
Multigene Genomic Testing (ONCOTYPE DX) Among New York Prostate Cancer Patients
Multigene Genomic Testing (ONCOTYPE DX) Among New York Prostate Cancer Patients
You might also like
- Introduction To The Philosophy of The Human PersonDocument24 pagesIntroduction To The Philosophy of The Human Personbethuel100% (2)
- Intern Log Book JazanUDocument41 pagesIntern Log Book JazanUdrstrao100% (1)
- Shen 2018Document12 pagesShen 2018Muhammad Yusuf HanifNo ratings yet
- Brief T.B. Control ProgrammeDocument3 pagesBrief T.B. Control ProgrammeAbdullah AfzalNo ratings yet
- 1 s2.0 S0006497121006340 MainDocument13 pages1 s2.0 S0006497121006340 Mainresi silviaNo ratings yet
- CCO Clin Onc June 2019 504Document13 pagesCCO Clin Onc June 2019 504bingqi xuNo ratings yet
- Therapy: Non-Pharmacologic: y Z X Z Z Z y KDocument1 pageTherapy: Non-Pharmacologic: y Z X Z Z Z y KsondiNo ratings yet
- Self-Collected Extra-Genital Gonorrhea and Chlamydia Testing For MSMDocument13 pagesSelf-Collected Extra-Genital Gonorrhea and Chlamydia Testing For MSMGuilherme SttelletNo ratings yet
- Laproscopic Omental Patch For Perforated Peptic Ulcer Disease 1Document26 pagesLaproscopic Omental Patch For Perforated Peptic Ulcer Disease 1Sagor Kumar DasNo ratings yet
- 2019 Preceptorship H N TNM Classification 8th Edition Jean Pascal MachielsDocument36 pages2019 Preceptorship H N TNM Classification 8th Edition Jean Pascal MachielsGalgalo GarbichaNo ratings yet
- Comprehensive Management of Prostate Cancer 20150821Document30 pagesComprehensive Management of Prostate Cancer 20150821Marhama FitrianiNo ratings yet
- FLAD1 Is Up-Regulated in Gastric Cancer and Is A Potential Prediction of PrognosisDocument10 pagesFLAD1 Is Up-Regulated in Gastric Cancer and Is A Potential Prediction of PrognosisAriani ArinNo ratings yet
- Honey Bees and Also Untamed Pollinators Vary Within Their Desire Regarding and Employ of Presented Flower Sourceshlwhg PDFDocument1 pageHoney Bees and Also Untamed Pollinators Vary Within Their Desire Regarding and Employ of Presented Flower Sourceshlwhg PDFlowtimer98No ratings yet
- 1 s2.0 S1120179718301078 MainDocument1 page1 s2.0 S1120179718301078 MainAdeola AshiruNo ratings yet
- JTCVS 2004 - Wright 2004Document9 pagesJTCVS 2004 - Wright 2004vinicius.alvarez3No ratings yet
- #40 Status of The Thyroid Ultrasound Examination Results (January 15, 2021)Document6 pages#40 Status of The Thyroid Ultrasound Examination Results (January 15, 2021)Yuri HiranumaNo ratings yet
- Huh Et Al-2010-Journal of Surgical OncologyDocument5 pagesHuh Et Al-2010-Journal of Surgical OncologyFieska AzizahNo ratings yet
- RX PDFDocument3 pagesRX PDFMASIEL AMELIA BARRANTES ARCENo ratings yet
- Jurnal Reading Dermatitis Kontak Iritan: Ahmad Amsori Yuli Darlinawati Pembimbing: Dr. Arif Effendi, SP - KKDocument17 pagesJurnal Reading Dermatitis Kontak Iritan: Ahmad Amsori Yuli Darlinawati Pembimbing: Dr. Arif Effendi, SP - KKAhmad AmsoryNo ratings yet
- Kol Slide Kit Atac 100Document43 pagesKol Slide Kit Atac 100api-26302710No ratings yet
- Assessment of Clinician Accuracy For Diagnosing MeDocument3 pagesAssessment of Clinician Accuracy For Diagnosing MeYilianeth Mena DazaNo ratings yet
- DAPA-HF and DELIVER Pooled Meta-Analysis. Nature Med. 2022 - With VEEVADocument16 pagesDAPA-HF and DELIVER Pooled Meta-Analysis. Nature Med. 2022 - With VEEVAzdmoorNo ratings yet
- Artículo Ca PróstataDocument12 pagesArtículo Ca PróstataEddy AuzNo ratings yet
- FTPDocument5 pagesFTPHaya RihanNo ratings yet
- HOI160023supp1 Prod PDFDocument10 pagesHOI160023supp1 Prod PDFcassieNo ratings yet
- Annie Anderson Obesity The Elephant in The RoomDocument18 pagesAnnie Anderson Obesity The Elephant in The RoomVignesh JayaNo ratings yet
- Stampede M0 ASTRO Presentation Sept 2014Document24 pagesStampede M0 ASTRO Presentation Sept 2014Prof_Nick_JamesNo ratings yet
- Ujian Metris II - HerikaDocument14 pagesUjian Metris II - HerikaErie MoetzNo ratings yet
- #41 Status of The Thyroid Ultrasound Examination Results (May 17, 2021)Document6 pages#41 Status of The Thyroid Ultrasound Examination Results (May 17, 2021)Yuri HiranumaNo ratings yet
- Stent For Malignant Large Bowl ObstructionDocument6 pagesStent For Malignant Large Bowl ObstructionAndrei ZbucheaNo ratings yet
- Sex Transm Infect. 2011 Aug 87 (5) 385-8Document6 pagesSex Transm Infect. 2011 Aug 87 (5) 385-8Cynthia Patricia Manotas AltamarNo ratings yet
- Comparison Between Fine Needle Aspiration and Core Needle Biopsy For The Diagnosis of Thyroid Nodules: Effective Indications According To US FindingsDocument7 pagesComparison Between Fine Needle Aspiration and Core Needle Biopsy For The Diagnosis of Thyroid Nodules: Effective Indications According To US FindingsRama DanusNo ratings yet
- ASTRO23Slides VanasDocument18 pagesASTRO23Slides Vanasjohapatino46No ratings yet
- Essay Komstat Farhan HF RahmanDocument5 pagesEssay Komstat Farhan HF RahmantaufikramadhaniNo ratings yet
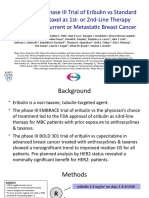
- Randomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast CancerDocument14 pagesRandomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast Canceralberto cabelloNo ratings yet
- #42 Status of The Thyroid Ultrasound Examination Results (July 27, 2021)Document6 pages#42 Status of The Thyroid Ultrasound Examination Results (July 27, 2021)Yuri HiranumaNo ratings yet
- Abstracts From The Global Embolization Sympo 2021 Journal of Vascular and inDocument21 pagesAbstracts From The Global Embolization Sympo 2021 Journal of Vascular and infreedy freedyNo ratings yet
- Prognostic Value of Ki-67 For Prostate Cancer Death in A Conservatively Managed CohortDocument7 pagesPrognostic Value of Ki-67 For Prostate Cancer Death in A Conservatively Managed Cohorthuu2toanNo ratings yet
- M7. MIII. O6a. Screening de CADocument29 pagesM7. MIII. O6a. Screening de CARogerio FernandesNo ratings yet
- Comparative Effectiveness Study of Single High-Dose Cisplatin WithDocument19 pagesComparative Effectiveness Study of Single High-Dose Cisplatin WithGentek PharmaNo ratings yet
- Management and Prognosis of Pancreatic Cancer Over A 30-Year PeriodDocument4 pagesManagement and Prognosis of Pancreatic Cancer Over A 30-Year PeriodAxelle BoukambaNo ratings yet
- Articol Extenso 2Document4 pagesArticol Extenso 2David CalinNo ratings yet
- CNCR 29602Document8 pagesCNCR 29602Joseph PerezNo ratings yet
- Khan SlidesDocument17 pagesKhan Slidesalberto cabelloNo ratings yet
- 4-Pres-Sardjito-Prof. Dr. Djaswadi Dasuki - M.ph. - PhD. - SpOGDocument12 pages4-Pres-Sardjito-Prof. Dr. Djaswadi Dasuki - M.ph. - PhD. - SpOGLukas Anjar KrismulyonoNo ratings yet
- #46 Status of The Thyroid Ultrasound Examination Results (Released On December 2, 2022)Document7 pages#46 Status of The Thyroid Ultrasound Examination Results (Released On December 2, 2022)Yuri HiranumaNo ratings yet
- Applying Data-Driven Imaging Biomarker in Mammography For Breast Cancer Screening: Preliminary StudyDocument8 pagesApplying Data-Driven Imaging Biomarker in Mammography For Breast Cancer Screening: Preliminary StudyDébora XavierNo ratings yet
- Establishment and Validation of PrognosticDocument10 pagesEstablishment and Validation of PrognosticMiss AmyNo ratings yet
- EARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDDocument31 pagesEARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDHengky TanNo ratings yet
- #43 Status of The Thyroid Ultrasound Examination Results (October 15, 2021)Document6 pages#43 Status of The Thyroid Ultrasound Examination Results (October 15, 2021)Yuri HiranumaNo ratings yet
- An Example of Propensity Score Matched ADocument10 pagesAn Example of Propensity Score Matched A古寒州No ratings yet
- MCHA022 (Analytical Chemistry 2)Document62 pagesMCHA022 (Analytical Chemistry 2)Mbali MazongweNo ratings yet
- Icmcrj 1 1011Document8 pagesIcmcrj 1 1011Shivaramakrishna SriramojuNo ratings yet
- Marshall 2007Document25 pagesMarshall 2007Allan Amaral da HoraNo ratings yet
- 727 Final+CommentsDocument14 pages727 Final+CommentsRahimSMCSwatNo ratings yet
- #44 Status of The Thyroid Ultrasound Examination Results (May 13, 2022)Document7 pages#44 Status of The Thyroid Ultrasound Examination Results (May 13, 2022)Yuri HiranumaNo ratings yet
- VEGF Expression in Colorectal Cancer Metastatic LyDocument14 pagesVEGF Expression in Colorectal Cancer Metastatic LyNana LianaNo ratings yet
- Pestana, 2022Document4 pagesPestana, 2022prof.rodrigopestanaNo ratings yet
- Journal Pone 0106203 PDFDocument7 pagesJournal Pone 0106203 PDFAnonymous 4vrma12QgbNo ratings yet
- PresentationDocument15 pagesPresentationSatish SinghNo ratings yet
- Supervised Classification Techniques and Deep Learning For Mortality Prediction in Sepsis PatientsDocument6 pagesSupervised Classification Techniques and Deep Learning For Mortality Prediction in Sepsis PatientsFabian Alberto Jaimes BarraganNo ratings yet
- First Hrpta MeetingDocument4 pagesFirst Hrpta MeetingbethuelNo ratings yet
- SF2 - NovemberDocument9 pagesSF2 - NovemberbethuelNo ratings yet
- HGP Eportfolio Editable 2022 2023Document34 pagesHGP Eportfolio Editable 2022 2023bethuelNo ratings yet
- Perdev-Dll-Aug. 29-Sept 2, 2022Document3 pagesPerdev-Dll-Aug. 29-Sept 2, 2022bethuelNo ratings yet
- Perdev Sept 5 - Sept 9, 2022Document3 pagesPerdev Sept 5 - Sept 9, 2022bethuelNo ratings yet
- Emotions ActivityDocument18 pagesEmotions ActivitybethuelNo ratings yet
- Manual Blood Pressure Competency ChecklistDocument1 pageManual Blood Pressure Competency ChecklistbethuelNo ratings yet
- Perdev Sept 12-16, 2022Document4 pagesPerdev Sept 12-16, 2022bethuelNo ratings yet
- Introduction To The Philosophy of The Human Person: Quarter 2 - Module 3Document20 pagesIntroduction To The Philosophy of The Human Person: Quarter 2 - Module 3bethuelNo ratings yet
- PD DLL March 06 10 2017Document3 pagesPD DLL March 06 10 2017bethuelNo ratings yet
- Introduction To The Philosophy of The Human Person: Quarter 2 - Module 4bDocument21 pagesIntroduction To The Philosophy of The Human Person: Quarter 2 - Module 4bbethuel100% (1)
- Final DLL Q1Document43 pagesFinal DLL Q1bethuelNo ratings yet
- Introduction To The Philosophy of The Human Person: Quarter 2 - Module 5Document19 pagesIntroduction To The Philosophy of The Human Person: Quarter 2 - Module 5bethuel100% (3)
- Sports Track 11: 2 Semester - Module 2b: Safety and First AidDocument18 pagesSports Track 11: 2 Semester - Module 2b: Safety and First AidbethuelNo ratings yet
- Matthias Rath Cancer Book - Vitamin C and Lysine For Cancer TreatmentDocument40 pagesMatthias Rath Cancer Book - Vitamin C and Lysine For Cancer TreatmentEbook PDF100% (3)
- Neural Tube Defects (Anatomy)Document11 pagesNeural Tube Defects (Anatomy)nur athiraNo ratings yet
- AlfanoDocument3 pagesAlfanoapi-532399186No ratings yet
- PPE and DrapesDocument27 pagesPPE and DrapesBang Tut ChuolNo ratings yet
- Cleaning+Standards+2021 v1.0+ (Revised+final)Document48 pagesCleaning+Standards+2021 v1.0+ (Revised+final)ابراهيم الحربيNo ratings yet
- Nurs 479 Professional DevelopmentDocument12 pagesNurs 479 Professional Developmentapi-490209035No ratings yet
- Mri Request FormDocument1 pageMri Request Formraad_alghamdi_1No ratings yet
- Form006 Survey Internship Student EvaluationDocument4 pagesForm006 Survey Internship Student Evaluationalexis tamayoNo ratings yet
- El Proyecto de InglesDocument3 pagesEl Proyecto de Ingleskim jojoNo ratings yet
- Batuk Dengan Atau Tanpa Sesak Nafas: DR Ari Kurniasih M, Ked (Ped), SpaDocument27 pagesBatuk Dengan Atau Tanpa Sesak Nafas: DR Ari Kurniasih M, Ked (Ped), Spacitra dewiNo ratings yet
- Drug Scenario in The PhilippinesDocument15 pagesDrug Scenario in The PhilippinesCalix GonzalesNo ratings yet
- Water Supply and Sanitation in IndiaDocument6 pagesWater Supply and Sanitation in IndiaMunish Dogra50% (2)
- Biomedical Ethics and Qawaid FiqhiyyahDocument12 pagesBiomedical Ethics and Qawaid FiqhiyyahSurgeon AsimNo ratings yet
- Clinical: ResearchDocument13 pagesClinical: ResearchAahil SumairNo ratings yet
- RLE Activity 1 - An Overview of MY COMMUNITY (Vizconde, Ehreiz Raiden C. BSN3-A)Document2 pagesRLE Activity 1 - An Overview of MY COMMUNITY (Vizconde, Ehreiz Raiden C. BSN3-A)Raiden VizcondeNo ratings yet
- 141 02Document8 pages141 02Shanty AnitaNo ratings yet
- Lab 7Document28 pagesLab 7Dave OrlandoNo ratings yet
- 180-SCF-3314 - Job DescriptionDocument17 pages180-SCF-3314 - Job DescriptionUmair AshfaqNo ratings yet
- Unit 1 Definitions/key Terms Varcarolis Mental Health NursingDocument6 pagesUnit 1 Definitions/key Terms Varcarolis Mental Health Nursingatl_nurse_studentNo ratings yet
- FHO, CHI, WC, ASSURE, Coparison One PagerDocument1 pageFHO, CHI, WC, ASSURE, Coparison One PagerLakshmikanth SNo ratings yet
- Bacterial Meningitis in Children Older Than One MonthDocument23 pagesBacterial Meningitis in Children Older Than One MonthMario Mendoza TorresNo ratings yet
- Legal Considerations of Maternal and Child PracticeDocument22 pagesLegal Considerations of Maternal and Child PracticeChari RivoNo ratings yet
- Zeel P InformationsDocument2 pagesZeel P InformationscosmynnsNo ratings yet
- Keratitis PPT 1 SUB ENGLISHDocument33 pagesKeratitis PPT 1 SUB ENGLISHarif rhNo ratings yet
- Bac - A Healthy Dose of LaughterDocument3 pagesBac - A Healthy Dose of LaughterBen Hussa100% (2)
- Delaware Technical and Community CollegeDocument6 pagesDelaware Technical and Community Collegeapi-384152992No ratings yet
- Good Practice 12 Patient HandoverDocument4 pagesGood Practice 12 Patient HandoverDewi Ratna SariNo ratings yet
- Nursing EssayDocument12 pagesNursing Essayzee jay100% (1)
- Medical Surgical Questions LiverDocument17 pagesMedical Surgical Questions LiverHasan A AsFourNo ratings yet







































































































Download as pptx, pdf, or txt
You might also like
- Introduction To The Philosophy of The Human PersonDocument24 pagesIntroduction To The Philosophy of The Human Personbethuel100% (2)
- Intern Log Book JazanUDocument41 pagesIntern Log Book JazanUdrstrao100% (1)
- Shen 2018Document12 pagesShen 2018Muhammad Yusuf HanifNo ratings yet
- Brief T.B. Control ProgrammeDocument3 pagesBrief T.B. Control ProgrammeAbdullah AfzalNo ratings yet
- 1 s2.0 S0006497121006340 MainDocument13 pages1 s2.0 S0006497121006340 Mainresi silviaNo ratings yet
- CCO Clin Onc June 2019 504Document13 pagesCCO Clin Onc June 2019 504bingqi xuNo ratings yet
- Therapy: Non-Pharmacologic: y Z X Z Z Z y KDocument1 pageTherapy: Non-Pharmacologic: y Z X Z Z Z y KsondiNo ratings yet
- Self-Collected Extra-Genital Gonorrhea and Chlamydia Testing For MSMDocument13 pagesSelf-Collected Extra-Genital Gonorrhea and Chlamydia Testing For MSMGuilherme SttelletNo ratings yet
- Laproscopic Omental Patch For Perforated Peptic Ulcer Disease 1Document26 pagesLaproscopic Omental Patch For Perforated Peptic Ulcer Disease 1Sagor Kumar DasNo ratings yet
- 2019 Preceptorship H N TNM Classification 8th Edition Jean Pascal MachielsDocument36 pages2019 Preceptorship H N TNM Classification 8th Edition Jean Pascal MachielsGalgalo GarbichaNo ratings yet
- Comprehensive Management of Prostate Cancer 20150821Document30 pagesComprehensive Management of Prostate Cancer 20150821Marhama FitrianiNo ratings yet
- FLAD1 Is Up-Regulated in Gastric Cancer and Is A Potential Prediction of PrognosisDocument10 pagesFLAD1 Is Up-Regulated in Gastric Cancer and Is A Potential Prediction of PrognosisAriani ArinNo ratings yet
- Honey Bees and Also Untamed Pollinators Vary Within Their Desire Regarding and Employ of Presented Flower Sourceshlwhg PDFDocument1 pageHoney Bees and Also Untamed Pollinators Vary Within Their Desire Regarding and Employ of Presented Flower Sourceshlwhg PDFlowtimer98No ratings yet
- 1 s2.0 S1120179718301078 MainDocument1 page1 s2.0 S1120179718301078 MainAdeola AshiruNo ratings yet
- JTCVS 2004 - Wright 2004Document9 pagesJTCVS 2004 - Wright 2004vinicius.alvarez3No ratings yet
- #40 Status of The Thyroid Ultrasound Examination Results (January 15, 2021)Document6 pages#40 Status of The Thyroid Ultrasound Examination Results (January 15, 2021)Yuri HiranumaNo ratings yet
- Huh Et Al-2010-Journal of Surgical OncologyDocument5 pagesHuh Et Al-2010-Journal of Surgical OncologyFieska AzizahNo ratings yet
- RX PDFDocument3 pagesRX PDFMASIEL AMELIA BARRANTES ARCENo ratings yet
- Jurnal Reading Dermatitis Kontak Iritan: Ahmad Amsori Yuli Darlinawati Pembimbing: Dr. Arif Effendi, SP - KKDocument17 pagesJurnal Reading Dermatitis Kontak Iritan: Ahmad Amsori Yuli Darlinawati Pembimbing: Dr. Arif Effendi, SP - KKAhmad AmsoryNo ratings yet
- Kol Slide Kit Atac 100Document43 pagesKol Slide Kit Atac 100api-26302710No ratings yet
- Assessment of Clinician Accuracy For Diagnosing MeDocument3 pagesAssessment of Clinician Accuracy For Diagnosing MeYilianeth Mena DazaNo ratings yet
- DAPA-HF and DELIVER Pooled Meta-Analysis. Nature Med. 2022 - With VEEVADocument16 pagesDAPA-HF and DELIVER Pooled Meta-Analysis. Nature Med. 2022 - With VEEVAzdmoorNo ratings yet
- Artículo Ca PróstataDocument12 pagesArtículo Ca PróstataEddy AuzNo ratings yet
- FTPDocument5 pagesFTPHaya RihanNo ratings yet
- HOI160023supp1 Prod PDFDocument10 pagesHOI160023supp1 Prod PDFcassieNo ratings yet
- Annie Anderson Obesity The Elephant in The RoomDocument18 pagesAnnie Anderson Obesity The Elephant in The RoomVignesh JayaNo ratings yet
- Stampede M0 ASTRO Presentation Sept 2014Document24 pagesStampede M0 ASTRO Presentation Sept 2014Prof_Nick_JamesNo ratings yet
- Ujian Metris II - HerikaDocument14 pagesUjian Metris II - HerikaErie MoetzNo ratings yet
- #41 Status of The Thyroid Ultrasound Examination Results (May 17, 2021)Document6 pages#41 Status of The Thyroid Ultrasound Examination Results (May 17, 2021)Yuri HiranumaNo ratings yet
- Stent For Malignant Large Bowl ObstructionDocument6 pagesStent For Malignant Large Bowl ObstructionAndrei ZbucheaNo ratings yet
- Sex Transm Infect. 2011 Aug 87 (5) 385-8Document6 pagesSex Transm Infect. 2011 Aug 87 (5) 385-8Cynthia Patricia Manotas AltamarNo ratings yet
- Comparison Between Fine Needle Aspiration and Core Needle Biopsy For The Diagnosis of Thyroid Nodules: Effective Indications According To US FindingsDocument7 pagesComparison Between Fine Needle Aspiration and Core Needle Biopsy For The Diagnosis of Thyroid Nodules: Effective Indications According To US FindingsRama DanusNo ratings yet
- ASTRO23Slides VanasDocument18 pagesASTRO23Slides Vanasjohapatino46No ratings yet
- Essay Komstat Farhan HF RahmanDocument5 pagesEssay Komstat Farhan HF RahmantaufikramadhaniNo ratings yet
- Randomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast CancerDocument14 pagesRandomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast Canceralberto cabelloNo ratings yet
- #42 Status of The Thyroid Ultrasound Examination Results (July 27, 2021)Document6 pages#42 Status of The Thyroid Ultrasound Examination Results (July 27, 2021)Yuri HiranumaNo ratings yet
- Abstracts From The Global Embolization Sympo 2021 Journal of Vascular and inDocument21 pagesAbstracts From The Global Embolization Sympo 2021 Journal of Vascular and infreedy freedyNo ratings yet
- Prognostic Value of Ki-67 For Prostate Cancer Death in A Conservatively Managed CohortDocument7 pagesPrognostic Value of Ki-67 For Prostate Cancer Death in A Conservatively Managed Cohorthuu2toanNo ratings yet
- M7. MIII. O6a. Screening de CADocument29 pagesM7. MIII. O6a. Screening de CARogerio FernandesNo ratings yet
- Comparative Effectiveness Study of Single High-Dose Cisplatin WithDocument19 pagesComparative Effectiveness Study of Single High-Dose Cisplatin WithGentek PharmaNo ratings yet
- Management and Prognosis of Pancreatic Cancer Over A 30-Year PeriodDocument4 pagesManagement and Prognosis of Pancreatic Cancer Over A 30-Year PeriodAxelle BoukambaNo ratings yet
- Articol Extenso 2Document4 pagesArticol Extenso 2David CalinNo ratings yet
- CNCR 29602Document8 pagesCNCR 29602Joseph PerezNo ratings yet
- Khan SlidesDocument17 pagesKhan Slidesalberto cabelloNo ratings yet
- 4-Pres-Sardjito-Prof. Dr. Djaswadi Dasuki - M.ph. - PhD. - SpOGDocument12 pages4-Pres-Sardjito-Prof. Dr. Djaswadi Dasuki - M.ph. - PhD. - SpOGLukas Anjar KrismulyonoNo ratings yet
- #46 Status of The Thyroid Ultrasound Examination Results (Released On December 2, 2022)Document7 pages#46 Status of The Thyroid Ultrasound Examination Results (Released On December 2, 2022)Yuri HiranumaNo ratings yet
- Applying Data-Driven Imaging Biomarker in Mammography For Breast Cancer Screening: Preliminary StudyDocument8 pagesApplying Data-Driven Imaging Biomarker in Mammography For Breast Cancer Screening: Preliminary StudyDébora XavierNo ratings yet
- Establishment and Validation of PrognosticDocument10 pagesEstablishment and Validation of PrognosticMiss AmyNo ratings yet
- EARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDDocument31 pagesEARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDHengky TanNo ratings yet
- #43 Status of The Thyroid Ultrasound Examination Results (October 15, 2021)Document6 pages#43 Status of The Thyroid Ultrasound Examination Results (October 15, 2021)Yuri HiranumaNo ratings yet
- An Example of Propensity Score Matched ADocument10 pagesAn Example of Propensity Score Matched A古寒州No ratings yet
- MCHA022 (Analytical Chemistry 2)Document62 pagesMCHA022 (Analytical Chemistry 2)Mbali MazongweNo ratings yet
- Icmcrj 1 1011Document8 pagesIcmcrj 1 1011Shivaramakrishna SriramojuNo ratings yet
- Marshall 2007Document25 pagesMarshall 2007Allan Amaral da HoraNo ratings yet
- 727 Final+CommentsDocument14 pages727 Final+CommentsRahimSMCSwatNo ratings yet
- #44 Status of The Thyroid Ultrasound Examination Results (May 13, 2022)Document7 pages#44 Status of The Thyroid Ultrasound Examination Results (May 13, 2022)Yuri HiranumaNo ratings yet
- VEGF Expression in Colorectal Cancer Metastatic LyDocument14 pagesVEGF Expression in Colorectal Cancer Metastatic LyNana LianaNo ratings yet
- Pestana, 2022Document4 pagesPestana, 2022prof.rodrigopestanaNo ratings yet
- Journal Pone 0106203 PDFDocument7 pagesJournal Pone 0106203 PDFAnonymous 4vrma12QgbNo ratings yet
- PresentationDocument15 pagesPresentationSatish SinghNo ratings yet
- Supervised Classification Techniques and Deep Learning For Mortality Prediction in Sepsis PatientsDocument6 pagesSupervised Classification Techniques and Deep Learning For Mortality Prediction in Sepsis PatientsFabian Alberto Jaimes BarraganNo ratings yet
- First Hrpta MeetingDocument4 pagesFirst Hrpta MeetingbethuelNo ratings yet
- SF2 - NovemberDocument9 pagesSF2 - NovemberbethuelNo ratings yet
- HGP Eportfolio Editable 2022 2023Document34 pagesHGP Eportfolio Editable 2022 2023bethuelNo ratings yet
- Perdev-Dll-Aug. 29-Sept 2, 2022Document3 pagesPerdev-Dll-Aug. 29-Sept 2, 2022bethuelNo ratings yet
- Perdev Sept 5 - Sept 9, 2022Document3 pagesPerdev Sept 5 - Sept 9, 2022bethuelNo ratings yet
- Emotions ActivityDocument18 pagesEmotions ActivitybethuelNo ratings yet
- Manual Blood Pressure Competency ChecklistDocument1 pageManual Blood Pressure Competency ChecklistbethuelNo ratings yet
- Perdev Sept 12-16, 2022Document4 pagesPerdev Sept 12-16, 2022bethuelNo ratings yet
- Introduction To The Philosophy of The Human Person: Quarter 2 - Module 3Document20 pagesIntroduction To The Philosophy of The Human Person: Quarter 2 - Module 3bethuelNo ratings yet
- PD DLL March 06 10 2017Document3 pagesPD DLL March 06 10 2017bethuelNo ratings yet
- Introduction To The Philosophy of The Human Person: Quarter 2 - Module 4bDocument21 pagesIntroduction To The Philosophy of The Human Person: Quarter 2 - Module 4bbethuel100% (1)
- Final DLL Q1Document43 pagesFinal DLL Q1bethuelNo ratings yet
- Introduction To The Philosophy of The Human Person: Quarter 2 - Module 5Document19 pagesIntroduction To The Philosophy of The Human Person: Quarter 2 - Module 5bethuel100% (3)
- Sports Track 11: 2 Semester - Module 2b: Safety and First AidDocument18 pagesSports Track 11: 2 Semester - Module 2b: Safety and First AidbethuelNo ratings yet
- Matthias Rath Cancer Book - Vitamin C and Lysine For Cancer TreatmentDocument40 pagesMatthias Rath Cancer Book - Vitamin C and Lysine For Cancer TreatmentEbook PDF100% (3)
- Neural Tube Defects (Anatomy)Document11 pagesNeural Tube Defects (Anatomy)nur athiraNo ratings yet
- AlfanoDocument3 pagesAlfanoapi-532399186No ratings yet
- PPE and DrapesDocument27 pagesPPE and DrapesBang Tut ChuolNo ratings yet
- Cleaning+Standards+2021 v1.0+ (Revised+final)Document48 pagesCleaning+Standards+2021 v1.0+ (Revised+final)ابراهيم الحربيNo ratings yet
- Nurs 479 Professional DevelopmentDocument12 pagesNurs 479 Professional Developmentapi-490209035No ratings yet
- Mri Request FormDocument1 pageMri Request Formraad_alghamdi_1No ratings yet
- Form006 Survey Internship Student EvaluationDocument4 pagesForm006 Survey Internship Student Evaluationalexis tamayoNo ratings yet
- El Proyecto de InglesDocument3 pagesEl Proyecto de Ingleskim jojoNo ratings yet
- Batuk Dengan Atau Tanpa Sesak Nafas: DR Ari Kurniasih M, Ked (Ped), SpaDocument27 pagesBatuk Dengan Atau Tanpa Sesak Nafas: DR Ari Kurniasih M, Ked (Ped), Spacitra dewiNo ratings yet
- Drug Scenario in The PhilippinesDocument15 pagesDrug Scenario in The PhilippinesCalix GonzalesNo ratings yet
- Water Supply and Sanitation in IndiaDocument6 pagesWater Supply and Sanitation in IndiaMunish Dogra50% (2)
- Biomedical Ethics and Qawaid FiqhiyyahDocument12 pagesBiomedical Ethics and Qawaid FiqhiyyahSurgeon AsimNo ratings yet
- Clinical: ResearchDocument13 pagesClinical: ResearchAahil SumairNo ratings yet
- RLE Activity 1 - An Overview of MY COMMUNITY (Vizconde, Ehreiz Raiden C. BSN3-A)Document2 pagesRLE Activity 1 - An Overview of MY COMMUNITY (Vizconde, Ehreiz Raiden C. BSN3-A)Raiden VizcondeNo ratings yet
- 141 02Document8 pages141 02Shanty AnitaNo ratings yet
- Lab 7Document28 pagesLab 7Dave OrlandoNo ratings yet
- 180-SCF-3314 - Job DescriptionDocument17 pages180-SCF-3314 - Job DescriptionUmair AshfaqNo ratings yet
- Unit 1 Definitions/key Terms Varcarolis Mental Health NursingDocument6 pagesUnit 1 Definitions/key Terms Varcarolis Mental Health Nursingatl_nurse_studentNo ratings yet
- FHO, CHI, WC, ASSURE, Coparison One PagerDocument1 pageFHO, CHI, WC, ASSURE, Coparison One PagerLakshmikanth SNo ratings yet
- Bacterial Meningitis in Children Older Than One MonthDocument23 pagesBacterial Meningitis in Children Older Than One MonthMario Mendoza TorresNo ratings yet
- Legal Considerations of Maternal and Child PracticeDocument22 pagesLegal Considerations of Maternal and Child PracticeChari RivoNo ratings yet
- Zeel P InformationsDocument2 pagesZeel P InformationscosmynnsNo ratings yet
- Keratitis PPT 1 SUB ENGLISHDocument33 pagesKeratitis PPT 1 SUB ENGLISHarif rhNo ratings yet
- Bac - A Healthy Dose of LaughterDocument3 pagesBac - A Healthy Dose of LaughterBen Hussa100% (2)
- Delaware Technical and Community CollegeDocument6 pagesDelaware Technical and Community Collegeapi-384152992No ratings yet
- Good Practice 12 Patient HandoverDocument4 pagesGood Practice 12 Patient HandoverDewi Ratna SariNo ratings yet
- Nursing EssayDocument12 pagesNursing Essayzee jay100% (1)
- Medical Surgical Questions LiverDocument17 pagesMedical Surgical Questions LiverHasan A AsFourNo ratings yet