Download as ppt, pdf, or txt
You might also like
- 3.1.3.2 - HeadacheDocument40 pages3.1.3.2 - HeadacheaddinaNo ratings yet
- HeadacheDocument33 pagesHeadacheMpanso Ahmad AlhijjNo ratings yet
- Neurological DiseasesDocument91 pagesNeurological Diseasesrabia khalidNo ratings yet
- Diagnoses and Management Acute Headache Emergency DepartmentDocument37 pagesDiagnoses and Management Acute Headache Emergency DepartmentBendy Dwi IrawanNo ratings yet
- Cefaleas 2018Document87 pagesCefaleas 2018Anonimo DesconocidoNo ratings yet
- Headache & Migraine DrugsDocument59 pagesHeadache & Migraine Drugsjoshua katunziNo ratings yet
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadisradiologi igdNo ratings yet
- Headache Brunner and Suddarth Ed 12Document6 pagesHeadache Brunner and Suddarth Ed 12jaberfaithbayanganNo ratings yet
- Headac HE: Chapter 21, Harrison'S Internal MedicineDocument21 pagesHeadac HE: Chapter 21, Harrison'S Internal MedicineFernando AnibanNo ratings yet
- Review NeuroDocument48 pagesReview NeuroNefrologia SamaritanaNo ratings yet
- Pediatric Neurology BAUDocument56 pagesPediatric Neurology BAUمجاهد أسعدNo ratings yet
- Headaches: Jonalyn Sotero-Esco, RNDocument40 pagesHeadaches: Jonalyn Sotero-Esco, RNJoni Lyn Ba-as BayengNo ratings yet
- MigraineDocument9 pagesMigraineMr VoralpenNo ratings yet
- Headache 2Document21 pagesHeadache 2geeeelzy07No ratings yet
- Diskusi Topik (Sakit Kepala) - Nafisa Zulpa Elhapidi-406202067Document34 pagesDiskusi Topik (Sakit Kepala) - Nafisa Zulpa Elhapidi-406202067nafisa zulfaelNo ratings yet
- Writing Committee:: Guidelines For All Doctors in The Diagnosis and Management of Migraine and Tension-Type Headache 2004Document53 pagesWriting Committee:: Guidelines For All Doctors in The Diagnosis and Management of Migraine and Tension-Type Headache 2004Yan Agus AchtiarNo ratings yet
- Headache - Approach To The Adult PatientDocument52 pagesHeadache - Approach To The Adult PatientfjnaressiNo ratings yet
- HeadachesDocument96 pagesHeadachesMelakuNo ratings yet
- 4 HeadacheDocument33 pages4 HeadacheNathaniel BudayNo ratings yet
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadishemanthshah2801No ratings yet
- By: Negesse T. (M.SC, N) : Management of Patient With Neurologic DysfunctionDocument53 pagesBy: Negesse T. (M.SC, N) : Management of Patient With Neurologic DysfunctionErsido SamuelNo ratings yet
- Headache: Presented by Vallavan Narendra PrasadDocument15 pagesHeadache: Presented by Vallavan Narendra Prasadmiguel mendezNo ratings yet
- HeadachesDocument37 pagesHeadachesHafiz Muhammad AeymonNo ratings yet
- Common Presentation in Primary Care Clinic - Acute IllnessDocument112 pagesCommon Presentation in Primary Care Clinic - Acute IllnessSyahmi SuhaimiNo ratings yet
- 1 Neuropsychiatry of HeadacheDocument6 pages1 Neuropsychiatry of HeadachepriyadikkalaNo ratings yet
- Headache NotesDocument25 pagesHeadache NotesAin AmanyNo ratings yet
- MigraineDocument30 pagesMigraineFathimathNo ratings yet
- Neuro Dr. RehabDocument142 pagesNeuro Dr. RehabMohammed Saad NabhanNo ratings yet
- Ukdi Preparation I:: Neurogenic Pain Syndromes Peripheral Nerve DisordersDocument65 pagesUkdi Preparation I:: Neurogenic Pain Syndromes Peripheral Nerve DisordersFelicia SutarliNo ratings yet
- Headache: Migraine and Tension-Type HeadacheDocument12 pagesHeadache: Migraine and Tension-Type HeadacheLoren SangalangNo ratings yet
- Neurolgy 2Document92 pagesNeurolgy 2Noura RihanNo ratings yet
- How Do I Diagnose Headache?: P AperDocument7 pagesHow Do I Diagnose Headache?: P Apervii05No ratings yet
- HeadachesDocument42 pagesHeadachesAulia RahmiNo ratings yet
- Headache: Assoc Professor Dr. VinothiniDocument27 pagesHeadache: Assoc Professor Dr. VinothiniVivienneNo ratings yet
- (Puspaa) HeadacheDocument93 pages(Puspaa) HeadachePuspaa BhusalNo ratings yet
- Pharmacotherapy of Headache DisorderDocument61 pagesPharmacotherapy of Headache Disordersocialservice1012No ratings yet
- Nama: Muhammad Akbar - PendidikanDocument99 pagesNama: Muhammad Akbar - PendidikanAdekresnaHernataNo ratings yet
- Headaches: Prof. Dr. Basjiruddin Ahmad, SP.S (K) Fakultas Kedokteran Universitas Andalas RS. Dr. M. Djamil PadangDocument44 pagesHeadaches: Prof. Dr. Basjiruddin Ahmad, SP.S (K) Fakultas Kedokteran Universitas Andalas RS. Dr. M. Djamil PadangPutri MiraaNo ratings yet
- Approach To HeadacheDocument49 pagesApproach To Headachegea pandhita sNo ratings yet
- Primary Headache Secondary HeadacheDocument5 pagesPrimary Headache Secondary HeadacheYolanda Dwi OktaviyaniNo ratings yet
- Primary Headache: Mohamad Dawoud 6 Course Kharkiv National Medical UniversityDocument17 pagesPrimary Headache: Mohamad Dawoud 6 Course Kharkiv National Medical UniversityMhamad DawoudNo ratings yet
- Headache: Dep. of Neurology, General Hospital of Ningxia Medical University Cell Phone:13709599000Document50 pagesHeadache: Dep. of Neurology, General Hospital of Ningxia Medical University Cell Phone:13709599000ArvindhanNo ratings yet
- 4 Headache Undergrad 2020Document21 pages4 Headache Undergrad 2020b24trrznnrNo ratings yet
- Therapy of Migraine: An Overview: By-Parul Dixit Iind Trimester, M.Pharm (Pharmacology), SPTM, NmimsDocument29 pagesTherapy of Migraine: An Overview: By-Parul Dixit Iind Trimester, M.Pharm (Pharmacology), SPTM, NmimsParul DixitNo ratings yet
- HeadacheDocument46 pagesHeadacheIyas JehadNo ratings yet
- Cluster HeadacheDocument34 pagesCluster HeadacheRapid MedicineNo ratings yet
- S7 - Nervous SystemDocument22 pagesS7 - Nervous Systemyouservezeropurpose113No ratings yet
- Basic Overview of NeurologyDocument45 pagesBasic Overview of NeurologyDith Rivelta CallahanthNo ratings yet
- Prodromal - Aura - Nyeri Kepala - PostdormalDocument15 pagesProdromal - Aura - Nyeri Kepala - PostdormalangelinaNo ratings yet
- CVA or StrokeDocument14 pagesCVA or StrokeJoenalyn AliguinNo ratings yet
- Headache Evaluation & Treatment 2014Document47 pagesHeadache Evaluation & Treatment 2014UmairohSetengahTigaNo ratings yet
- Pemicu 6 Blok Saraf Dan KejiwaanDocument44 pagesPemicu 6 Blok Saraf Dan KejiwaanTommy WidjajaNo ratings yet
- Department of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaDocument106 pagesDepartment of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaSuba Saravanan 12No ratings yet
- 4th Problem Emergency Medicine Group 1Document82 pages4th Problem Emergency Medicine Group 1Jonathan TandajuNo ratings yet
- Neurologic Disorders Part 3Document72 pagesNeurologic Disorders Part 3Aly RiveraNo ratings yet
- NeurologyDocument42 pagesNeurologyPierre BenardNo ratings yet
- Pemicu 1: Blok Sistem Saraf Dan KejiwaanDocument50 pagesPemicu 1: Blok Sistem Saraf Dan KejiwaancecilliacynthiaNo ratings yet
- A Guide to Headaches and Migraines: Symptoms; Causes; Treatment; PreventionFrom EverandA Guide to Headaches and Migraines: Symptoms; Causes; Treatment; PreventionNo ratings yet
- Trigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesFrom EverandTrigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesNo ratings yet
- Cardiology (1) Nplex ReviewDocument55 pagesCardiology (1) Nplex ReviewValeria AcevedoNo ratings yet
- Clinical Infectious Disease Nplex ReviewDocument64 pagesClinical Infectious Disease Nplex ReviewValeria AcevedoNo ratings yet
- Gynecology Nplex ReviewDocument45 pagesGynecology Nplex ReviewValeria AcevedoNo ratings yet
- Hematology Oncology Nplex ReviewDocument46 pagesHematology Oncology Nplex ReviewValeria AcevedoNo ratings yet
- Endocrinology: Nplex Review Kimberly Sanders, NDDocument37 pagesEndocrinology: Nplex Review Kimberly Sanders, NDValeria AcevedoNo ratings yet
- Emergency Medicine ReviewDocument97 pagesEmergency Medicine ReviewValeria AcevedoNo ratings yet
- NPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesDocument83 pagesNPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesValeria AcevedoNo ratings yet
- Allreports Aspx PDFDocument3 pagesAllreports Aspx PDFAlNo ratings yet
- Case Study Final AsthmaDocument6 pagesCase Study Final AsthmaRichelle Sandriel C. de CastroNo ratings yet
- Casumpang v. Cortejo DigestDocument2 pagesCasumpang v. Cortejo DigestLucky P. RiveraNo ratings yet
- Chairside Guide Staging and Grading PeriodontitisDocument2 pagesChairside Guide Staging and Grading PeriodontitisMuhammad Hassan memonNo ratings yet
- Spinal Cord Injury Desk Reference Guidelines For LDocument2 pagesSpinal Cord Injury Desk Reference Guidelines For LLuna Begines FernándezNo ratings yet
- Communicable DiseaseDocument9 pagesCommunicable DiseaseSusan HepziNo ratings yet
- Miliaria, Leucoplakia, PPPDocument44 pagesMiliaria, Leucoplakia, PPPcuteNo ratings yet
- Braden Q Scale:: Intensity and Duration of Pressure ScoreDocument1 pageBraden Q Scale:: Intensity and Duration of Pressure Scoresholihatul fuadahNo ratings yet
- Module 8-NSTP 1-Health Program, Common Illness & Their PreventionDocument46 pagesModule 8-NSTP 1-Health Program, Common Illness & Their PreventionLalaine AlonNo ratings yet
- Radiotherapy For Colorectal CancerDocument28 pagesRadiotherapy For Colorectal CancerIndonesian Journal of CancerNo ratings yet
- Fig psychiatricAssessmentFormDocument3 pagesFig psychiatricAssessmentFormPatricia Eunise HerañaNo ratings yet
- Arianna Mabunga Bsn-3BDocument7 pagesArianna Mabunga Bsn-3BArianna Jasmine MabungaNo ratings yet
- Obesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaDocument8 pagesObesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaIJAR JOURNALNo ratings yet
- Sigtrans20162 7608Document9 pagesSigtrans20162 7608Emalaith BlackburnNo ratings yet
- Pathophys RespDocument38 pagesPathophys RespSabrina LavegaNo ratings yet
- Cardiac Tamponade, Also Known As Pericardial Tamponade, Is AnDocument7 pagesCardiac Tamponade, Also Known As Pericardial Tamponade, Is AnSimran Josan100% (1)
- Vaccine: Contents Lists Available atDocument9 pagesVaccine: Contents Lists Available atShabrina Amalia SuciNo ratings yet
- Guideline Perkeni 2019Document29 pagesGuideline Perkeni 2019Mradipta Arrya MNo ratings yet
- 1763 Pathology Question BankDocument5 pages1763 Pathology Question BankAkash js Akash jsNo ratings yet
- Maharastra University of Health Sciences, Nashik: III M.B.B.S. MedicineDocument96 pagesMaharastra University of Health Sciences, Nashik: III M.B.B.S. Medicineanant_nimkar9243No ratings yet
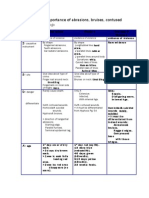
- Medico-Legal Importance of WoundsDocument3 pagesMedico-Legal Importance of Woundsapi-383014680% (5)
- Leuk OrrheaDocument6 pagesLeuk Orrheababon3No ratings yet
- 89 91Document15 pages89 91Victorine Levana PudjiadiNo ratings yet
- SLIDE Scoliosis SRSDocument48 pagesSLIDE Scoliosis SRSAnonymous x2OJJmi9Z100% (2)
- READING ON Tick-Borne DiseasesDocument3 pagesREADING ON Tick-Borne DiseasesMonique LeonardoNo ratings yet
- Fitrilya A.C.D.S 2018012258Document3 pagesFitrilya A.C.D.S 2018012258FitrilyaacdsNo ratings yet
- Blood Glucose MonitoringDocument20 pagesBlood Glucose Monitoringask1400100% (1)
- Article 21 - Bone Marrow TransplantDocument2 pagesArticle 21 - Bone Marrow TransplantAjay Noronha-PillaiNo ratings yet
- World IBD Day Infographic 2019 PDFDocument1 pageWorld IBD Day Infographic 2019 PDFVasoRafaelaVakouftsiNo ratings yet
- ACL ReconstructionDocument21 pagesACL ReconstructionMeet ShahNo ratings yet