
3D Mapping Expert Consensus JoA
3D Mapping Expert Consensus JoA
You might also like
- Atlas of Cardiovascular Computed Tomography - Imaging Companion To Braunwald's Heart Disease, 1E (2010) (PDF) (UnitedVRG) PDFDocument270 pagesAtlas of Cardiovascular Computed Tomography - Imaging Companion To Braunwald's Heart Disease, 1E (2010) (PDF) (UnitedVRG) PDFboghezloredanaNo ratings yet
- Cardiac Imaging in Electrophysiology (PDFDrive)Document332 pagesCardiac Imaging in Electrophysiology (PDFDrive)aafagih100% (2)
- AHA ECG Database PDFDocument12 pagesAHA ECG Database PDFAllam Jaya PrakashNo ratings yet
- AbsorptionDocument39 pagesAbsorptionAlexânder De Paula Rodrigues100% (2)
- Chap 15 Indices Exponentials and Logarithms 2 PDFDocument27 pagesChap 15 Indices Exponentials and Logarithms 2 PDFArahNo ratings yet
- PDX-joa3 12606Document3 pagesPDX-joa3 12606PokéGoKidNo ratings yet
- Carto3 Fact SheetDocument3 pagesCarto3 Fact SheetVimal NishadNo ratings yet
- Manzke 2010Document13 pagesManzke 2010Boopathi RNo ratings yet
- CH 6.angioDocument20 pagesCH 6.angioKumail KhandwalaNo ratings yet
- Spect CTDocument41 pagesSpect CTJohn Paul MarasiganNo ratings yet
- Rita BDocument9 pagesRita Bpubliuscscipio236No ratings yet
- Saluja Et Al 2020 The Rapid Prediction of Focal Wavefront OriginsDocument10 pagesSaluja Et Al 2020 The Rapid Prediction of Focal Wavefront OriginsAndrés AllaucaNo ratings yet
- CT Support of Cardiac Structural Interventions: Review ArticleDocument12 pagesCT Support of Cardiac Structural Interventions: Review ArticlefibiaNo ratings yet
- CT Simulation MethodologyDocument41 pagesCT Simulation MethodologyRohla habibiNo ratings yet
- Raj2015, Arm Based Arrhythmia Beat MonitoringDocument8 pagesRaj2015, Arm Based Arrhythmia Beat Monitoringdharsandipan86No ratings yet
- Heart RhythmDocument5 pagesHeart RhythmPokéGoKidNo ratings yet
- 009 CT AdvancesDocument62 pages009 CT AdvancesSUSHILA GYAWALINo ratings yet
- Imagingofacutestroke: Current StateDocument9 pagesImagingofacutestroke: Current Statealejandro echeverriNo ratings yet
- Development of Artificial Atrium For Advancement of Catheterization SurgeriesDocument13 pagesDevelopment of Artificial Atrium For Advancement of Catheterization SurgeriesshmuelavshlmNo ratings yet
- Cardiovasc Electrophysiol - 2022 - Franco - Automatic Identification of Areas With Low Voltage Fragmented Electrograms ForDocument10 pagesCardiovasc Electrophysiol - 2022 - Franco - Automatic Identification of Areas With Low Voltage Fragmented Electrograms ForPaolo BerruquierNo ratings yet
- The Dyssynchronous Ventricle: Kian-Keong PohDocument33 pagesThe Dyssynchronous Ventricle: Kian-Keong PohcesareNo ratings yet
- Angiography of The Coronary ArteriesDocument14 pagesAngiography of The Coronary ArteriesYonatan Merchant PerezNo ratings yet
- TAC PeñascoDocument10 pagesTAC PeñascoJose ManuelNo ratings yet
- Retinal Blood Vessel Segmentation and Measurement of Vessel DiametersDocument6 pagesRetinal Blood Vessel Segmentation and Measurement of Vessel DiametersLekshmiNo ratings yet
- Pilani, K. K. Birla Goa Campus: Birla Institute of Technology & ScienceDocument8 pagesPilani, K. K. Birla Goa Campus: Birla Institute of Technology & Sciencedivyarai12345No ratings yet
- Cardiac Electrophysiology Without FluoroscopyFrom EverandCardiac Electrophysiology Without FluoroscopyRiccardo ProiettiNo ratings yet
- Art:10.1007/s11517 014 1165 7Document8 pagesArt:10.1007/s11517 014 1165 7Mustafa A. ElattarNo ratings yet
- CNN SkipDocument13 pagesCNN Skipjaviera.quirozNo ratings yet
- Design and Control of Motion Compensation Cardiac CathetersDocument7 pagesDesign and Control of Motion Compensation Cardiac CathetersmukhanNo ratings yet
- Dundamadappa, Multiphase CT AngiographyDocument7 pagesDundamadappa, Multiphase CT AngiographyririsNo ratings yet
- Deformable Cardiac Surface Tracking by Adaptive Estimation AlgorithmsDocument22 pagesDeformable Cardiac Surface Tracking by Adaptive Estimation AlgorithmssciCatNo ratings yet
- Heartrate MiniprojDocument4 pagesHeartrate MiniprojAravindanelangovanNo ratings yet
- How To: A Practical Guide To Cardiac Conduction Devices On Chest RadiographDocument7 pagesHow To: A Practical Guide To Cardiac Conduction Devices On Chest RadiographAndreea TeodorescuNo ratings yet
- Online Digital Filter and QRS Detector Applicable in Low Resource ECG Monitoring SystemsDocument11 pagesOnline Digital Filter and QRS Detector Applicable in Low Resource ECG Monitoring SystemsЈокић СтеванNo ratings yet
- A Computational Investigation Into Rate-Dependant VectorcardiogramDocument13 pagesA Computational Investigation Into Rate-Dependant VectorcardiogramsegurahNo ratings yet
- Exploiting Similar Prior Knowledge For Compressing ECG SignalsDocument13 pagesExploiting Similar Prior Knowledge For Compressing ECG SignalsNaser MovahhediniaNo ratings yet
- Clinical Application CTDocument40 pagesClinical Application CTWalaa MajeedNo ratings yet
- Perfusion Acv TacDocument7 pagesPerfusion Acv TacNicolás LozanoNo ratings yet
- Different Styles of IGRTDocument10 pagesDifferent Styles of IGRTPeter CaldwellNo ratings yet
- Resume C-ArmDocument4 pagesResume C-Armp27838121011No ratings yet
- Automatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsDocument23 pagesAutomatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsNishant UzirNo ratings yet
- Classifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationDocument9 pagesClassifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationIAES IJAINo ratings yet
- Research Article: An Adaptive and Time-Efficient ECG R-Peak Detection AlgorithmDocument15 pagesResearch Article: An Adaptive and Time-Efficient ECG R-Peak Detection AlgorithmAmelia Yulian SariNo ratings yet
- Cardiac Computed TomographyDocument29 pagesCardiac Computed TomographyAnu MavelyNo ratings yet
- Magnetocardiography Provides Non-Invasive Three-Dimensional Electroanatomical Imaging of Cardiac ElectrophysiologyDocument6 pagesMagnetocardiography Provides Non-Invasive Three-Dimensional Electroanatomical Imaging of Cardiac ElectrophysiologyAnca IftemieNo ratings yet
- Proceedings of Spie: Two Stage Registration-Based Automatic Left Ventricle Myocardium Segmentation of Cardiac 4DCT ImagesDocument9 pagesProceedings of Spie: Two Stage Registration-Based Automatic Left Ventricle Myocardium Segmentation of Cardiac 4DCT ImagesMdSalahUddinYusufNo ratings yet
- Biomedical Microsystems For Minimally Invasive Diagnosis and TreatmentDocument17 pagesBiomedical Microsystems For Minimally Invasive Diagnosis and TreatmentasifnewazuccNo ratings yet
- Ebook Fisica EletronsDocument27 pagesEbook Fisica EletronsBrena SouzaNo ratings yet
- Qyad 027Document13 pagesQyad 027alemed24No ratings yet
- Diagnoses SDocument25 pagesDiagnoses STudor DumitrascuNo ratings yet
- AngioNet A Convolutional Neural Network For VesselDocument14 pagesAngioNet A Convolutional Neural Network For VesselFederico WeckesserNo ratings yet
- VLSI Implementation of QRS Complex Detector Based On Wavelet DecompositionDocument11 pagesVLSI Implementation of QRS Complex Detector Based On Wavelet DecompositionVengababu VeturiNo ratings yet
- Articulo 5Document9 pagesArticulo 5grabacionesgoNo ratings yet
- Swapnil Poster Presentation 23 FinalDocument13 pagesSwapnil Poster Presentation 23 FinalFree Escort ServiceNo ratings yet
- Semantic ECG Interval Segmentation Using AutoencodersDocument7 pagesSemantic ECG Interval Segmentation Using AutoencodersMhd rdbNo ratings yet
- Multisensor Fusion For Atrial and Ventricular Activity Detection in Coronary Care MonitoringDocument5 pagesMultisensor Fusion For Atrial and Ventricular Activity Detection in Coronary Care Monitoringsufyan006No ratings yet
- Adult CTColonographyDocument16 pagesAdult CTColonographyrenatafisicamNo ratings yet
- Accepted Manuscript: Computer Methods and Programs in BiomedicineDocument31 pagesAccepted Manuscript: Computer Methods and Programs in Biomedicinearya segaraNo ratings yet
- Electrocardiogram (ECG) Pattern Modeling and Recognition Via Deterministic LearningDocument13 pagesElectrocardiogram (ECG) Pattern Modeling and Recognition Via Deterministic LearninglucashelalNo ratings yet
- 04b The ESC Textbook of Cardiovascular Imaging, 2nd Edition 2015 - Removed - RemovedDocument67 pages04b The ESC Textbook of Cardiovascular Imaging, 2nd Edition 2015 - Removed - RemovedLa Ode Muhammadin MatahanaNo ratings yet
- A Fast ECG Diagnosis by Using Non-Uniform Spectral AnalysisDocument21 pagesA Fast ECG Diagnosis by Using Non-Uniform Spectral AnalysisjyotiNo ratings yet
- CT GanjilDocument6 pagesCT Ganjilmuhammad erfansyahNo ratings yet
- Cardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIDocument30 pagesCardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIFikriYTNo ratings yet
- Lembar Informed Consent - PISCDocument3 pagesLembar Informed Consent - PISCFikriYTNo ratings yet
- Asianotik CHD Ahmad MuthiaDocument46 pagesAsianotik CHD Ahmad MuthiaFikriYTNo ratings yet
- Rido, Rudi - Peripheral Arterial and Venous DiseaseDocument87 pagesRido, Rudi - Peripheral Arterial and Venous DiseaseFikriYTNo ratings yet
- Edited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoDocument26 pagesEdited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoFikriYTNo ratings yet
- Primary and Secondary CV Prevention - Iman EvanDocument104 pagesPrimary and Secondary CV Prevention - Iman EvanFikriYTNo ratings yet
- Mike Fajri ECG Chamber Dilatation and HyperthorphyDocument27 pagesMike Fajri ECG Chamber Dilatation and HyperthorphyFikriYTNo ratings yet
- Anatomi Fisiologi Ahmad MuthiaDocument37 pagesAnatomi Fisiologi Ahmad MuthiaFikriYTNo ratings yet
- ACC Jimmy AsafDocument152 pagesACC Jimmy AsafFikriYTNo ratings yet
- Agustus Monitoring HemodinamikDocument61 pagesAgustus Monitoring HemodinamikFikriYTNo ratings yet
- Rido, Rudini - Paediatric ECGDocument51 pagesRido, Rudini - Paediatric ECGFikriYTNo ratings yet
- Rido, Rudini - Disease of Aorta and Trauma To The AortaDocument114 pagesRido, Rudini - Disease of Aorta and Trauma To The AortaFikriYTNo ratings yet
- Rido, Rudini - Rheumatic Heart DiseaseDocument23 pagesRido, Rudini - Rheumatic Heart DiseaseFikriYTNo ratings yet
- Anamnesis & PemfisDocument81 pagesAnamnesis & PemfisFikriYTNo ratings yet
- History Taking and PF CVD Iman Evan Final Fix - Dr. M Yusak SPJPDocument84 pagesHistory Taking and PF CVD Iman Evan Final Fix - Dr. M Yusak SPJPFikriYTNo ratings yet
- Pembekalan Auskultasi Jantung Jimmy AsafDocument45 pagesPembekalan Auskultasi Jantung Jimmy AsafFikriYTNo ratings yet
- Abstrak KilotoraksDocument1 pageAbstrak KilotoraksFikriYTNo ratings yet
- Atherosclerosis and Lipidology Juli 2021Document62 pagesAtherosclerosis and Lipidology Juli 2021FikriYTNo ratings yet
- Muthia-Ahmad Basic Cardiac ElectrophysiologyDocument53 pagesMuthia-Ahmad Basic Cardiac ElectrophysiologyFikriYTNo ratings yet
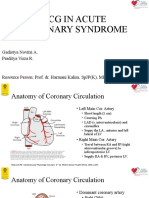
- ECG IN ACUTE CORONARY SYNDROME - Gadis Virza - Prof HarmaniDocument41 pagesECG IN ACUTE CORONARY SYNDROME - Gadis Virza - Prof HarmaniFikriYTNo ratings yet
- Evan-Iman - Exercise ECG - Stress Test FINALDocument73 pagesEvan-Iman - Exercise ECG - Stress Test FINALFikriYTNo ratings yet
- Basic Echo and DopplerDocument20 pagesBasic Echo and DopplerFikriYTNo ratings yet
- Slide Technical MeetingDocument14 pagesSlide Technical MeetingFikriYTNo ratings yet
- Lightolier Lytespan Track Lighting Systems Catalog 1984Document94 pagesLightolier Lytespan Track Lighting Systems Catalog 1984Alan Masters100% (1)
- Frequently Used Terms in Vedic AstrologyDocument3 pagesFrequently Used Terms in Vedic AstrologyNarayana Remala100% (1)
- Datasheet LTH-1550-01Document4 pagesDatasheet LTH-1550-01AntonellaBogadoNo ratings yet
- Allowable Stress Design of Concrete Masonry PilastersDocument7 pagesAllowable Stress Design of Concrete Masonry PilastersReinaldo Andrei SalazarNo ratings yet
- CYWGDocument19 pagesCYWGGerry EscañoNo ratings yet
- Why Use Preheat and Post Weld Heat Treatments Brochure PDFDocument2 pagesWhy Use Preheat and Post Weld Heat Treatments Brochure PDFErick HoganNo ratings yet
- Case Study On Development of Process Failure Mode Effect Analysis (PFMEA) - Issues and RecommendationsDocument8 pagesCase Study On Development of Process Failure Mode Effect Analysis (PFMEA) - Issues and RecommendationsSang BùiNo ratings yet
- Numerical Analysis of A Bisection-Exclusion Method To Find Zeros of Univariate Analytic FunctionsDocument39 pagesNumerical Analysis of A Bisection-Exclusion Method To Find Zeros of Univariate Analytic FunctionsLucas SantosNo ratings yet
- The Elephant and FriendsDocument2 pagesThe Elephant and FriendsENGLISHCLASS SMKN1SRKNo ratings yet
- AccurioLabel 400 - Basic - Demo - Script - v1.0 - EDocument33 pagesAccurioLabel 400 - Basic - Demo - Script - v1.0 - EDiego LanderosNo ratings yet
- Floor 76: Sword Art Online: Infinity Moment - Guide (Uncompleted)Document30 pagesFloor 76: Sword Art Online: Infinity Moment - Guide (Uncompleted)Sony Kasujaya100% (1)
- Metrology CH 3Document52 pagesMetrology CH 3Eng Islam Kamal ElDin100% (1)
- OTS Optical Tool Setter: Installation GuideDocument52 pagesOTS Optical Tool Setter: Installation GuideIrina BesliuNo ratings yet
- C10 CBSEPhy QueDocument4 pagesC10 CBSEPhy QueGeneric nameNo ratings yet
- Sweet Corn and Cheese Samoosa - Google SearchDocument2 pagesSweet Corn and Cheese Samoosa - Google SearchmisslxmasherNo ratings yet
- The Effect of Elevated Temperature On ConcreteDocument204 pagesThe Effect of Elevated Temperature On Concretexaaabbb_550464353100% (1)
- Programmable 3 Channel Power Supply 526Document2 pagesProgrammable 3 Channel Power Supply 526digiarkanandNo ratings yet
- 23-Primary Treatment and Secondary Treatment-21!02!2023Document37 pages23-Primary Treatment and Secondary Treatment-21!02!2023Back upNo ratings yet
- Energy Challenges in SomaliaDocument14 pagesEnergy Challenges in SomaliaLiban Abdullahi AliNo ratings yet
- Suld United PPT2020.09Document31 pagesSuld United PPT2020.09Ulstuguldur Kh.No ratings yet
- 36 - 4 - New York - 08-91 - 1478Document8 pages36 - 4 - New York - 08-91 - 1478Ovo OjasNo ratings yet
- NDT Tests On Concrete: G Rebound Tests G Pull-Out Tests G Dynamic Tests G Radioactive Methods G Maturity ConceptDocument7 pagesNDT Tests On Concrete: G Rebound Tests G Pull-Out Tests G Dynamic Tests G Radioactive Methods G Maturity ConceptBarun KarNo ratings yet
- Far Trek Continue VoyagesDocument148 pagesFar Trek Continue Voyageswintermute57100% (2)
- Pub - Vectors Matrices and Geometry PDFDocument357 pagesPub - Vectors Matrices and Geometry PDFSalami Blessing100% (1)
- Stewart Revofalg ExercisesDocument12 pagesStewart Revofalg Exercisesapi-261282952No ratings yet
- SWP 04 Lifting OperationDocument4 pagesSWP 04 Lifting Operationমমিন মানবNo ratings yet
- Mens TshirtDocument15 pagesMens TshirtTrung Hieu NguyenNo ratings yet
- The Baldur's Gate Series 2 - Shadows of AmnDocument99 pagesThe Baldur's Gate Series 2 - Shadows of AmnJustin Moore100% (1)















































































































Download as pptx, pdf, or txt
You might also like
- Atlas of Cardiovascular Computed Tomography - Imaging Companion To Braunwald's Heart Disease, 1E (2010) (PDF) (UnitedVRG) PDFDocument270 pagesAtlas of Cardiovascular Computed Tomography - Imaging Companion To Braunwald's Heart Disease, 1E (2010) (PDF) (UnitedVRG) PDFboghezloredanaNo ratings yet
- Cardiac Imaging in Electrophysiology (PDFDrive)Document332 pagesCardiac Imaging in Electrophysiology (PDFDrive)aafagih100% (2)
- AHA ECG Database PDFDocument12 pagesAHA ECG Database PDFAllam Jaya PrakashNo ratings yet
- AbsorptionDocument39 pagesAbsorptionAlexânder De Paula Rodrigues100% (2)
- Chap 15 Indices Exponentials and Logarithms 2 PDFDocument27 pagesChap 15 Indices Exponentials and Logarithms 2 PDFArahNo ratings yet
- PDX-joa3 12606Document3 pagesPDX-joa3 12606PokéGoKidNo ratings yet
- Carto3 Fact SheetDocument3 pagesCarto3 Fact SheetVimal NishadNo ratings yet
- Manzke 2010Document13 pagesManzke 2010Boopathi RNo ratings yet
- CH 6.angioDocument20 pagesCH 6.angioKumail KhandwalaNo ratings yet
- Spect CTDocument41 pagesSpect CTJohn Paul MarasiganNo ratings yet
- Rita BDocument9 pagesRita Bpubliuscscipio236No ratings yet
- Saluja Et Al 2020 The Rapid Prediction of Focal Wavefront OriginsDocument10 pagesSaluja Et Al 2020 The Rapid Prediction of Focal Wavefront OriginsAndrés AllaucaNo ratings yet
- CT Support of Cardiac Structural Interventions: Review ArticleDocument12 pagesCT Support of Cardiac Structural Interventions: Review ArticlefibiaNo ratings yet
- CT Simulation MethodologyDocument41 pagesCT Simulation MethodologyRohla habibiNo ratings yet
- Raj2015, Arm Based Arrhythmia Beat MonitoringDocument8 pagesRaj2015, Arm Based Arrhythmia Beat Monitoringdharsandipan86No ratings yet
- Heart RhythmDocument5 pagesHeart RhythmPokéGoKidNo ratings yet
- 009 CT AdvancesDocument62 pages009 CT AdvancesSUSHILA GYAWALINo ratings yet
- Imagingofacutestroke: Current StateDocument9 pagesImagingofacutestroke: Current Statealejandro echeverriNo ratings yet
- Development of Artificial Atrium For Advancement of Catheterization SurgeriesDocument13 pagesDevelopment of Artificial Atrium For Advancement of Catheterization SurgeriesshmuelavshlmNo ratings yet
- Cardiovasc Electrophysiol - 2022 - Franco - Automatic Identification of Areas With Low Voltage Fragmented Electrograms ForDocument10 pagesCardiovasc Electrophysiol - 2022 - Franco - Automatic Identification of Areas With Low Voltage Fragmented Electrograms ForPaolo BerruquierNo ratings yet
- The Dyssynchronous Ventricle: Kian-Keong PohDocument33 pagesThe Dyssynchronous Ventricle: Kian-Keong PohcesareNo ratings yet
- Angiography of The Coronary ArteriesDocument14 pagesAngiography of The Coronary ArteriesYonatan Merchant PerezNo ratings yet
- TAC PeñascoDocument10 pagesTAC PeñascoJose ManuelNo ratings yet
- Retinal Blood Vessel Segmentation and Measurement of Vessel DiametersDocument6 pagesRetinal Blood Vessel Segmentation and Measurement of Vessel DiametersLekshmiNo ratings yet
- Pilani, K. K. Birla Goa Campus: Birla Institute of Technology & ScienceDocument8 pagesPilani, K. K. Birla Goa Campus: Birla Institute of Technology & Sciencedivyarai12345No ratings yet
- Cardiac Electrophysiology Without FluoroscopyFrom EverandCardiac Electrophysiology Without FluoroscopyRiccardo ProiettiNo ratings yet
- Art:10.1007/s11517 014 1165 7Document8 pagesArt:10.1007/s11517 014 1165 7Mustafa A. ElattarNo ratings yet
- CNN SkipDocument13 pagesCNN Skipjaviera.quirozNo ratings yet
- Design and Control of Motion Compensation Cardiac CathetersDocument7 pagesDesign and Control of Motion Compensation Cardiac CathetersmukhanNo ratings yet
- Dundamadappa, Multiphase CT AngiographyDocument7 pagesDundamadappa, Multiphase CT AngiographyririsNo ratings yet
- Deformable Cardiac Surface Tracking by Adaptive Estimation AlgorithmsDocument22 pagesDeformable Cardiac Surface Tracking by Adaptive Estimation AlgorithmssciCatNo ratings yet
- Heartrate MiniprojDocument4 pagesHeartrate MiniprojAravindanelangovanNo ratings yet
- How To: A Practical Guide To Cardiac Conduction Devices On Chest RadiographDocument7 pagesHow To: A Practical Guide To Cardiac Conduction Devices On Chest RadiographAndreea TeodorescuNo ratings yet
- Online Digital Filter and QRS Detector Applicable in Low Resource ECG Monitoring SystemsDocument11 pagesOnline Digital Filter and QRS Detector Applicable in Low Resource ECG Monitoring SystemsЈокић СтеванNo ratings yet
- A Computational Investigation Into Rate-Dependant VectorcardiogramDocument13 pagesA Computational Investigation Into Rate-Dependant VectorcardiogramsegurahNo ratings yet
- Exploiting Similar Prior Knowledge For Compressing ECG SignalsDocument13 pagesExploiting Similar Prior Knowledge For Compressing ECG SignalsNaser MovahhediniaNo ratings yet
- Clinical Application CTDocument40 pagesClinical Application CTWalaa MajeedNo ratings yet
- Perfusion Acv TacDocument7 pagesPerfusion Acv TacNicolás LozanoNo ratings yet
- Different Styles of IGRTDocument10 pagesDifferent Styles of IGRTPeter CaldwellNo ratings yet
- Resume C-ArmDocument4 pagesResume C-Armp27838121011No ratings yet
- Automatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsDocument23 pagesAutomatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsNishant UzirNo ratings yet
- Classifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationDocument9 pagesClassifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationIAES IJAINo ratings yet
- Research Article: An Adaptive and Time-Efficient ECG R-Peak Detection AlgorithmDocument15 pagesResearch Article: An Adaptive and Time-Efficient ECG R-Peak Detection AlgorithmAmelia Yulian SariNo ratings yet
- Cardiac Computed TomographyDocument29 pagesCardiac Computed TomographyAnu MavelyNo ratings yet
- Magnetocardiography Provides Non-Invasive Three-Dimensional Electroanatomical Imaging of Cardiac ElectrophysiologyDocument6 pagesMagnetocardiography Provides Non-Invasive Three-Dimensional Electroanatomical Imaging of Cardiac ElectrophysiologyAnca IftemieNo ratings yet
- Proceedings of Spie: Two Stage Registration-Based Automatic Left Ventricle Myocardium Segmentation of Cardiac 4DCT ImagesDocument9 pagesProceedings of Spie: Two Stage Registration-Based Automatic Left Ventricle Myocardium Segmentation of Cardiac 4DCT ImagesMdSalahUddinYusufNo ratings yet
- Biomedical Microsystems For Minimally Invasive Diagnosis and TreatmentDocument17 pagesBiomedical Microsystems For Minimally Invasive Diagnosis and TreatmentasifnewazuccNo ratings yet
- Ebook Fisica EletronsDocument27 pagesEbook Fisica EletronsBrena SouzaNo ratings yet
- Qyad 027Document13 pagesQyad 027alemed24No ratings yet
- Diagnoses SDocument25 pagesDiagnoses STudor DumitrascuNo ratings yet
- AngioNet A Convolutional Neural Network For VesselDocument14 pagesAngioNet A Convolutional Neural Network For VesselFederico WeckesserNo ratings yet
- VLSI Implementation of QRS Complex Detector Based On Wavelet DecompositionDocument11 pagesVLSI Implementation of QRS Complex Detector Based On Wavelet DecompositionVengababu VeturiNo ratings yet
- Articulo 5Document9 pagesArticulo 5grabacionesgoNo ratings yet
- Swapnil Poster Presentation 23 FinalDocument13 pagesSwapnil Poster Presentation 23 FinalFree Escort ServiceNo ratings yet
- Semantic ECG Interval Segmentation Using AutoencodersDocument7 pagesSemantic ECG Interval Segmentation Using AutoencodersMhd rdbNo ratings yet
- Multisensor Fusion For Atrial and Ventricular Activity Detection in Coronary Care MonitoringDocument5 pagesMultisensor Fusion For Atrial and Ventricular Activity Detection in Coronary Care Monitoringsufyan006No ratings yet
- Adult CTColonographyDocument16 pagesAdult CTColonographyrenatafisicamNo ratings yet
- Accepted Manuscript: Computer Methods and Programs in BiomedicineDocument31 pagesAccepted Manuscript: Computer Methods and Programs in Biomedicinearya segaraNo ratings yet
- Electrocardiogram (ECG) Pattern Modeling and Recognition Via Deterministic LearningDocument13 pagesElectrocardiogram (ECG) Pattern Modeling and Recognition Via Deterministic LearninglucashelalNo ratings yet
- 04b The ESC Textbook of Cardiovascular Imaging, 2nd Edition 2015 - Removed - RemovedDocument67 pages04b The ESC Textbook of Cardiovascular Imaging, 2nd Edition 2015 - Removed - RemovedLa Ode Muhammadin MatahanaNo ratings yet
- A Fast ECG Diagnosis by Using Non-Uniform Spectral AnalysisDocument21 pagesA Fast ECG Diagnosis by Using Non-Uniform Spectral AnalysisjyotiNo ratings yet
- CT GanjilDocument6 pagesCT Ganjilmuhammad erfansyahNo ratings yet
- Cardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIDocument30 pagesCardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIFikriYTNo ratings yet
- Lembar Informed Consent - PISCDocument3 pagesLembar Informed Consent - PISCFikriYTNo ratings yet
- Asianotik CHD Ahmad MuthiaDocument46 pagesAsianotik CHD Ahmad MuthiaFikriYTNo ratings yet
- Rido, Rudi - Peripheral Arterial and Venous DiseaseDocument87 pagesRido, Rudi - Peripheral Arterial and Venous DiseaseFikriYTNo ratings yet
- Edited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoDocument26 pagesEdited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoFikriYTNo ratings yet
- Primary and Secondary CV Prevention - Iman EvanDocument104 pagesPrimary and Secondary CV Prevention - Iman EvanFikriYTNo ratings yet
- Mike Fajri ECG Chamber Dilatation and HyperthorphyDocument27 pagesMike Fajri ECG Chamber Dilatation and HyperthorphyFikriYTNo ratings yet
- Anatomi Fisiologi Ahmad MuthiaDocument37 pagesAnatomi Fisiologi Ahmad MuthiaFikriYTNo ratings yet
- ACC Jimmy AsafDocument152 pagesACC Jimmy AsafFikriYTNo ratings yet
- Agustus Monitoring HemodinamikDocument61 pagesAgustus Monitoring HemodinamikFikriYTNo ratings yet
- Rido, Rudini - Paediatric ECGDocument51 pagesRido, Rudini - Paediatric ECGFikriYTNo ratings yet
- Rido, Rudini - Disease of Aorta and Trauma To The AortaDocument114 pagesRido, Rudini - Disease of Aorta and Trauma To The AortaFikriYTNo ratings yet
- Rido, Rudini - Rheumatic Heart DiseaseDocument23 pagesRido, Rudini - Rheumatic Heart DiseaseFikriYTNo ratings yet
- Anamnesis & PemfisDocument81 pagesAnamnesis & PemfisFikriYTNo ratings yet
- History Taking and PF CVD Iman Evan Final Fix - Dr. M Yusak SPJPDocument84 pagesHistory Taking and PF CVD Iman Evan Final Fix - Dr. M Yusak SPJPFikriYTNo ratings yet
- Pembekalan Auskultasi Jantung Jimmy AsafDocument45 pagesPembekalan Auskultasi Jantung Jimmy AsafFikriYTNo ratings yet
- Abstrak KilotoraksDocument1 pageAbstrak KilotoraksFikriYTNo ratings yet
- Atherosclerosis and Lipidology Juli 2021Document62 pagesAtherosclerosis and Lipidology Juli 2021FikriYTNo ratings yet
- Muthia-Ahmad Basic Cardiac ElectrophysiologyDocument53 pagesMuthia-Ahmad Basic Cardiac ElectrophysiologyFikriYTNo ratings yet
- ECG IN ACUTE CORONARY SYNDROME - Gadis Virza - Prof HarmaniDocument41 pagesECG IN ACUTE CORONARY SYNDROME - Gadis Virza - Prof HarmaniFikriYTNo ratings yet
- Evan-Iman - Exercise ECG - Stress Test FINALDocument73 pagesEvan-Iman - Exercise ECG - Stress Test FINALFikriYTNo ratings yet
- Basic Echo and DopplerDocument20 pagesBasic Echo and DopplerFikriYTNo ratings yet
- Slide Technical MeetingDocument14 pagesSlide Technical MeetingFikriYTNo ratings yet
- Lightolier Lytespan Track Lighting Systems Catalog 1984Document94 pagesLightolier Lytespan Track Lighting Systems Catalog 1984Alan Masters100% (1)
- Frequently Used Terms in Vedic AstrologyDocument3 pagesFrequently Used Terms in Vedic AstrologyNarayana Remala100% (1)
- Datasheet LTH-1550-01Document4 pagesDatasheet LTH-1550-01AntonellaBogadoNo ratings yet
- Allowable Stress Design of Concrete Masonry PilastersDocument7 pagesAllowable Stress Design of Concrete Masonry PilastersReinaldo Andrei SalazarNo ratings yet
- CYWGDocument19 pagesCYWGGerry EscañoNo ratings yet
- Why Use Preheat and Post Weld Heat Treatments Brochure PDFDocument2 pagesWhy Use Preheat and Post Weld Heat Treatments Brochure PDFErick HoganNo ratings yet
- Case Study On Development of Process Failure Mode Effect Analysis (PFMEA) - Issues and RecommendationsDocument8 pagesCase Study On Development of Process Failure Mode Effect Analysis (PFMEA) - Issues and RecommendationsSang BùiNo ratings yet
- Numerical Analysis of A Bisection-Exclusion Method To Find Zeros of Univariate Analytic FunctionsDocument39 pagesNumerical Analysis of A Bisection-Exclusion Method To Find Zeros of Univariate Analytic FunctionsLucas SantosNo ratings yet
- The Elephant and FriendsDocument2 pagesThe Elephant and FriendsENGLISHCLASS SMKN1SRKNo ratings yet
- AccurioLabel 400 - Basic - Demo - Script - v1.0 - EDocument33 pagesAccurioLabel 400 - Basic - Demo - Script - v1.0 - EDiego LanderosNo ratings yet
- Floor 76: Sword Art Online: Infinity Moment - Guide (Uncompleted)Document30 pagesFloor 76: Sword Art Online: Infinity Moment - Guide (Uncompleted)Sony Kasujaya100% (1)
- Metrology CH 3Document52 pagesMetrology CH 3Eng Islam Kamal ElDin100% (1)
- OTS Optical Tool Setter: Installation GuideDocument52 pagesOTS Optical Tool Setter: Installation GuideIrina BesliuNo ratings yet
- C10 CBSEPhy QueDocument4 pagesC10 CBSEPhy QueGeneric nameNo ratings yet
- Sweet Corn and Cheese Samoosa - Google SearchDocument2 pagesSweet Corn and Cheese Samoosa - Google SearchmisslxmasherNo ratings yet
- The Effect of Elevated Temperature On ConcreteDocument204 pagesThe Effect of Elevated Temperature On Concretexaaabbb_550464353100% (1)
- Programmable 3 Channel Power Supply 526Document2 pagesProgrammable 3 Channel Power Supply 526digiarkanandNo ratings yet
- 23-Primary Treatment and Secondary Treatment-21!02!2023Document37 pages23-Primary Treatment and Secondary Treatment-21!02!2023Back upNo ratings yet
- Energy Challenges in SomaliaDocument14 pagesEnergy Challenges in SomaliaLiban Abdullahi AliNo ratings yet
- Suld United PPT2020.09Document31 pagesSuld United PPT2020.09Ulstuguldur Kh.No ratings yet
- 36 - 4 - New York - 08-91 - 1478Document8 pages36 - 4 - New York - 08-91 - 1478Ovo OjasNo ratings yet
- NDT Tests On Concrete: G Rebound Tests G Pull-Out Tests G Dynamic Tests G Radioactive Methods G Maturity ConceptDocument7 pagesNDT Tests On Concrete: G Rebound Tests G Pull-Out Tests G Dynamic Tests G Radioactive Methods G Maturity ConceptBarun KarNo ratings yet
- Far Trek Continue VoyagesDocument148 pagesFar Trek Continue Voyageswintermute57100% (2)
- Pub - Vectors Matrices and Geometry PDFDocument357 pagesPub - Vectors Matrices and Geometry PDFSalami Blessing100% (1)
- Stewart Revofalg ExercisesDocument12 pagesStewart Revofalg Exercisesapi-261282952No ratings yet
- SWP 04 Lifting OperationDocument4 pagesSWP 04 Lifting Operationমমিন মানবNo ratings yet
- Mens TshirtDocument15 pagesMens TshirtTrung Hieu NguyenNo ratings yet
- The Baldur's Gate Series 2 - Shadows of AmnDocument99 pagesThe Baldur's Gate Series 2 - Shadows of AmnJustin Moore100% (1)