Download as pptx, pdf, or txt
You might also like
- Manual Emdr Parts Work Treating Complex TraumaDocument73 pagesManual Emdr Parts Work Treating Complex Traumacora4eva5699100% (1)
- 2017 05 GC Pocket CardDocument2 pages2017 05 GC Pocket Cardapi-312241089No ratings yet
- Norvasc Drug CardDocument1 pageNorvasc Drug CardSheri490No ratings yet
- HadLock BPD ShapeDocument6 pagesHadLock BPD ShapePippo KennedyNo ratings yet
- Electrolytes (3607)Document11 pagesElectrolytes (3607)JennNo ratings yet
- DPN Icu PDFDocument1 pageDPN Icu PDFharoonNo ratings yet
- R1 Orientation, Oncall Issues.Document55 pagesR1 Orientation, Oncall Issues.latifaNo ratings yet
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocument5 pagesEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNo ratings yet
- MI MEDIC CARDS - Reference MaterialDocument26 pagesMI MEDIC CARDS - Reference MaterialAylinNo ratings yet
- Nursing Day Plan - ExcelDocument1 pageNursing Day Plan - ExceltennyrbNo ratings yet
- ICU Checklist For RoundingDocument1 pageICU Checklist For RoundingViolaNo ratings yet
- CXR Interpretation: by Dr. Iqbal TariqDocument19 pagesCXR Interpretation: by Dr. Iqbal TariqSalman Khan100% (1)
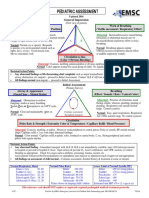
- Pediatric Assessment: General ImpressionDocument2 pagesPediatric Assessment: General ImpressionAghnia Nafila100% (1)
- Nursing CS Abnormal Lung SoundsDocument1 pageNursing CS Abnormal Lung SoundsMahdia akterNo ratings yet
- Module 4 - Cardiac EmergencyDocument30 pagesModule 4 - Cardiac EmergencyElaine AntonetteNo ratings yet
- College of Medicine and Health Sciences: For Public Health C-I StudentsDocument29 pagesCollege of Medicine and Health Sciences: For Public Health C-I StudentsWĩž BŕëãžÿNo ratings yet
- Agenda Bls-AclsDocument2 pagesAgenda Bls-AclsespegehNo ratings yet
- 7th 12th Summer Book Report PDFDocument12 pages7th 12th Summer Book Report PDFlila100% (1)
- Nursing CS Angina-Pectoris-medications 03Document1 pageNursing CS Angina-Pectoris-medications 03Mahdia akterNo ratings yet
- Nursing Care of Clients With Upper Airway or Respiratory DisordersDocument6 pagesNursing Care of Clients With Upper Airway or Respiratory DisordersLuna MarieNo ratings yet
- Memonic Exam 2Document18 pagesMemonic Exam 2Justine Grace TolentinoNo ratings yet
- EVD PosterDocument1 pageEVD PosterDwie 'keonk' UnisaspalaNo ratings yet
- Medical School Notes On Stomach IssuesDocument31 pagesMedical School Notes On Stomach IssuesDeji KajiNo ratings yet
- Acute Abdomen: Medic Curses A MopDocument50 pagesAcute Abdomen: Medic Curses A MopSharaz AhmedNo ratings yet
- Oral CareDocument6 pagesOral CareChristian Jewel GambolNo ratings yet
- Think Nursing! ReportDocument20 pagesThink Nursing! ReportRobert Fraser RNNo ratings yet
- Icu FlowsheetDocument4 pagesIcu FlowsheetdedeandikaNo ratings yet
- ABCDE Education SlidesDocument43 pagesABCDE Education SlidesEvangelina María C. PoliNo ratings yet
- Webinar ACLSDocument52 pagesWebinar ACLSNurhasanahNo ratings yet
- Care of The Unconscious PatientDocument33 pagesCare of The Unconscious Patientta CNo ratings yet
- Med Surg Report Sheet Night Shift FINALDocument2 pagesMed Surg Report Sheet Night Shift FINALCindy AnnNo ratings yet
- Malignant Hyperthermia Fact SheetDocument2 pagesMalignant Hyperthermia Fact Sheetapi-301819201No ratings yet
- Cardiac NotesDocument24 pagesCardiac NotesYary MayorNo ratings yet
- Axis DeviationDocument26 pagesAxis DeviationDanial HassanNo ratings yet
- Icu Adult and PaedsDocument2 pagesIcu Adult and PaedsPrashin RocharamNo ratings yet
- Icu Sop: TOPIC: Length of Stay in ICUDocument5 pagesIcu Sop: TOPIC: Length of Stay in ICURohit RajeevanNo ratings yet
- Nursing CS End of Shift Checklist 03Document1 pageNursing CS End of Shift Checklist 03Ciara GonzalezNo ratings yet
- NCM 109 SKILLS LAB DAY 5.3 Catheterization22Document33 pagesNCM 109 SKILLS LAB DAY 5.3 Catheterization22Joseph DusichNo ratings yet
- EKG RhythmsDocument71 pagesEKG RhythmsalexaNo ratings yet
- Primary Trauma CareDocument48 pagesPrimary Trauma CareKABERA RENENo ratings yet
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- ACLS Algorithms (2011)Document6 pagesACLS Algorithms (2011)senbonsakuraNo ratings yet
- Nursing CS Wound DocumentationDocument1 pageNursing CS Wound DocumentationJazzmine GuraNo ratings yet
- H. OncologyDocument27 pagesH. OncologyGloryJaneNo ratings yet
- Dysrhythmia TestsDocument3 pagesDysrhythmia TestsKimberly WhitesideNo ratings yet
- Bioinstrumentation II: Lecture 4: ECG MachineDocument30 pagesBioinstrumentation II: Lecture 4: ECG MachineHundessa DabaNo ratings yet
- Guide To Oxygen Delivery SystemDocument3 pagesGuide To Oxygen Delivery SystemDarwin Villestas0% (1)
- Midline - Tip of The Sternum-Umbilicus-Symphysis Lateral - Runs Through The Umbilicus Across TheDocument3 pagesMidline - Tip of The Sternum-Umbilicus-Symphysis Lateral - Runs Through The Umbilicus Across TheQuinonez Anna MarieNo ratings yet
- SDPSC Icu Sedation Guidelines of Care Toolkit December 2009Document44 pagesSDPSC Icu Sedation Guidelines of Care Toolkit December 2009yonoNo ratings yet
- Assessing Head, Face and NeckDocument112 pagesAssessing Head, Face and NeckHyacinth Jane Dela PeñaNo ratings yet
- New Icu SheetDocument3 pagesNew Icu SheetJan MarcusNo ratings yet
- Best Practice in ShockDocument30 pagesBest Practice in ShockFoungZanz D. LuffyzNo ratings yet
- PharmaDocument6 pagesPharmaLovely AmadoNo ratings yet
- College of Nursing Procedures Checklist: Giving Subcutaneous InjectionsDocument2 pagesCollege of Nursing Procedures Checklist: Giving Subcutaneous InjectionsCamillus Carillo AngelesNo ratings yet
- Med-Surg Lecture 4th Year 1st Sem (Incomplete)Document70 pagesMed-Surg Lecture 4th Year 1st Sem (Incomplete)Raezhell Dianne RachoNo ratings yet
- Fetal Heart TonesDocument1 pageFetal Heart TonesChristian Clyde N. JakosalemNo ratings yet
- PreclinicalDocument8 pagesPreclinicalKeishaNo ratings yet
- Chapter 5: Analyzing A Rhythm StripDocument7 pagesChapter 5: Analyzing A Rhythm StriptellyNo ratings yet
- Physical Examinations Respiratory System: InspectionDocument5 pagesPhysical Examinations Respiratory System: InspectionAzizan HannyNo ratings yet
- Triage FormDocument2 pagesTriage FormCael LayugNo ratings yet
- How To Read An ECGDocument21 pagesHow To Read An ECGSlychenkoNo ratings yet
- Airway ClearanceDocument24 pagesAirway ClearanceGoddy ManzanoNo ratings yet
- Principles in Trauma ManagementDocument34 pagesPrinciples in Trauma Managementvirz23No ratings yet
- This Study Resource Was: Biology 20IB: Urine Analysis LabDocument2 pagesThis Study Resource Was: Biology 20IB: Urine Analysis LabKALI LAWRENCENo ratings yet
- Pregnancy in End-Stage Renal Disease Patients On Long-Term Hemodialysis: Two Case ReportsDocument3 pagesPregnancy in End-Stage Renal Disease Patients On Long-Term Hemodialysis: Two Case Reportsade_liaNo ratings yet
- Test Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensDocument11 pagesTest Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensWilbur Penny100% (40)
- WIlson DiseaseDocument11 pagesWIlson DiseaseOrdnas UcimNo ratings yet
- NCP Dengue FeverDocument3 pagesNCP Dengue FeverLorainne BallesterosNo ratings yet
- Step 1 Estudio WORDDocument171 pagesStep 1 Estudio WORDdenisse moraNo ratings yet
- Non KeratinocytesDocument21 pagesNon KeratinocytesAbi AbiramithangamNo ratings yet
- Acute Diverticulitis-GcpDocument85 pagesAcute Diverticulitis-Gcpkuro hanabusaNo ratings yet
- DIC Case StudyDocument7 pagesDIC Case StudyRobertNo ratings yet
- Edit Dafpus TK 1-1Document3 pagesEdit Dafpus TK 1-1annewidiatmoNo ratings yet
- KKM Policies & Procedures On Infection Prevention and Control 2019 PDFDocument305 pagesKKM Policies & Procedures On Infection Prevention and Control 2019 PDFAenz Princess KkmNo ratings yet
- Surat Buat VisaDocument12 pagesSurat Buat VisaNurul FitrianaNo ratings yet
- Benefits of Butterfly PeaDocument2 pagesBenefits of Butterfly PeaMarie MarsilNo ratings yet
- Stages of LaborDocument3 pagesStages of LaborJepoy GomezNo ratings yet
- Columbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeDocument1 pageColumbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeIzabel EstevamNo ratings yet
- Dsa FLXM Pi en 00Document7 pagesDsa FLXM Pi en 00yantuNo ratings yet
- Ow Q 51-100 (14.11.09)Document102 pagesOw Q 51-100 (14.11.09)PradeepNo ratings yet
- TCA CrossDocument6 pagesTCA CrosssalivaNo ratings yet
- Resume Charlie Castro 2Document13 pagesResume Charlie Castro 2JasonV.PanayNo ratings yet
- Diagnosis Banding Kejang DemamDocument7 pagesDiagnosis Banding Kejang DemamCesaNo ratings yet
- 2 - CNS QDocument4 pages2 - CNS QTan Hing LeeNo ratings yet
- Principles For Aseptic Technique - Information For Healthcare Workers - December 2021Document5 pagesPrinciples For Aseptic Technique - Information For Healthcare Workers - December 2021ebubechukwu echefuNo ratings yet
- Extended Trochanteric Osteotomy in Revision Total Hip Arthroplasty - Contemporary Outcomes of 612 HipsDocument12 pagesExtended Trochanteric Osteotomy in Revision Total Hip Arthroplasty - Contemporary Outcomes of 612 Hips阿欧有怪兽No ratings yet
- Assignment 1.03Document1 pageAssignment 1.03bianca chartrandNo ratings yet
- PoliomyelitisDocument81 pagesPoliomyelitisKaycee Glene CalubNo ratings yet
- CHN ComputationDocument3 pagesCHN ComputationRhyann AdvinculaNo ratings yet
- Blood - BLD 2022 018896 MainDocument5 pagesBlood - BLD 2022 018896 MainRana RaedNo ratings yet