
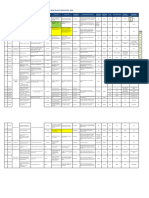
Non-Conformances / Document Control: Draakhine Chemical Pathology Nhls Tygerberg Lab Management Workshop June 4-6 2019
Non-Conformances / Document Control: Draakhine Chemical Pathology Nhls Tygerberg Lab Management Workshop June 4-6 2019
You might also like
- CBC Absolute Count Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageCBC Absolute Count Test Report Format Example Sample Template Drlogy Lab ReportThota charanNo ratings yet
- Contoh Format DriftDocument12 pagesContoh Format DriftGenevy KarminNo ratings yet
- Nursing Care Plan For DysmenorrheaDocument3 pagesNursing Care Plan For DysmenorrheaMarife Lipana Reyes73% (22)
- Program For Calibration, Preventive Maintenance Final PDFDocument28 pagesProgram For Calibration, Preventive Maintenance Final PDFMatthew Pacardo100% (1)
- Lesson-09 MODUL PDFDocument9 pagesLesson-09 MODUL PDFanggaririn100% (1)
- Bone Marrow Aspirate and BiopsyDocument3 pagesBone Marrow Aspirate and BiopsyatikaNo ratings yet
- Step 2 Clinical Skills (CS) : Content Description and General InformationDocument20 pagesStep 2 Clinical Skills (CS) : Content Description and General Informationdr322No ratings yet
- 2019 Registration FormDocument3 pages2019 Registration FormJoanne Jaramilla Dollente33% (3)
- Histopathology COP 09153 1.0Document15 pagesHistopathology COP 09153 1.0Dr sumithra ravi100% (1)
- Physical and Chemical Properties of UrinalysisDocument39 pagesPhysical and Chemical Properties of UrinalysisDOLORES LIZANo ratings yet
- Allowable Imprecisionfor Laboratory Tests Based On Clinical and Analytical TestDocument6 pagesAllowable Imprecisionfor Laboratory Tests Based On Clinical and Analytical Testsidomoyo100% (1)
- BX 3010 (0C)Document362 pagesBX 3010 (0C)Lâm Hồ Ngọc HãnNo ratings yet
- QualityindicatorsDocument8 pagesQualityindicatorsMishalni PotterNo ratings yet
- QA03005 Critical Testand Critical Result ReportingDocument7 pagesQA03005 Critical Testand Critical Result Reportingdebbie o. azcunaNo ratings yet
- Do 2020-0820Document8 pagesDo 2020-0820wyneth navesisNo ratings yet
- Biosafety in Microbiological and Biomedical Laboratory, 4th Edition (U.S. Department of Health)Document270 pagesBiosafety in Microbiological and Biomedical Laboratory, 4th Edition (U.S. Department of Health)Marlene TapiaNo ratings yet
- Mindray BS 3600 Laboratory Preventive MaintenanceDocument1 pageMindray BS 3600 Laboratory Preventive MaintenanceCaesar A. AlesnaNo ratings yet
- F D A O R A: ORA Laboratory Manual Volume IDocument3 pagesF D A O R A: ORA Laboratory Manual Volume IvictorNo ratings yet
- CHAPTER 8 MedtechDocument17 pagesCHAPTER 8 MedtechKisen DiazNo ratings yet
- 7.CCLM 2018 WG BV HarmonisationDocument8 pages7.CCLM 2018 WG BV HarmonisationJulián Mesa SierraNo ratings yet
- QA QC Clinical MicrosDocument14 pagesQA QC Clinical MicrosKristel S. BalismonNo ratings yet
- Master Health CheckupDocument8 pagesMaster Health CheckupstephenvedhamalarNo ratings yet
- Lab Med Quality IndicatorsDocument15 pagesLab Med Quality IndicatorsMelani Sinasri RenagupitaNo ratings yet
- CA Series Measurement Evaluation and Check MethodsDocument34 pagesCA Series Measurement Evaluation and Check MethodsmarianalinamihaelaNo ratings yet
- Liquid Wastes Proper DisposalDocument2 pagesLiquid Wastes Proper DisposalCaesar A. AlesnaNo ratings yet
- Quality Assurance For Veterinary In-Clinic LaboratoriesDocument29 pagesQuality Assurance For Veterinary In-Clinic Laboratoriesvitalab llanograndeNo ratings yet
- CALIBRATION REPORT (Hema)Document1 pageCALIBRATION REPORT (Hema)jef1234321No ratings yet
- Lab Math Lec (Prelims)Document7 pagesLab Math Lec (Prelims)Merra VenzuelaNo ratings yet
- Manual For Procurement of Diagnostics-001-June2013Document34 pagesManual For Procurement of Diagnostics-001-June2013Jose MirandaNo ratings yet
- TAT AnalysisDocument5 pagesTAT AnalysisSrinivas PolikepatiNo ratings yet
- Primary Sample Collection Manual GD-QSPMDocument51 pagesPrimary Sample Collection Manual GD-QSPMLalit Surykant Chavan100% (1)
- Uncontrolled When PrintedDocument54 pagesUncontrolled When PrintedAmal HaririNo ratings yet
- Empowering Breakthroughs: Science and Lab SolutionsDocument1,182 pagesEmpowering Breakthroughs: Science and Lab Solutionsmoparthi rajeshNo ratings yet
- Quality Control Management in Labortory Services.Document54 pagesQuality Control Management in Labortory Services.Bakhtawar Siddique MemonNo ratings yet
- Nnaca Sop 302Document6 pagesNnaca Sop 302Thusitha LakpriyaNo ratings yet
- Non-Protein Nitrogen Compounds1 (FINALS)Document60 pagesNon-Protein Nitrogen Compounds1 (FINALS)Marydith Ortillo100% (1)
- Wasserlab Brochure Autwomatic Plus 1+2Document10 pagesWasserlab Brochure Autwomatic Plus 1+2Lloid LauretaNo ratings yet
- Critical Value in HematologyDocument8 pagesCritical Value in HematologySTARK DIAGNOSTICSNo ratings yet
- Flow Cytometry Immunophenotyping For Hematologic NeoplasmsDocument28 pagesFlow Cytometry Immunophenotyping For Hematologic NeoplasmsAti Rahmi PurwandariNo ratings yet
- Changes Blood Transfusion Consent AlgorithmDocument1 pageChanges Blood Transfusion Consent AlgorithmLawrence GamboaNo ratings yet
- Sigma Metric QMS in Medical Lab - Palembang IndonesiaDocument76 pagesSigma Metric QMS in Medical Lab - Palembang Indonesiabudi darmanta100% (1)
- ENG-01-F02 Calibration Report Ver.02 20190329 XP-100 S.N B1554 in RSUD Anshari Saleh BanjarmasinDocument4 pagesENG-01-F02 Calibration Report Ver.02 20190329 XP-100 S.N B1554 in RSUD Anshari Saleh BanjarmasinLaboratorium Ansari Saleh100% (1)
- IFCC PPT, July 2017 - Control of Lab Error Through CAPADocument15 pagesIFCC PPT, July 2017 - Control of Lab Error Through CAPAAbdul KalimNo ratings yet
- Drug Testing Consent FormDocument4 pagesDrug Testing Consent FormJeffrey LunaNo ratings yet
- Linearity of Calibration Curves For Analytical MethodsDocument21 pagesLinearity of Calibration Curves For Analytical MethodsAna Carolina SantosNo ratings yet
- The EFLM Update of The European Urinalysis GuidelinesDocument16 pagesThe EFLM Update of The European Urinalysis GuidelinesGawri AbeyNo ratings yet
- Standard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Document17 pagesStandard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Aniruddha ChatterjeeNo ratings yet
- NCM 120J Handout # 1: 2.decent Work Is Employment That "Document10 pagesNCM 120J Handout # 1: 2.decent Work Is Employment That "Nur Fatima SanaaniNo ratings yet
- Lesson 7 QUALITY SYSTEMS MANAGEMENTDocument34 pagesLesson 7 QUALITY SYSTEMS MANAGEMENTMika De VeraNo ratings yet
- A Model For Reducing Medical ErrorsDocument4 pagesA Model For Reducing Medical ErrorsPinto PintoNo ratings yet
- A Handbook On Covid-19 Testing F1Document27 pagesA Handbook On Covid-19 Testing F1Sumesh Shreekhanda ShresthaNo ratings yet
- Retention Times For Records, Reports, and SpecimensDocument1 pageRetention Times For Records, Reports, and SpecimensDayledaniel SorvetoNo ratings yet
- 11 Key Areas Evaluation ToolDocument10 pages11 Key Areas Evaluation Toolpinoybsn26No ratings yet
- Haematology Diagnosis-Army USADocument205 pagesHaematology Diagnosis-Army USAManuela BotisNo ratings yet
- IH Hospital Wide QI Master Spreadsheet 2023Document115 pagesIH Hospital Wide QI Master Spreadsheet 2023Uranchimeg MyagmarchimedNo ratings yet
- A02a00004aen Yumizen G APTT PDFDocument2 pagesA02a00004aen Yumizen G APTT PDFNAKANWAGI JOSLYLINENo ratings yet
- Supportive Supervision Tool For COVID - After Review With Lab Heads PDFDocument10 pagesSupportive Supervision Tool For COVID - After Review With Lab Heads PDFNzema NgakanaNo ratings yet
- 8.7 Nonconforming Outputs: Previous NextDocument10 pages8.7 Nonconforming Outputs: Previous Nextgayathrisrk001No ratings yet
- Assessment ToolDocument13 pagesAssessment Toolal gulNo ratings yet
- Corrective & Preventive ActionDocument2 pagesCorrective & Preventive ActionStephen Lim Kean JinNo ratings yet
- Corrective ActionsDocument3 pagesCorrective Actionsasderbva100% (1)
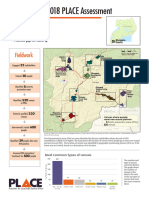
- Ntungamo: 2018 PLACE Assessment: PL CEDocument4 pagesNtungamo: 2018 PLACE Assessment: PL CEJulius MuhimboNo ratings yet
- Procurement Advert 1 22-23Document1 pageProcurement Advert 1 22-23Julius MuhimboNo ratings yet
- Ims Policy - Integrated Management System: Ergy For The WDocument4 pagesIms Policy - Integrated Management System: Ergy For The WJulius MuhimboNo ratings yet
- Type23 NR2Document16 pagesType23 NR2Julius MuhimboNo ratings yet
- UNBS CertificatesDocument1 pageUNBS CertificatesJulius MuhimboNo ratings yet
- Form - CAR FormDocument6 pagesForm - CAR FormJulius MuhimboNo ratings yet
- Fair Enough PDFDocument6 pagesFair Enough PDFJulius MuhimboNo ratings yet
- 71bd00 Betopan Brosur TRDocument2 pages71bd00 Betopan Brosur TRJulius MuhimboNo ratings yet
- SPD Solar Flood Lights SpecificationsDocument1 pageSPD Solar Flood Lights SpecificationsJulius MuhimboNo ratings yet
- Comformity Certificate NewDocument4 pagesComformity Certificate NewJulius MuhimboNo ratings yet
- Test Report For 2core Flex Cable 14 11 2022Document3 pagesTest Report For 2core Flex Cable 14 11 2022Julius MuhimboNo ratings yet
- Solcourse Polythene DPM V005 TDSDocument3 pagesSolcourse Polythene DPM V005 TDSJulius MuhimboNo ratings yet
- TDS - Technical Data SheetsDocument1 pageTDS - Technical Data SheetsJulius MuhimboNo ratings yet
- JPL Haccp Plan (2) (Repaired)Document13 pagesJPL Haccp Plan (2) (Repaired)Julius MuhimboNo ratings yet
- Rose FoamDocument4 pagesRose FoamJulius MuhimboNo ratings yet
- Material Safety Data Sheet: Wet Chemical Dry Charge (Portable Fire Extinguisher Agent)Document6 pagesMaterial Safety Data Sheet: Wet Chemical Dry Charge (Portable Fire Extinguisher Agent)Julius MuhimboNo ratings yet
- Sika Monotop 610 MsdsDocument14 pagesSika Monotop 610 MsdsJulius MuhimboNo ratings yet
- Newterra Quality Plan - Uganda WWTP - PWTPDocument1 pageNewterra Quality Plan - Uganda WWTP - PWTPJulius MuhimboNo ratings yet
- MSDS - Smoke Detector Test SprayDocument15 pagesMSDS - Smoke Detector Test SprayJulius MuhimboNo ratings yet
- GWC24AGDXE-K3DNA1A - Spec SheetDocument5 pagesGWC24AGDXE-K3DNA1A - Spec SheetJulius MuhimboNo ratings yet
- Anchor Bolt Detail 1Document1 pageAnchor Bolt Detail 1Julius MuhimboNo ratings yet
- EM14WMCBULK - Emmergency Light Data SheetDocument1 pageEM14WMCBULK - Emmergency Light Data SheetJulius MuhimboNo ratings yet
- Tusher Center Working Paper 7Document46 pagesTusher Center Working Paper 7Julius MuhimboNo ratings yet
- 01 35 16 Alteration Project ProceduresDocument8 pages01 35 16 Alteration Project ProceduresJulius MuhimboNo ratings yet
- This Certificate of Compliance Validates The FollowingDocument6 pagesThis Certificate of Compliance Validates The FollowingJulius MuhimboNo ratings yet
- SF01 Food Application Form With All AnnexesDocument11 pagesSF01 Food Application Form With All AnnexesJulius MuhimboNo ratings yet
- Talacogon - 4th Quarter PresentationDocument48 pagesTalacogon - 4th Quarter PresentationRomeo AbrigoNo ratings yet
- Rapport M1-M2Document2 pagesRapport M1-M2LedouxNo ratings yet
- Health Education ProcessDocument25 pagesHealth Education Processdailygrind00011No ratings yet
- Sop For Bio-BurdenDocument5 pagesSop For Bio-BurdenMusyoka Urbanus100% (1)
- SWMS Sample - Safe Work MethodDocument8 pagesSWMS Sample - Safe Work Methodsupasart100% (1)
- JOGNN Guidelines For AuthorsDocument3 pagesJOGNN Guidelines For AuthorsPrathibha Lydia Braggs DsouzaNo ratings yet
- ReseachDocument20 pagesReseachLila GrayNo ratings yet
- Complaint - Wall V Southwest AirlinesDocument94 pagesComplaint - Wall V Southwest AirlinesDaniel MillerNo ratings yet
- Risk Assessment - Placing of Transformer - TTSDocument6 pagesRisk Assessment - Placing of Transformer - TTSnsadnan100% (2)
- Audiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The LiteratureDocument12 pagesAudiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The Literaturericardorojas2403No ratings yet
- New Era of Filipino Youth VolunteerismDocument11 pagesNew Era of Filipino Youth VolunteerismArvhie Santos100% (1)
- Safety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingDocument8 pagesSafety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingElizabeth Trejo MoralesNo ratings yet
- Service Manual FABIAN - 1.1Document48 pagesService Manual FABIAN - 1.1Алексей100% (1)
- Provisional Combined Merit List of Candidates Applied For MDS Courses Under NEET PG 2021Document11 pagesProvisional Combined Merit List of Candidates Applied For MDS Courses Under NEET PG 2021pkv2302No ratings yet
- Barangay Nutrition Profile or Situation Analysis 1Document2 pagesBarangay Nutrition Profile or Situation Analysis 1ann29No ratings yet
- Yokoyama Et Al. C-BED Hikikomori SupportDocument10 pagesYokoyama Et Al. C-BED Hikikomori SupportKayu LowNo ratings yet
- RisperidoneDocument4 pagesRisperidoneimaginarna_88No ratings yet
- Brigo 2014Document22 pagesBrigo 2014Luis CsrNo ratings yet
- Ethnomedicine and Social Control in The Bisayas, PhilippinesDocument14 pagesEthnomedicine and Social Control in The Bisayas, PhilippinesMariano PonceNo ratings yet
- Endocrinology Expected ValuesDocument88 pagesEndocrinology Expected ValuesSandra SánchezNo ratings yet
- Material Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationStewart CredoNo ratings yet
- بايو نظري محاضرة 6 مترجم PDFDocument16 pagesبايو نظري محاضرة 6 مترجم PDFMatti LaythNo ratings yet
- DocumentDocument6 pagesDocumentAnita AkbarNo ratings yet
- Primary Health CareDocument17 pagesPrimary Health CareKevins ChepsirNo ratings yet
- MSDS Stearic Acid NewDocument6 pagesMSDS Stearic Acid NewMASH TLMOSNo ratings yet
- The Nursing Process in Psychiatric/Mental Health NursingDocument30 pagesThe Nursing Process in Psychiatric/Mental Health Nursingmp17570% (1)
- 《新时代的中国青年》白皮书Document60 pages《新时代的中国青年》白皮书Veronica ZhuNo ratings yet
- Swimmer Syndrome in WildlifeDocument2 pagesSwimmer Syndrome in WildlifeALicjaNo ratings yet
- Report On The Transition From Institutional Care To Community-Based Services in 27 Eu Member StatesDocument124 pagesReport On The Transition From Institutional Care To Community-Based Services in 27 Eu Member StatesP.Ch.O.No ratings yet















































































































Download as pptx, pdf, or txt
You might also like
- CBC Absolute Count Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageCBC Absolute Count Test Report Format Example Sample Template Drlogy Lab ReportThota charanNo ratings yet
- Contoh Format DriftDocument12 pagesContoh Format DriftGenevy KarminNo ratings yet
- Nursing Care Plan For DysmenorrheaDocument3 pagesNursing Care Plan For DysmenorrheaMarife Lipana Reyes73% (22)
- Program For Calibration, Preventive Maintenance Final PDFDocument28 pagesProgram For Calibration, Preventive Maintenance Final PDFMatthew Pacardo100% (1)
- Lesson-09 MODUL PDFDocument9 pagesLesson-09 MODUL PDFanggaririn100% (1)
- Bone Marrow Aspirate and BiopsyDocument3 pagesBone Marrow Aspirate and BiopsyatikaNo ratings yet
- Step 2 Clinical Skills (CS) : Content Description and General InformationDocument20 pagesStep 2 Clinical Skills (CS) : Content Description and General Informationdr322No ratings yet
- 2019 Registration FormDocument3 pages2019 Registration FormJoanne Jaramilla Dollente33% (3)
- Histopathology COP 09153 1.0Document15 pagesHistopathology COP 09153 1.0Dr sumithra ravi100% (1)
- Physical and Chemical Properties of UrinalysisDocument39 pagesPhysical and Chemical Properties of UrinalysisDOLORES LIZANo ratings yet
- Allowable Imprecisionfor Laboratory Tests Based On Clinical and Analytical TestDocument6 pagesAllowable Imprecisionfor Laboratory Tests Based On Clinical and Analytical Testsidomoyo100% (1)
- BX 3010 (0C)Document362 pagesBX 3010 (0C)Lâm Hồ Ngọc HãnNo ratings yet
- QualityindicatorsDocument8 pagesQualityindicatorsMishalni PotterNo ratings yet
- QA03005 Critical Testand Critical Result ReportingDocument7 pagesQA03005 Critical Testand Critical Result Reportingdebbie o. azcunaNo ratings yet
- Do 2020-0820Document8 pagesDo 2020-0820wyneth navesisNo ratings yet
- Biosafety in Microbiological and Biomedical Laboratory, 4th Edition (U.S. Department of Health)Document270 pagesBiosafety in Microbiological and Biomedical Laboratory, 4th Edition (U.S. Department of Health)Marlene TapiaNo ratings yet
- Mindray BS 3600 Laboratory Preventive MaintenanceDocument1 pageMindray BS 3600 Laboratory Preventive MaintenanceCaesar A. AlesnaNo ratings yet
- F D A O R A: ORA Laboratory Manual Volume IDocument3 pagesF D A O R A: ORA Laboratory Manual Volume IvictorNo ratings yet
- CHAPTER 8 MedtechDocument17 pagesCHAPTER 8 MedtechKisen DiazNo ratings yet
- 7.CCLM 2018 WG BV HarmonisationDocument8 pages7.CCLM 2018 WG BV HarmonisationJulián Mesa SierraNo ratings yet
- QA QC Clinical MicrosDocument14 pagesQA QC Clinical MicrosKristel S. BalismonNo ratings yet
- Master Health CheckupDocument8 pagesMaster Health CheckupstephenvedhamalarNo ratings yet
- Lab Med Quality IndicatorsDocument15 pagesLab Med Quality IndicatorsMelani Sinasri RenagupitaNo ratings yet
- CA Series Measurement Evaluation and Check MethodsDocument34 pagesCA Series Measurement Evaluation and Check MethodsmarianalinamihaelaNo ratings yet
- Liquid Wastes Proper DisposalDocument2 pagesLiquid Wastes Proper DisposalCaesar A. AlesnaNo ratings yet
- Quality Assurance For Veterinary In-Clinic LaboratoriesDocument29 pagesQuality Assurance For Veterinary In-Clinic Laboratoriesvitalab llanograndeNo ratings yet
- CALIBRATION REPORT (Hema)Document1 pageCALIBRATION REPORT (Hema)jef1234321No ratings yet
- Lab Math Lec (Prelims)Document7 pagesLab Math Lec (Prelims)Merra VenzuelaNo ratings yet
- Manual For Procurement of Diagnostics-001-June2013Document34 pagesManual For Procurement of Diagnostics-001-June2013Jose MirandaNo ratings yet
- TAT AnalysisDocument5 pagesTAT AnalysisSrinivas PolikepatiNo ratings yet
- Primary Sample Collection Manual GD-QSPMDocument51 pagesPrimary Sample Collection Manual GD-QSPMLalit Surykant Chavan100% (1)
- Uncontrolled When PrintedDocument54 pagesUncontrolled When PrintedAmal HaririNo ratings yet
- Empowering Breakthroughs: Science and Lab SolutionsDocument1,182 pagesEmpowering Breakthroughs: Science and Lab Solutionsmoparthi rajeshNo ratings yet
- Quality Control Management in Labortory Services.Document54 pagesQuality Control Management in Labortory Services.Bakhtawar Siddique MemonNo ratings yet
- Nnaca Sop 302Document6 pagesNnaca Sop 302Thusitha LakpriyaNo ratings yet
- Non-Protein Nitrogen Compounds1 (FINALS)Document60 pagesNon-Protein Nitrogen Compounds1 (FINALS)Marydith Ortillo100% (1)
- Wasserlab Brochure Autwomatic Plus 1+2Document10 pagesWasserlab Brochure Autwomatic Plus 1+2Lloid LauretaNo ratings yet
- Critical Value in HematologyDocument8 pagesCritical Value in HematologySTARK DIAGNOSTICSNo ratings yet
- Flow Cytometry Immunophenotyping For Hematologic NeoplasmsDocument28 pagesFlow Cytometry Immunophenotyping For Hematologic NeoplasmsAti Rahmi PurwandariNo ratings yet
- Changes Blood Transfusion Consent AlgorithmDocument1 pageChanges Blood Transfusion Consent AlgorithmLawrence GamboaNo ratings yet
- Sigma Metric QMS in Medical Lab - Palembang IndonesiaDocument76 pagesSigma Metric QMS in Medical Lab - Palembang Indonesiabudi darmanta100% (1)
- ENG-01-F02 Calibration Report Ver.02 20190329 XP-100 S.N B1554 in RSUD Anshari Saleh BanjarmasinDocument4 pagesENG-01-F02 Calibration Report Ver.02 20190329 XP-100 S.N B1554 in RSUD Anshari Saleh BanjarmasinLaboratorium Ansari Saleh100% (1)
- IFCC PPT, July 2017 - Control of Lab Error Through CAPADocument15 pagesIFCC PPT, July 2017 - Control of Lab Error Through CAPAAbdul KalimNo ratings yet
- Drug Testing Consent FormDocument4 pagesDrug Testing Consent FormJeffrey LunaNo ratings yet
- Linearity of Calibration Curves For Analytical MethodsDocument21 pagesLinearity of Calibration Curves For Analytical MethodsAna Carolina SantosNo ratings yet
- The EFLM Update of The European Urinalysis GuidelinesDocument16 pagesThe EFLM Update of The European Urinalysis GuidelinesGawri AbeyNo ratings yet
- Standard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Document17 pagesStandard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Aniruddha ChatterjeeNo ratings yet
- NCM 120J Handout # 1: 2.decent Work Is Employment That "Document10 pagesNCM 120J Handout # 1: 2.decent Work Is Employment That "Nur Fatima SanaaniNo ratings yet
- Lesson 7 QUALITY SYSTEMS MANAGEMENTDocument34 pagesLesson 7 QUALITY SYSTEMS MANAGEMENTMika De VeraNo ratings yet
- A Model For Reducing Medical ErrorsDocument4 pagesA Model For Reducing Medical ErrorsPinto PintoNo ratings yet
- A Handbook On Covid-19 Testing F1Document27 pagesA Handbook On Covid-19 Testing F1Sumesh Shreekhanda ShresthaNo ratings yet
- Retention Times For Records, Reports, and SpecimensDocument1 pageRetention Times For Records, Reports, and SpecimensDayledaniel SorvetoNo ratings yet
- 11 Key Areas Evaluation ToolDocument10 pages11 Key Areas Evaluation Toolpinoybsn26No ratings yet
- Haematology Diagnosis-Army USADocument205 pagesHaematology Diagnosis-Army USAManuela BotisNo ratings yet
- IH Hospital Wide QI Master Spreadsheet 2023Document115 pagesIH Hospital Wide QI Master Spreadsheet 2023Uranchimeg MyagmarchimedNo ratings yet
- A02a00004aen Yumizen G APTT PDFDocument2 pagesA02a00004aen Yumizen G APTT PDFNAKANWAGI JOSLYLINENo ratings yet
- Supportive Supervision Tool For COVID - After Review With Lab Heads PDFDocument10 pagesSupportive Supervision Tool For COVID - After Review With Lab Heads PDFNzema NgakanaNo ratings yet
- 8.7 Nonconforming Outputs: Previous NextDocument10 pages8.7 Nonconforming Outputs: Previous Nextgayathrisrk001No ratings yet
- Assessment ToolDocument13 pagesAssessment Toolal gulNo ratings yet
- Corrective & Preventive ActionDocument2 pagesCorrective & Preventive ActionStephen Lim Kean JinNo ratings yet
- Corrective ActionsDocument3 pagesCorrective Actionsasderbva100% (1)
- Ntungamo: 2018 PLACE Assessment: PL CEDocument4 pagesNtungamo: 2018 PLACE Assessment: PL CEJulius MuhimboNo ratings yet
- Procurement Advert 1 22-23Document1 pageProcurement Advert 1 22-23Julius MuhimboNo ratings yet
- Ims Policy - Integrated Management System: Ergy For The WDocument4 pagesIms Policy - Integrated Management System: Ergy For The WJulius MuhimboNo ratings yet
- Type23 NR2Document16 pagesType23 NR2Julius MuhimboNo ratings yet
- UNBS CertificatesDocument1 pageUNBS CertificatesJulius MuhimboNo ratings yet
- Form - CAR FormDocument6 pagesForm - CAR FormJulius MuhimboNo ratings yet
- Fair Enough PDFDocument6 pagesFair Enough PDFJulius MuhimboNo ratings yet
- 71bd00 Betopan Brosur TRDocument2 pages71bd00 Betopan Brosur TRJulius MuhimboNo ratings yet
- SPD Solar Flood Lights SpecificationsDocument1 pageSPD Solar Flood Lights SpecificationsJulius MuhimboNo ratings yet
- Comformity Certificate NewDocument4 pagesComformity Certificate NewJulius MuhimboNo ratings yet
- Test Report For 2core Flex Cable 14 11 2022Document3 pagesTest Report For 2core Flex Cable 14 11 2022Julius MuhimboNo ratings yet
- Solcourse Polythene DPM V005 TDSDocument3 pagesSolcourse Polythene DPM V005 TDSJulius MuhimboNo ratings yet
- TDS - Technical Data SheetsDocument1 pageTDS - Technical Data SheetsJulius MuhimboNo ratings yet
- JPL Haccp Plan (2) (Repaired)Document13 pagesJPL Haccp Plan (2) (Repaired)Julius MuhimboNo ratings yet
- Rose FoamDocument4 pagesRose FoamJulius MuhimboNo ratings yet
- Material Safety Data Sheet: Wet Chemical Dry Charge (Portable Fire Extinguisher Agent)Document6 pagesMaterial Safety Data Sheet: Wet Chemical Dry Charge (Portable Fire Extinguisher Agent)Julius MuhimboNo ratings yet
- Sika Monotop 610 MsdsDocument14 pagesSika Monotop 610 MsdsJulius MuhimboNo ratings yet
- Newterra Quality Plan - Uganda WWTP - PWTPDocument1 pageNewterra Quality Plan - Uganda WWTP - PWTPJulius MuhimboNo ratings yet
- MSDS - Smoke Detector Test SprayDocument15 pagesMSDS - Smoke Detector Test SprayJulius MuhimboNo ratings yet
- GWC24AGDXE-K3DNA1A - Spec SheetDocument5 pagesGWC24AGDXE-K3DNA1A - Spec SheetJulius MuhimboNo ratings yet
- Anchor Bolt Detail 1Document1 pageAnchor Bolt Detail 1Julius MuhimboNo ratings yet
- EM14WMCBULK - Emmergency Light Data SheetDocument1 pageEM14WMCBULK - Emmergency Light Data SheetJulius MuhimboNo ratings yet
- Tusher Center Working Paper 7Document46 pagesTusher Center Working Paper 7Julius MuhimboNo ratings yet
- 01 35 16 Alteration Project ProceduresDocument8 pages01 35 16 Alteration Project ProceduresJulius MuhimboNo ratings yet
- This Certificate of Compliance Validates The FollowingDocument6 pagesThis Certificate of Compliance Validates The FollowingJulius MuhimboNo ratings yet
- SF01 Food Application Form With All AnnexesDocument11 pagesSF01 Food Application Form With All AnnexesJulius MuhimboNo ratings yet
- Talacogon - 4th Quarter PresentationDocument48 pagesTalacogon - 4th Quarter PresentationRomeo AbrigoNo ratings yet
- Rapport M1-M2Document2 pagesRapport M1-M2LedouxNo ratings yet
- Health Education ProcessDocument25 pagesHealth Education Processdailygrind00011No ratings yet
- Sop For Bio-BurdenDocument5 pagesSop For Bio-BurdenMusyoka Urbanus100% (1)
- SWMS Sample - Safe Work MethodDocument8 pagesSWMS Sample - Safe Work Methodsupasart100% (1)
- JOGNN Guidelines For AuthorsDocument3 pagesJOGNN Guidelines For AuthorsPrathibha Lydia Braggs DsouzaNo ratings yet
- ReseachDocument20 pagesReseachLila GrayNo ratings yet
- Complaint - Wall V Southwest AirlinesDocument94 pagesComplaint - Wall V Southwest AirlinesDaniel MillerNo ratings yet
- Risk Assessment - Placing of Transformer - TTSDocument6 pagesRisk Assessment - Placing of Transformer - TTSnsadnan100% (2)
- Audiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The LiteratureDocument12 pagesAudiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The Literaturericardorojas2403No ratings yet
- New Era of Filipino Youth VolunteerismDocument11 pagesNew Era of Filipino Youth VolunteerismArvhie Santos100% (1)
- Safety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingDocument8 pagesSafety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingElizabeth Trejo MoralesNo ratings yet
- Service Manual FABIAN - 1.1Document48 pagesService Manual FABIAN - 1.1Алексей100% (1)
- Provisional Combined Merit List of Candidates Applied For MDS Courses Under NEET PG 2021Document11 pagesProvisional Combined Merit List of Candidates Applied For MDS Courses Under NEET PG 2021pkv2302No ratings yet
- Barangay Nutrition Profile or Situation Analysis 1Document2 pagesBarangay Nutrition Profile or Situation Analysis 1ann29No ratings yet
- Yokoyama Et Al. C-BED Hikikomori SupportDocument10 pagesYokoyama Et Al. C-BED Hikikomori SupportKayu LowNo ratings yet
- RisperidoneDocument4 pagesRisperidoneimaginarna_88No ratings yet
- Brigo 2014Document22 pagesBrigo 2014Luis CsrNo ratings yet
- Ethnomedicine and Social Control in The Bisayas, PhilippinesDocument14 pagesEthnomedicine and Social Control in The Bisayas, PhilippinesMariano PonceNo ratings yet
- Endocrinology Expected ValuesDocument88 pagesEndocrinology Expected ValuesSandra SánchezNo ratings yet
- Material Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationStewart CredoNo ratings yet
- بايو نظري محاضرة 6 مترجم PDFDocument16 pagesبايو نظري محاضرة 6 مترجم PDFMatti LaythNo ratings yet
- DocumentDocument6 pagesDocumentAnita AkbarNo ratings yet
- Primary Health CareDocument17 pagesPrimary Health CareKevins ChepsirNo ratings yet
- MSDS Stearic Acid NewDocument6 pagesMSDS Stearic Acid NewMASH TLMOSNo ratings yet
- The Nursing Process in Psychiatric/Mental Health NursingDocument30 pagesThe Nursing Process in Psychiatric/Mental Health Nursingmp17570% (1)
- 《新时代的中国青年》白皮书Document60 pages《新时代的中国青年》白皮书Veronica ZhuNo ratings yet
- Swimmer Syndrome in WildlifeDocument2 pagesSwimmer Syndrome in WildlifeALicjaNo ratings yet
- Report On The Transition From Institutional Care To Community-Based Services in 27 Eu Member StatesDocument124 pagesReport On The Transition From Institutional Care To Community-Based Services in 27 Eu Member StatesP.Ch.O.No ratings yet