiqa Group Claims Submission ChecklistDocument3 pagesEtiqa Group Claims Submission ChecklistPnk Telok KemangNo ratings yet
- Ebook Health Psychology An Introduction To Behavior and Health 2 Full Chapter PDFDocument67 pagesEbook Health Psychology An Introduction To Behavior and Health 2 Full Chapter PDFmelanie.ballew774100% (35)
- Final Exam Micropara 101 Lab 2020 2021 Microbiology and Parasitology Lab PDFDocument24 pagesFinal Exam Micropara 101 Lab 2020 2021 Microbiology and Parasitology Lab PDFJuliana MendozaNo ratings yet
- Factors Affecting Physical Activity ParticipationDocument10 pagesFactors Affecting Physical Activity ParticipationCatherine Sagario OliquinoNo ratings yet
- Oral Health in PregnancyDocument6 pagesOral Health in PregnancyTamara Al KautsarNo ratings yet
- Inglés para Médicos IIDocument29 pagesInglés para Médicos IICarla JaegerNo ratings yet
- Business Sales Proposal Sample LetterDocument11 pagesBusiness Sales Proposal Sample LetterMainul HossainNo ratings yet
- Verorab PDFDocument8 pagesVerorab PDFเด็กชายท็อปปิ้ง ชอบกลิ้งเข้าคณะเภสัชศาสตร์No ratings yet
- PIDDocument11 pagesPIDManjuNo ratings yet
- Cholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is TheDocument3 pagesCholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is Thejosias_jorgio1No ratings yet
- Chapter 25 The Child With Cardiovascular DysfunctionDocument20 pagesChapter 25 The Child With Cardiovascular DysfunctionJill Hill100% (3)
- Drug Induced Intracranial Hypertension: A Systematic Review and Critical Assessment of Drug Induced CausesDocument10 pagesDrug Induced Intracranial Hypertension: A Systematic Review and Critical Assessment of Drug Induced CausesSerque777No ratings yet
- Nausea, Vomiting in Pregnancy & Hyperemesis Gravidarum, UPDATE 2024Document30 pagesNausea, Vomiting in Pregnancy & Hyperemesis Gravidarum, UPDATE 2024patsilwalNo ratings yet
- Shoulder Orthosis - DevadriDocument18 pagesShoulder Orthosis - DevadriDevadri DeyNo ratings yet
- Hubungan Faktor Lokal, Faktor Sistemik Dan Faktor Perilaku Terhadap Kejadian Penyakit Periodontal Di Indonesia (Analisis Riskesdas)Document10 pagesHubungan Faktor Lokal, Faktor Sistemik Dan Faktor Perilaku Terhadap Kejadian Penyakit Periodontal Di Indonesia (Analisis Riskesdas)lidyaNo ratings yet
- Session53, Zoom English CafeDocument23 pagesSession53, Zoom English CafeBrosoa LoquaNo ratings yet
- Antibiotics IN Maxillofacial Surgery: Presenter: Dr. Venu G.RDocument92 pagesAntibiotics IN Maxillofacial Surgery: Presenter: Dr. Venu G.RkatnevNo ratings yet
- Rhesus SystemDocument41 pagesRhesus SystemLaud ArthurNo ratings yet
- Prof DR Akram ICUDocument233 pagesProf DR Akram ICUramzi MohamedNo ratings yet
- The Assessment of Mitral Valve Disease: A Guideline From The British Society of EchocardiographyDocument50 pagesThe Assessment of Mitral Valve Disease: A Guideline From The British Society of EchocardiographyAnurag PandeyNo ratings yet
- Presbyastasis A Multifactorial Cause of Balance Problems in The ElderlyDocument5 pagesPresbyastasis A Multifactorial Cause of Balance Problems in The Elderlydarmayanti ibnuNo ratings yet
- HESI LPN ADN ENTRANCE EXAM MOBILITY EXAMS A GRADED 100 VERIFIED - pdf-1-33Document33 pagesHESI LPN ADN ENTRANCE EXAM MOBILITY EXAMS A GRADED 100 VERIFIED - pdf-1-33erick kanyiNo ratings yet
- ParasitologyDocument7 pagesParasitologysumairaNo ratings yet
- System Normal Abnormal Remarks Vital SignsDocument3 pagesSystem Normal Abnormal Remarks Vital SignsJM RomiasNo ratings yet
- Introductory Medical Surgical Nursing Timby 11th Edition Test BankDocument14 pagesIntroductory Medical Surgical Nursing Timby 11th Edition Test Bankteresastoneniegwrjcyt100% (28)
- Pulse Oximetry ArticleDocument6 pagesPulse Oximetry ArticlesvarroggNo ratings yet
- Conversation: For The Second-Year StudentsDocument15 pagesConversation: For The Second-Year StudentsНаташа ПритолюкNo ratings yet
- Daftar Pustaka Dr. Tutty Ariani, SPDVDocument8 pagesDaftar Pustaka Dr. Tutty Ariani, SPDVliyaNo ratings yet
- Jeudy 2016Document22 pagesJeudy 2016Emirza Nur WicaksonoNo ratings yet