Download as pptx, pdf, or txt
You might also like
- Case Study Rheumatoid ArthritisDocument16 pagesCase Study Rheumatoid ArthritisJessy Mallo100% (2)
- OsteoarthritisDocument40 pagesOsteoarthritiskylieverNo ratings yet
- 87 Slides Fundamentals in Orthopedic Surgery 2019Document88 pages87 Slides Fundamentals in Orthopedic Surgery 2019Mark Samuel Tanchoco100% (1)
- Pharm MnemonicsDocument33 pagesPharm MnemonicsThomson George75% (4)
- Lecture 11aDocument33 pagesLecture 11amukhtarjaballaNo ratings yet
- Osteoarthritis: Dr. Angelo Smith M.D WHPLDocument51 pagesOsteoarthritis: Dr. Angelo Smith M.D WHPLChuks LeviNo ratings yet
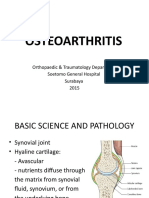
- Osteoarthritis: Orthopaedic & Traumatology Department Soetomo General Hospital Surabaya 2015Document31 pagesOsteoarthritis: Orthopaedic & Traumatology Department Soetomo General Hospital Surabaya 2015internship nganjukNo ratings yet
- Osteoarthritis 191016103144Document49 pagesOsteoarthritis 191016103144dr.abouzaid098No ratings yet
- OSTHEOARTHIRITISDocument25 pagesOSTHEOARTHIRITISOndari gisemba OSINDENo ratings yet
- Osteoarthritis of The Knee HKDocument31 pagesOsteoarthritis of The Knee HKFira Wahidah FirdausNo ratings yet
- 2025 Osteoarthritis 2013 PDFDocument40 pages2025 Osteoarthritis 2013 PDFwahyu andayaniNo ratings yet
- Osteoarthritis: - Typically Affects The Fingers, Spine, Hips andDocument36 pagesOsteoarthritis: - Typically Affects The Fingers, Spine, Hips andsuyatmiNo ratings yet
- YOU Don'T Have To Live With Joint Pain: A Patient'S Guide To The Causes and Treatment of Joint PainDocument18 pagesYOU Don'T Have To Live With Joint Pain: A Patient'S Guide To The Causes and Treatment of Joint PainbaboosabNo ratings yet
- Osteo Arthit IsDocument19 pagesOsteo Arthit IsShaa ShawalishaNo ratings yet
- OsteoarthritisDocument29 pagesOsteoarthritisniekoNo ratings yet
- Muskuloskeletal 2012 NaufalDocument53 pagesMuskuloskeletal 2012 Naufaldahlia kharisma wardhaniNo ratings yet
- Oa OsteoaethritisDocument30 pagesOa Osteoaethritismohamed mowafeyNo ratings yet
- Osteoarthritis: Ferdinand Robert JKKM CPT KPMDocument40 pagesOsteoarthritis: Ferdinand Robert JKKM CPT KPMFerdinand RobertNo ratings yet
- Musculoskeletal AssessmentDocument98 pagesMusculoskeletal AssessmentAbdurehman AyeleNo ratings yet
- Musculoskeletal Disorders 21 Dec. 2021Document61 pagesMusculoskeletal Disorders 21 Dec. 2021sofiamansoorNo ratings yet
- Osteoarthritis: Dr. C. C. VisserDocument85 pagesOsteoarthritis: Dr. C. C. VisserAhmad Fathira FitraNo ratings yet
- Lect 6Document37 pagesLect 6eslambasuony98No ratings yet
- Musculoskeletal SystemDocument6 pagesMusculoskeletal SystemsimonedarlingNo ratings yet
- ArthritisDocument30 pagesArthritisprasherpratik1984No ratings yet
- OsteoarthritisDocument45 pagesOsteoarthritisMar ClrNo ratings yet
- Lecture 11aDocument40 pagesLecture 11aElliya Rosyida67% (3)
- OsteoarthritisDocument19 pagesOsteoarthritisESHA SIDDIQUENo ratings yet
- OSTEOARTHRITISDocument4 pagesOSTEOARTHRITISapi-3822433100% (3)
- 3-22 Slides Arthritis-CIS2016 CoxDocument42 pages3-22 Slides Arthritis-CIS2016 CoxbAmNo ratings yet
- Osteoarthritis - Kali NursaidaDocument18 pagesOsteoarthritis - Kali NursaidaAbeir Abdulhakim SampornaNo ratings yet
- Ra and Osteoarthritis R IfDocument43 pagesRa and Osteoarthritis R IfsnfhanNo ratings yet
- Musculo-Skeletal SystemDocument111 pagesMusculo-Skeletal SystemjohnuwakijijweNo ratings yet
- Osteoarthritis: Heberden's NodesDocument4 pagesOsteoarthritis: Heberden's NodesAmalNo ratings yet
- Rehabilitation in Musculoskeletal - Dr. Ibrahim Agung, SPKFR (K)Document64 pagesRehabilitation in Musculoskeletal - Dr. Ibrahim Agung, SPKFR (K)igd rsudcpNo ratings yet
- MS 36Document7 pagesMS 36jefrocNo ratings yet
- 2027 Osteoarthritis of The KneeDocument36 pages2027 Osteoarthritis of The KneeMark KovalNo ratings yet
- Oa RaDocument24 pagesOa RaRehab NaeemNo ratings yet
- Osteoarthritis: "Degenerative Joint Disease"Document30 pagesOsteoarthritis: "Degenerative Joint Disease"Kim GonzalesNo ratings yet
- Fracture: Edfran Jed A. Serino MSN 303Document34 pagesFracture: Edfran Jed A. Serino MSN 303Edfran Jed SerinoNo ratings yet
- OsteoarthritisDocument23 pagesOsteoarthritisednamwaka03No ratings yet
- Name Seat #: Class: Assignment On Submitted To: EBP2001051 1 Year Eve (A) Joint DisordersDocument11 pagesName Seat #: Class: Assignment On Submitted To: EBP2001051 1 Year Eve (A) Joint DisordersAbdul WasayNo ratings yet
- ArthritisDocument54 pagesArthritisPeby M. Ramdhan100% (1)
- OsteoarthritisDocument39 pagesOsteoarthritisRohit RajeevNo ratings yet
- Osteoarthritis: (Degenerative Arthritis/osteoarthrosis/hypertrophic Arthritis)Document64 pagesOsteoarthritis: (Degenerative Arthritis/osteoarthrosis/hypertrophic Arthritis)Linda SugiartoNo ratings yet
- Chapter 3 HTDocument65 pagesChapter 3 HTtesfamichael mengistuNo ratings yet
- Osteoarthritis (Oa) July 2010Document17 pagesOsteoarthritis (Oa) July 2010Ooi Ah GuanNo ratings yet
- 2 2-ArthritidesDocument76 pages2 2-ArthritidesAvinash KaushikNo ratings yet
- Mayumi - How To Cure OsteoarthritisDocument4 pagesMayumi - How To Cure OsteoarthritisMayumi SariputraNo ratings yet
- OA Presentation Parth SinghDocument20 pagesOA Presentation Parth Singhparthsingh4211No ratings yet
- 1-22 Osteoporosis & Hip PainDocument79 pages1-22 Osteoporosis & Hip PaintarikeopsNo ratings yet
- Introduction OADocument3 pagesIntroduction OAMae UsquisaNo ratings yet
- Osteoarthritis NotesDocument11 pagesOsteoarthritis Notesjesmitha2740No ratings yet
- Oa KneeDocument17 pagesOa KneeChitra ChauhanNo ratings yet
- Lecture 11aDocument39 pagesLecture 11aSourabh KulkarniNo ratings yet
- Degenerative Disorders of JointsDocument25 pagesDegenerative Disorders of JointsayuNo ratings yet
- V.Lokeesan, BSN T.Assistant Lecturer FHCS, EuslDocument39 pagesV.Lokeesan, BSN T.Assistant Lecturer FHCS, EuslMourian AmanNo ratings yet
- Medical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)Document41 pagesMedical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)YanuarNo ratings yet
- Surgery - Dychioco - Musculo Skeletal InjuriesDocument79 pagesSurgery - Dychioco - Musculo Skeletal Injuries3rd yrsNo ratings yet
- MedSurg Chapter 51 OutlineDocument7 pagesMedSurg Chapter 51 OutlineJosephine Navarro100% (1)
- OsteoarthritisDocument34 pagesOsteoarthritisLaiba KhanNo ratings yet
- Distal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDistal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 2.2. Physical-Chemical Factors Affecting Oral Absorption (6hrs)Document60 pages2.2. Physical-Chemical Factors Affecting Oral Absorption (6hrs)Abera JamboNo ratings yet
- Bioavailability: by Abera JDocument59 pagesBioavailability: by Abera JAbera JamboNo ratings yet
- Pharmacotherapy of RADocument44 pagesPharmacotherapy of RAAbera JamboNo ratings yet
- Pharmacotherapy of GoutDocument40 pagesPharmacotherapy of GoutAbera JamboNo ratings yet
- Pharmacotherapy of OsteoporosisDocument49 pagesPharmacotherapy of OsteoporosisAbera JamboNo ratings yet
- Pharmacotherapy of HTNDocument57 pagesPharmacotherapy of HTNAbera JamboNo ratings yet
- Pharmacotherapy of VTEDocument80 pagesPharmacotherapy of VTEAbera JamboNo ratings yet
- Pharmacotherapy of ACSDocument79 pagesPharmacotherapy of ACSAbera JamboNo ratings yet
- Pharmacotherapy of Heart Failure: Abera J. (Bpharm., MSC in Clinical Pharmacy) School of Pharmacy, CHMS, HuDocument79 pagesPharmacotherapy of Heart Failure: Abera J. (Bpharm., MSC in Clinical Pharmacy) School of Pharmacy, CHMS, HuAbera JamboNo ratings yet
- Aceclofenac For Pain ManagmentDocument11 pagesAceclofenac For Pain Managmentsyeda tahsin naharNo ratings yet
- Case Study On Gastrointestinal Disorders PDFDocument5 pagesCase Study On Gastrointestinal Disorders PDFJude Micko Bunyi AlipitNo ratings yet
- Side Effects of NSAIDsDocument8 pagesSide Effects of NSAIDsAlmas PrawotoNo ratings yet
- Kine 3p80 Hip Injury Assignment 1Document4 pagesKine 3p80 Hip Injury Assignment 1api-437399185No ratings yet
- What Is PolymyositisDocument24 pagesWhat Is PolymyositisAshraf MobyNo ratings yet
- MEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncDocument14 pagesMEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncIrma DamayantiNo ratings yet
- M6 Case StudyDocument5 pagesM6 Case StudylorrieNo ratings yet
- Pregnancy and Lactation AnswersDocument8 pagesPregnancy and Lactation AnswersAoiNo ratings yet
- What Is A Migraine Headache?Document18 pagesWhat Is A Migraine Headache?mrsarojnayak8840No ratings yet
- Saw Palmetto: Also Known AsDocument6 pagesSaw Palmetto: Also Known AsbencleeseNo ratings yet
- Reference Guide For The Pharmacy Licensing Exam - Questions and AnswersDocument81 pagesReference Guide For The Pharmacy Licensing Exam - Questions and AnswersNikka LaborteNo ratings yet
- PainoxiaDocument66 pagesPainoxiaOmar WahbiNo ratings yet
- Lupus: PrintDocument24 pagesLupus: Printmelodia gandezaNo ratings yet
- Newapproachestopain Management: Orrett E. OgleDocument10 pagesNewapproachestopain Management: Orrett E. OgleNajeeb UllahNo ratings yet
- Trade Name Generic Name Group: TetracyclinesDocument11 pagesTrade Name Generic Name Group: Tetracyclinesmisfer72No ratings yet
- Common DrugsDocument15 pagesCommon DrugsKate Penelope DalidNo ratings yet
- Alternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Document159 pagesAlternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Marvin T Verna100% (2)
- Bone Cancer TreatmentDocument14 pagesBone Cancer TreatmentHarshitha Harshitha0% (1)
- Drugs and Dosages PDFDocument4 pagesDrugs and Dosages PDFsharmee sarmientaNo ratings yet
- Drug Companion Peds 2003Document413 pagesDrug Companion Peds 2003Nisar Shaik100% (1)
- Diagnosisandtreatmentof Goutandpseudogoutfor EverydaypracticeDocument24 pagesDiagnosisandtreatmentof Goutandpseudogoutfor EverydaypracticePutri Aswariyah RamliNo ratings yet
- Practice Advisory On The Appropriate Use of Nsaids in Primary CareDocument15 pagesPractice Advisory On The Appropriate Use of Nsaids in Primary CareAsti IndriyaniNo ratings yet
- Naplexq&aDocument81 pagesNaplexq&aRamy Raafat Rezk100% (4)
- AINS CaseDocument11 pagesAINS CaseMarilena TarcaNo ratings yet
- Nervous System Drugs: Drugs For Pain Management: Non-Narcotic and Narcotic AnalgesicsDocument29 pagesNervous System Drugs: Drugs For Pain Management: Non-Narcotic and Narcotic AnalgesicsJon Corpuz AggasidNo ratings yet
- Post Op Pain ManagementDocument42 pagesPost Op Pain ManagementMuhammad Iqbal A GhaniNo ratings yet
- CHF Patient Education Booklet English WebDocument20 pagesCHF Patient Education Booklet English WebBelete NigusieNo ratings yet
- Formulaiton and Pharmacokinetic Evaluation of Naproxen Sodium Modified Release TabletDocument8 pagesFormulaiton and Pharmacokinetic Evaluation of Naproxen Sodium Modified Release TabletiajpsNo ratings yet