Download as pptx, pdf, or txt
You might also like
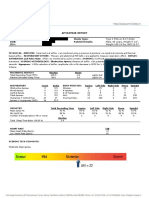
- Sample-Sleep Study Report PDFDocument2 pagesSample-Sleep Study Report PDFgopuNo ratings yet
- Enter APH L&D: 1. A. As Diane's New Assistant, You Need To Flowchart This ProcessDocument5 pagesEnter APH L&D: 1. A. As Diane's New Assistant, You Need To Flowchart This ProcessMichelle Ann Wong100% (1)
- Sleep Study Test: PSG Summary ReportDocument12 pagesSleep Study Test: PSG Summary Reportkuwar palNo ratings yet
- Short Diagnosis Report: PatientDocument6 pagesShort Diagnosis Report: PatientCarmen JurcoaneNo ratings yet
- EU/EEA Digital COVID Certificate EU/EØS Digitalt KoronasertifikatDocument3 pagesEU/EEA Digital COVID Certificate EU/EØS Digitalt KoronasertifikatVegardNo ratings yet
- Interpreting Sleep Studies PrimerDocument23 pagesInterpreting Sleep Studies PrimerLaura MoiseNo ratings yet
- ENT 讀書報告Chapter74 C2 吳丞皓Document20 pagesENT 讀書報告Chapter74 C2 吳丞皓陳永杰No ratings yet
- Obstruc (Ve Sleep Apnea: An Overview: Clinical Commi8ee Society of Anesthesia and Sleep MedicineDocument41 pagesObstruc (Ve Sleep Apnea: An Overview: Clinical Commi8ee Society of Anesthesia and Sleep MedicinepuneetNo ratings yet
- Leep Pnea: Reporters: Desdechado, Niellan Ferrer, Jessa Magkilat, Hanzarri Palmes, Kamillah Sabat, ChristianDocument27 pagesLeep Pnea: Reporters: Desdechado, Niellan Ferrer, Jessa Magkilat, Hanzarri Palmes, Kamillah Sabat, ChristianEira LopezNo ratings yet
- 4) Obstructive Sleep Apnea (Notes)Document94 pages4) Obstructive Sleep Apnea (Notes)Priyanka GosaiNo ratings yet
- OSA UpdatesDocument64 pagesOSA UpdatesRosmadi IsmailNo ratings yet
- Helen Gidey, MD Emory Johns Creek Hospital March 13, 2008Document69 pagesHelen Gidey, MD Emory Johns Creek Hospital March 13, 2008Mohd QureshiNo ratings yet
- Understanding Your Sleep Test ResultsDocument4 pagesUnderstanding Your Sleep Test ResultsChris LeeNo ratings yet
- 1 Basics of OSA 2015Document39 pages1 Basics of OSA 2015saurabh karandeNo ratings yet
- Osa 2008Document48 pagesOsa 2008Jay AayNo ratings yet
- Short Diagnosis Report: PatientDocument6 pagesShort Diagnosis Report: PatientCarmen JurcoaneNo ratings yet
- MR Dalip AroraDocument9 pagesMR Dalip AroraBalwinder KangNo ratings yet
- Obesity Hypoventilation SyndromeDocument88 pagesObesity Hypoventilation SyndromeakijismNo ratings yet
- Obstructive Sleep ApnoeaDocument69 pagesObstructive Sleep ApnoeaPrasanna Datta100% (1)
- Sample PSG LongDocument5 pagesSample PSG LongIrem YitmenNo ratings yet
- Sleep Medicine: Devi Farida UtamiDocument105 pagesSleep Medicine: Devi Farida UtamimufiNo ratings yet
- Obstructive Sleep Apnea SyndromeDocument44 pagesObstructive Sleep Apnea SyndromeSantiNo ratings yet
- Mohamed Ali Hassen Respiration ReportDocument5 pagesMohamed Ali Hassen Respiration ReportMohamed AhmedNo ratings yet
- Obstructive Sleep Apnea - An Overview - Prof. Siraj WaliDocument95 pagesObstructive Sleep Apnea - An Overview - Prof. Siraj WaliGhaida AlshehriNo ratings yet
- Spirometry in Primary Care: Global Initiative For Chronic Obstructive Lung Disease (GOLD) 2008Document59 pagesSpirometry in Primary Care: Global Initiative For Chronic Obstructive Lung Disease (GOLD) 2008zulfikar adiNo ratings yet
- Management of Upper Airway DisorderDocument46 pagesManagement of Upper Airway DisorderSahana Rangarajan100% (1)
- Obstructive Sleep Apnoea SyndromeDocument72 pagesObstructive Sleep Apnoea SyndromeArjun SainiNo ratings yet
- Uyku Laboratuvari: Sleep Architecture SummaryDocument6 pagesUyku Laboratuvari: Sleep Architecture SummaryIrem YitmenNo ratings yet
- Monitoring PerioperatipDocument54 pagesMonitoring Perioperatipjavajavu100% (1)
- Split Night Report: Patient InformationDocument9 pagesSplit Night Report: Patient InformationBalwinder KangNo ratings yet
- Kanishka SarkarDocument9 pagesKanishka SarkarKunal CHOUDHARYNo ratings yet
- Ateletaksis Case ReportDocument17 pagesAteletaksis Case Reportnina purnamasariNo ratings yet
- Shock SepticDocument35 pagesShock SepticAkbar SyarialNo ratings yet
- Chapter 36V3Document25 pagesChapter 36V3عباس أحمد الشيخ جعفرNo ratings yet
- Perioperative Management of OSADocument69 pagesPerioperative Management of OSAandynightmare97No ratings yet
- 1st Rot CP - ReviseDocument43 pages1st Rot CP - ReviseChristian Miguel SabatinNo ratings yet
- 5 - Esc Guidence 2015 Pulmonary HypertensionDocument85 pages5 - Esc Guidence 2015 Pulmonary Hypertensionpuskommedic 003No ratings yet
- Preop Conference AnesthesiaDocument33 pagesPreop Conference AnesthesiaBhi-An BatobalonosNo ratings yet
- A1 CBLDocument59 pagesA1 CBLEbtesamNo ratings yet
- MR PneumoniaDocument14 pagesMR PneumoniaMuhammad Lutfi Al AyubiNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- A1 CBLDocument59 pagesA1 CBLEbtesamNo ratings yet
- 1130 Saturday Sleep Disorders I CollopDocument72 pages1130 Saturday Sleep Disorders I Colloptechang1No ratings yet
- NC Khairunnisa - NeuroDocument18 pagesNC Khairunnisa - NeuroDodi DiNo ratings yet
- Sleep CPGDocument54 pagesSleep CPGbonn maNo ratings yet
- International Institute of Sleep Sciences: Refreshing Sleep and Sustained Alertness... To ALLDocument32 pagesInternational Institute of Sleep Sciences: Refreshing Sleep and Sustained Alertness... To ALLChinmay ShahNo ratings yet
- Interpreting Sleep StudyDocument55 pagesInterpreting Sleep StudySundar RamanathanNo ratings yet
- COPD - Changing Concepts of Pathogenesis and New Ideas For Old TreatmentsDocument49 pagesCOPD - Changing Concepts of Pathogenesis and New Ideas For Old TreatmentsMikee MoganNo ratings yet
- Scenario Title: Community Acquired Pneumonia Learning Outcomes: 1. Assessment and Recognition of The Signs and Symptoms of PneumoniaDocument6 pagesScenario Title: Community Acquired Pneumonia Learning Outcomes: 1. Assessment and Recognition of The Signs and Symptoms of PneumoniaDud AccNo ratings yet
- SOMNOcheck MicroDocument2 pagesSOMNOcheck MicroEvangelosNo ratings yet
- Spirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Document60 pagesSpirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Alkaustariyah LubisNo ratings yet
- PSG Diagnostic Report SampleDocument6 pagesPSG Diagnostic Report SampleZhang Ting TingNo ratings yet
- Responses To Altered PerceptionDocument74 pagesResponses To Altered PerceptionANDREA JUSTINE CARDEÑONo ratings yet
- Assessment Pada Covid-19Document60 pagesAssessment Pada Covid-19FISIOTERAPI TRIMITRANo ratings yet
- Asthma and COPDDocument74 pagesAsthma and COPDCharles YiuNo ratings yet
- Polysomnograpy: Charmain Beatriz A. AtosDocument62 pagesPolysomnograpy: Charmain Beatriz A. AtosPhạm Văn HiệpNo ratings yet
- FND Sleep DisordersDocument10 pagesFND Sleep DisordersQuang VuNo ratings yet
- Short Diagnosis Report: PatientDocument6 pagesShort Diagnosis Report: PatientCarmen JurcoaneNo ratings yet
- Obstructive Sleep Apnea (OSA) Impacting Workplace Safety and CostDocument29 pagesObstructive Sleep Apnea (OSA) Impacting Workplace Safety and CostrahmaputraNo ratings yet
- Chap 104Document6 pagesChap 104revathiiNo ratings yet
- Cross-Linked Hyaluronic Acid Filler Hydrolysis With Hyaluronidase Different Settings ToDocument22 pagesCross-Linked Hyaluronic Acid Filler Hydrolysis With Hyaluronidase Different Settings ToElizabeth TovittoNo ratings yet
- Oxytetracycline PowderDocument1 pageOxytetracycline Powderbejoy karimNo ratings yet
- Teen DepressionDocument8 pagesTeen Depressionsirthana697547No ratings yet
- BG - GB - 07 Lozovey PDFDocument608 pagesBG - GB - 07 Lozovey PDFalifia fitriNo ratings yet
- Exercise and Physical Activity For Older Adults (Powerpoint)Document28 pagesExercise and Physical Activity For Older Adults (Powerpoint)vernonadams42100% (1)
- Care of Postpartum PatientsDocument35 pagesCare of Postpartum PatientsCHi NAi100% (1)
- Lec 7 Care of Clients With Problems in Oxygenation Part 1Document185 pagesLec 7 Care of Clients With Problems in Oxygenation Part 1Chucky VergaraNo ratings yet
- Content - E779462 - 847 Jurnal 5 Definisi Hairy Tongue PDFDocument2 pagesContent - E779462 - 847 Jurnal 5 Definisi Hairy Tongue PDFJeevithaNo ratings yet
- Room Data SheetDocument306 pagesRoom Data SheetAlroukn MechanicalNo ratings yet
- Summary Tables: Bigg Pharmaceutical Company BP3304-002Document55 pagesSummary Tables: Bigg Pharmaceutical Company BP3304-002Uttam SinghNo ratings yet
- Manual PainpenDocument2 pagesManual PainpenElson GomesNo ratings yet
- +++ Eye Problems in Livestock - Infonet BiovisionDocument10 pages+++ Eye Problems in Livestock - Infonet BiovisionkakunguccNo ratings yet
- Bramley 2000Document5 pagesBramley 2000Andres SalcedoNo ratings yet
- Bib R 5864Document117 pagesBib R 5864Yuridia RodríguezNo ratings yet
- The Immune SystemDocument9 pagesThe Immune SystemVictoriaNo ratings yet
- Organ Donation Myths and Facts - Organ DonorDocument4 pagesOrgan Donation Myths and Facts - Organ Donor13WMAZNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationDanilo Clerigo Sr.No ratings yet
- Republic of The Philippines Western Mindanao State University College of Nursing Zamboanga CityDocument6 pagesRepublic of The Philippines Western Mindanao State University College of Nursing Zamboanga Cityalaysa udokNo ratings yet
- FDARDocument3 pagesFDARNMDNMSSDNo ratings yet
- End-Stage Renal Disease Kidney Transplantation TopDocument8 pagesEnd-Stage Renal Disease Kidney Transplantation Topmondae175934No ratings yet
- Maths For Midwifery and Nursing Dosage Calculation - WorksheetDocument5 pagesMaths For Midwifery and Nursing Dosage Calculation - WorksheetMiles Brianne Lymer A. OlvidoNo ratings yet
- CertificateDocument1 pageCertificatechinni kumarNo ratings yet
- Class ProphecyDocument3 pagesClass ProphecyRaisah Bint AbdullahNo ratings yet
- Development of A Protovol For The Management of Obstetric Erb's Palsy 2015Document6 pagesDevelopment of A Protovol For The Management of Obstetric Erb's Palsy 2015Michael HalimNo ratings yet
- Sample Medical CertificateDocument1 pageSample Medical CertificateAce Anthony Figueroa CaroNo ratings yet
- GTR For Oro Antral CommunicationDocument3 pagesGTR For Oro Antral CommunicationSuhas PrabhakarNo ratings yet
- Pacemakers, Cardiac, External, Noninvasive Electrodes Invasive Electrodes, TransesophagealDocument10 pagesPacemakers, Cardiac, External, Noninvasive Electrodes Invasive Electrodes, TransesophagealKevin RubioNo ratings yet
- Blood Transfusion Notes For StudentsDocument5 pagesBlood Transfusion Notes For StudentsMegan TurnerNo ratings yet