Download as ppt, pdf, or txt
You might also like
- NeuroinfecciónDocument19 pagesNeuroinfecciónfabio100% (1)
- Neisseria, MoraxellaDocument33 pagesNeisseria, MoraxellaShuler0071No ratings yet
- Pediatric Community-Acquired Pneumonia: Updated Guidelines Pediatric Community-Acquired Pneumonia: Updated GuidelinesDocument18 pagesPediatric Community-Acquired Pneumonia: Updated Guidelines Pediatric Community-Acquired Pneumonia: Updated GuidelinesugascribNo ratings yet
- Day 1 Typhoid Fever - ItableDocument42 pagesDay 1 Typhoid Fever - ItableRye CalderonNo ratings yet
- Streptococcal PharyngitisDocument19 pagesStreptococcal PharyngitisBimasenaNo ratings yet
- Febris TyphoidDocument20 pagesFebris Typhoidcahyo setiawanNo ratings yet
- Cefoperazone Sulbactam en RNDocument4 pagesCefoperazone Sulbactam en RNchieneralbaNo ratings yet
- Habits Are Some of The Strategies RecommendedDocument30 pagesHabits Are Some of The Strategies Recommendedmd.dascalescu2486No ratings yet
- DR Maurits - PNEUMONIA DIES NATALIS KG88 PDFDocument37 pagesDR Maurits - PNEUMONIA DIES NATALIS KG88 PDFdanang andi100% (1)
- Community Acquired Bacterial Meningitis in AdultsDocument45 pagesCommunity Acquired Bacterial Meningitis in AdultsDaniel Tettamanti MirandaNo ratings yet
- Streptococcal PharyngitisDocument28 pagesStreptococcal PharyngitissylviaNo ratings yet
- FeverDocument27 pagesFeverTilaye GebruNo ratings yet
- Urinary Tract Infection Diagnosis and ManagementDocument6 pagesUrinary Tract Infection Diagnosis and ManagementAmr BashaNo ratings yet
- Clinical Features: - Initial Symptoms in Patients With MeningitisDocument12 pagesClinical Features: - Initial Symptoms in Patients With Meningitisyuii_48No ratings yet
- Antibiotka PicuDocument4 pagesAntibiotka Picusunu rachmat100% (1)
- Clinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Document3 pagesClinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Joey CuayoNo ratings yet
- What Is The Appendix?: Symptoms of AppendicitisDocument6 pagesWhat Is The Appendix?: Symptoms of AppendicitisVonn Bryan CalumiaNo ratings yet
- Febrile Neutropenia: Dr. Abdelkareem Wedaa EltohamyDocument31 pagesFebrile Neutropenia: Dr. Abdelkareem Wedaa Eltohamyjehemir100% (1)
- Ventilator Associated Pneumonia TreatmentDocument43 pagesVentilator Associated Pneumonia Treatmentmkc71No ratings yet
- Pneumonia: Recent Evidence Based UpdatesDocument30 pagesPneumonia: Recent Evidence Based UpdatesAli AzamNo ratings yet
- Diagnosis & Treatment of Healthcare-Associated Pneumonia: Beyond The GuidelineDocument57 pagesDiagnosis & Treatment of Healthcare-Associated Pneumonia: Beyond The GuidelineKei MiyazakiNo ratings yet
- Cefazolin (Ancef ®) : D5W, NsDocument9 pagesCefazolin (Ancef ®) : D5W, Nsbabe5606No ratings yet
- Otite Si SinDocument29 pagesOtite Si Sinminerva_stanciuNo ratings yet
- Fever With A Focus in Well Looking Child Under 3 YrsDocument80 pagesFever With A Focus in Well Looking Child Under 3 YrsAnuradha RoopchandNo ratings yet
- Karin Ananditya Fazri 30101407217: Pembimbing: DR, Dian Indah Setyorini, SP - THT-KLDocument31 pagesKarin Ananditya Fazri 30101407217: Pembimbing: DR, Dian Indah Setyorini, SP - THT-KLVivie Tirany SoediroNo ratings yet
- Pediatric Hematology Oncology CaseDocument107 pagesPediatric Hematology Oncology CaseSayyed Ahmad KhursheedNo ratings yet
- Drug of Treatment For Meningitis: Penicillin Cefotaxime ResistantDocument5 pagesDrug of Treatment For Meningitis: Penicillin Cefotaxime ResistantNama BestNo ratings yet
- Empyema CPGDocument8 pagesEmpyema CPGLe Vu AnhNo ratings yet
- Pediatric Pharmacotherapy: CefipimeDocument9 pagesPediatric Pharmacotherapy: Cefipimeashfaq ahmedNo ratings yet
- H1N1 Clinician Guidance Final Version1Document2 pagesH1N1 Clinician Guidance Final Version1cha_cruz_6No ratings yet
- Klebsiella PDFDocument4 pagesKlebsiella PDFOscarEduardoNo ratings yet
- Management of Intra-Abdominal InfectionDocument65 pagesManagement of Intra-Abdominal InfectionKamran SherazNo ratings yet
- Fiebre Sin Foco Aparente 3 A 36 Meses DynaMedDocument41 pagesFiebre Sin Foco Aparente 3 A 36 Meses DynaMedAna Maria Guerron CabreraNo ratings yet
- CNS InfectionsDocument44 pagesCNS Infectionsfire_n_iceNo ratings yet
- DR Dhani Redono - Management Sepsis 6Document41 pagesDR Dhani Redono - Management Sepsis 6PraviyantiNo ratings yet
- Enteric FeverDocument35 pagesEnteric FeverTejinder SinghNo ratings yet
- Monitoring The Treatment of Sepsis With Vancomycin in Term Newborn InfantsDocument8 pagesMonitoring The Treatment of Sepsis With Vancomycin in Term Newborn InfantsCristiano CardosoNo ratings yet
- CefaclorsandozcapDocument9 pagesCefaclorsandozcapseagull70No ratings yet
- Joc 911151Document8 pagesJoc 911151Daniel BorgesNo ratings yet
- Sepsis in PregnancyDocument25 pagesSepsis in Pregnancysana khan008No ratings yet
- Pyogenic MeningitisDocument46 pagesPyogenic MeningitisShahnaaz ShahNo ratings yet
- Principles of Antibiotic TherapyDocument26 pagesPrinciples of Antibiotic TherapyHaroun drissNo ratings yet
- Hospital-Acquired Pneumonia (HAP) & Ventilator-Associated Pneumonia (VAP) Healthcare-Associated Pneumonia (HCAP)Document32 pagesHospital-Acquired Pneumonia (HAP) & Ventilator-Associated Pneumonia (VAP) Healthcare-Associated Pneumonia (HCAP)Kamel HadyNo ratings yet
- Nosocomial Pneumonia in AdultsDocument28 pagesNosocomial Pneumonia in AdultsAndrie WigunaNo ratings yet
- Pharmacotherapeutics-Ii Assignment: Submitted To Mrs. Rojeena Koju Shrestha Department of PharmacyDocument7 pagesPharmacotherapeutics-Ii Assignment: Submitted To Mrs. Rojeena Koju Shrestha Department of PharmacyAnish GhaleNo ratings yet
- Antimicrobial Therapy in Sepsis PDFDocument38 pagesAntimicrobial Therapy in Sepsis PDFTatik HandayaniNo ratings yet
- Fluconazole Versus Nystatin in The Prevention of CandidaDocument25 pagesFluconazole Versus Nystatin in The Prevention of CandidaMutia SesunanNo ratings yet
- JURNAL Cefaclor Vs Amoxicillin in The Treatment of AcuteDocument8 pagesJURNAL Cefaclor Vs Amoxicillin in The Treatment of Acuterichard gunturNo ratings yet
- Pediatric Pharyngitis (Sore Throat) : InfectiousDocument9 pagesPediatric Pharyngitis (Sore Throat) : InfectiousRudi Jazz RegobizNo ratings yet
- Pulmonary InfectionsDocument16 pagesPulmonary InfectionsFawad AhmedNo ratings yet
- Intra Abdominal 2009Document8 pagesIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNo ratings yet
- Infections of The Upper Genital TractDocument40 pagesInfections of The Upper Genital TractBernard Palarca SantosNo ratings yet
- Neonatal Sepsis: Prof DR Saima BatoolDocument31 pagesNeonatal Sepsis: Prof DR Saima BatoolSAIMA BATOOLNo ratings yet
- Ranicef Tablets Cefdinir Tablets 300MG FidsonDocument13 pagesRanicef Tablets Cefdinir Tablets 300MG FidsonWright JohnNo ratings yet
- Pharma URO CephalosporinsDocument20 pagesPharma URO CephalosporinsHussein AlhaddadNo ratings yet
- A Study On Ventilator Associated Pneumonia inDocument4 pagesA Study On Ventilator Associated Pneumonia inAl MuzakkiNo ratings yet
- Febrile Neutropenia 2Document35 pagesFebrile Neutropenia 2Okky Rizqika KamilNo ratings yet
- Management of PharyngotonsylitisDocument6 pagesManagement of PharyngotonsylitisAmeenu Isah HasheemNo ratings yet
- CephalosporinsDocument20 pagesCephalosporinsHussein AlhaddadNo ratings yet
- Pneumonia GuidelinesDocument4 pagesPneumonia GuidelinesFatkhul Ali ImronNo ratings yet
- Febrile Neutropenia ArunDocument40 pagesFebrile Neutropenia ArunArun GeorgeNo ratings yet
- Pedia CardsDocument40 pagesPedia CardsKristine Marie Santos100% (1)
- Taxonomy of OystersDocument50 pagesTaxonomy of OystersKristine Marie SantosNo ratings yet
- Cargos and Genes: Insights Into Vesicular Transport From Inherited Human DiseaseDocument23 pagesCargos and Genes: Insights Into Vesicular Transport From Inherited Human DiseaseKristine Marie SantosNo ratings yet
- Allelopathy Ppt. EditedDocument16 pagesAllelopathy Ppt. EditedKristine Marie Santos100% (3)
- Muscles of Felis Domestica-1Document17 pagesMuscles of Felis Domestica-1Kristine Marie SantosNo ratings yet
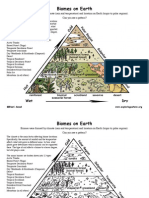
- Biome Locations PDFDocument2 pagesBiome Locations PDFKristine Marie SantosNo ratings yet
- Floral Formulas and DiagramsDocument25 pagesFloral Formulas and DiagramsSidra Sameen100% (1)
- Protocol LabDocument53 pagesProtocol LabKristine Marie SantosNo ratings yet
- Ingrain Dye Explantaion PDFDocument8 pagesIngrain Dye Explantaion PDFKristine Marie Santos100% (1)
- 6 Alcohols and Phenols PDFDocument7 pages6 Alcohols and Phenols PDFKristine Marie SantosNo ratings yet
- 001.final Group One Ass Survilance All in OneDocument43 pages001.final Group One Ass Survilance All in Onehabtamu birhanuNo ratings yet
- Causes and Treatment For MeningitisDocument21 pagesCauses and Treatment For MeningitisJoyce Suzzane HyuugaNo ratings yet
- Summary of Infectious DiseasesDocument415 pagesSummary of Infectious DiseasesAlston Foods BVNo ratings yet
- Collection of Systematic Bacteriology (Mansoura Dentistry)Document16 pagesCollection of Systematic Bacteriology (Mansoura Dentistry)elsayed barhomeNo ratings yet
- Child With Non Blanching RashDocument6 pagesChild With Non Blanching Rashtanya mathewNo ratings yet
- SDL-Bacterial Infections: Case 1 Group 3Document15 pagesSDL-Bacterial Infections: Case 1 Group 3Russell Talan CilotNo ratings yet
- Infectious DiseasesDocument62 pagesInfectious DiseasesakufahabaNo ratings yet
- Meningococcemia: Neisseria Meningitidis - Is An EncapsulatedDocument19 pagesMeningococcemia: Neisseria Meningitidis - Is An EncapsulatedcarolinecayasaNo ratings yet
- Electrical SafetyDocument11 pagesElectrical SafetyMoatasem AhmedNo ratings yet
- What Is MeningitisDocument10 pagesWhat Is MeningitisJoshua Capa FrondaNo ratings yet
- Meningitis (Completed)Document26 pagesMeningitis (Completed)seema83% (6)
- Ow Q 51-100 (14.11.09)Document102 pagesOw Q 51-100 (14.11.09)PradeepNo ratings yet
- Meningitis Pathophysiology PDFDocument59 pagesMeningitis Pathophysiology PDFpaswordnyalupa100% (1)
- Chairman of Poonawalla Group Which Includes Serum Institute of India EMDocument29 pagesChairman of Poonawalla Group Which Includes Serum Institute of India EMzufishaNo ratings yet
- Diagnostic Tests: Neisseria Meningitidis CapsularDocument2 pagesDiagnostic Tests: Neisseria Meningitidis CapsularCherry Mae JasoNo ratings yet
- Pediatric Meningitis Case StudyDocument5 pagesPediatric Meningitis Case StudyCheska PalomaNo ratings yet
- Communication Scenarios PDFDocument1,052 pagesCommunication Scenarios PDFDr AhmedNo ratings yet
- Meningitis - 2018Document55 pagesMeningitis - 2018Abraham Anaely100% (1)
- Bacteriology Edited 1Document65 pagesBacteriology Edited 1Ali AhmedNo ratings yet
- MeningitisDocument6 pagesMeningitisspicychips7No ratings yet
- NBHS2332 Learning KitDocument36 pagesNBHS2332 Learning Kitshinichi kudoNo ratings yet
- Bacterial Meningitis: Dr.T.V.Rao MDDocument70 pagesBacterial Meningitis: Dr.T.V.Rao MDSerque777No ratings yet
- Normal FloraDocument28 pagesNormal FloraMuhammad KashifNo ratings yet
- Communicable Disease PresentationDocument67 pagesCommunicable Disease PresentationMonaNo ratings yet
- Travel Medicine: Health Quarantine 2021 Dr. Esther Meylina SipahutarDocument35 pagesTravel Medicine: Health Quarantine 2021 Dr. Esther Meylina SipahutarEsther Meyline XhypaNo ratings yet
- Introduction, Case StudyDocument56 pagesIntroduction, Case StudyLeanna Cantanero67% (3)
- PIDSR Other DiseasesDocument45 pagesPIDSR Other DiseasesMichelle TuraNo ratings yet