Download as pptx, pdf, or txt
You might also like
- Organization of NICU ServicesDocument45 pagesOrganization of NICU ServicesMonika Bagchi84% (64)
- Astm E564Document5 pagesAstm E564Julio Cesar ValdiviesoNo ratings yet
- Current Principles Practices and Trends in PediaDocument3 pagesCurrent Principles Practices and Trends in PediaArchana Sahu100% (2)
- Assessment and Management of High Risk NeonateDocument14 pagesAssessment and Management of High Risk Neonatenitu_kalita392% (12)
- Newborn Adaptation FinalDocument28 pagesNewborn Adaptation Finalsanthiyasandy91% (11)
- Iugr FinalDocument35 pagesIugr Finalsanthiyasandy100% (4)
- Changing Trends in Paediatric NursingDocument25 pagesChanging Trends in Paediatric NursingGayatri Mudliyar71% (7)
- Live Video DatingDocument11 pagesLive Video DatingPhuc Pham XuanNo ratings yet
- Organisation of NicuDocument5 pagesOrganisation of NicuDelphy Varghese100% (4)
- CBLM Oap Ncii Core MCCDocument101 pagesCBLM Oap Ncii Core MCCmario layan100% (5)
- Organization of Neonatal Intensive Care Unit: Vanderbilt University Mildred Stahlman StahlmanDocument12 pagesOrganization of Neonatal Intensive Care Unit: Vanderbilt University Mildred Stahlman StahlmanKiran Kumar100% (1)
- Organization of NICU NotesDocument39 pagesOrganization of NICU NotesSobha ajo100% (2)
- Neonatal Heart DiseaseDocument8 pagesNeonatal Heart DiseaseDelphy VargheseNo ratings yet
- Uterine MalformationsDocument6 pagesUterine MalformationssubashikNo ratings yet
- Feeding of High Risk NeonatesDocument33 pagesFeeding of High Risk Neonatesannu panchal50% (6)
- Bordador Vs Luz DigestDocument2 pagesBordador Vs Luz DigestHazel Angeline Q. AbenojaNo ratings yet
- PT Oranization of Neonatal Care ServicesDocument10 pagesPT Oranization of Neonatal Care ServicesPragati BholeNo ratings yet
- Assignment On NicuDocument24 pagesAssignment On NicuRupali Arora67% (3)
- Organization of Neonatal Care ServicesDocument67 pagesOrganization of Neonatal Care ServicesArchana88% (8)
- Organization of A Neonatal Intensive Care UnitDocument30 pagesOrganization of A Neonatal Intensive Care UnitJaya Prabha90% (29)
- Peergroup Nicu OrganizationDocument17 pagesPeergroup Nicu OrganizationManisha ThakurNo ratings yet
- Nicu Physical LayoutDocument16 pagesNicu Physical LayoutMeena Koushal100% (5)
- Cpms College of Nursing Assignment ON Bilimeter: Subject: Child Health Nursing DATED:23 JUNE 2021Document5 pagesCpms College of Nursing Assignment ON Bilimeter: Subject: Child Health Nursing DATED:23 JUNE 2021Amy Lalringhluani Chhakchhuak100% (3)
- Newborn ProfileDocument92 pagesNewborn ProfilesarikaNo ratings yet
- Crisis and Nursing InterventionDocument44 pagesCrisis and Nursing InterventionArchana100% (4)
- Seminar 1 EXPANDED AND EXTENDED ROLE OF PEDIATRIC NURSEDocument15 pagesSeminar 1 EXPANDED AND EXTENDED ROLE OF PEDIATRIC NURSESuganthi Parthiban100% (7)
- Baby Friendly Hospital InitiativeDocument6 pagesBaby Friendly Hospital InitiativeBinal JoshiNo ratings yet
- Needs of Newborn MicroteachingDocument11 pagesNeeds of Newborn MicroteachingAnjali DasNo ratings yet
- History, Principle and Scope of CHNDocument39 pagesHistory, Principle and Scope of CHNArchana100% (1)
- Concept, Assessment, Goals, Objectives of High Risk NewbornDocument76 pagesConcept, Assessment, Goals, Objectives of High Risk NewbornEsha KuttiNo ratings yet
- Identification and Classification of Neonate With InfectionsDocument62 pagesIdentification and Classification of Neonate With Infectionsvisuinsvu100% (7)
- Preventive PediatricDocument15 pagesPreventive PediatricArchana100% (1)
- High-Risk NCM 102Document36 pagesHigh-Risk NCM 102EmmanuelL.TarucNo ratings yet
- Trends in The ObstetricsDocument12 pagesTrends in The ObstetricssuthaNo ratings yet
- Role of Pediatric Nurse in Child CareDocument4 pagesRole of Pediatric Nurse in Child Carevishnu100% (1)
- Administration of PICU Child Health NursingDocument37 pagesAdministration of PICU Child Health NursingJimcy100% (4)
- Physically ChallengedDocument8 pagesPhysically ChallengedUday Kumar100% (4)
- Psychological Complication in PuerperiumDocument17 pagesPsychological Complication in Puerperiumbaby67% (3)
- Icterus Neonatorum/ Jaundice: 07/12/2021 Rupinder DeolDocument83 pagesIcterus Neonatorum/ Jaundice: 07/12/2021 Rupinder DeolShivangi SharmaNo ratings yet
- Unwed MotherDocument3 pagesUnwed Motherjasmine904677% (13)
- Preventive Paediatric and Paediatric NursingDocument2 pagesPreventive Paediatric and Paediatric NursingHUSSAINA BANO100% (1)
- Advanced Neonatal ProceduresDocument43 pagesAdvanced Neonatal ProceduresKrupa Jyothirmai100% (1)
- Infection Control and Standard Safety MeasuresDocument25 pagesInfection Control and Standard Safety MeasuresManisha Thakur100% (1)
- Advanced Neonatal Procedures2Document14 pagesAdvanced Neonatal Procedures2Vijith.V.kumar100% (8)
- TOPIC - Management of Challenged ChildrenDocument20 pagesTOPIC - Management of Challenged ChildrenDinesh Khinchi75% (4)
- Common Neonatal DisordersDocument71 pagesCommon Neonatal DisordersRANJIT GOGOI100% (3)
- Training and Rehabilitation of Challenged ChildrenDocument3 pagesTraining and Rehabilitation of Challenged ChildrenSanthosh.S.U100% (2)
- Characteristics of NewbornDocument28 pagesCharacteristics of NewbornChandu Raj100% (4)
- UNIT I - Modern Concepts & Trends of Child Health CareDocument19 pagesUNIT I - Modern Concepts & Trends of Child Health CarevigneshNo ratings yet
- Icterus Neonatorum: Presented By: Ms. Sharon Vincent Ii Yr MSC NursingDocument38 pagesIcterus Neonatorum: Presented By: Ms. Sharon Vincent Ii Yr MSC Nursingvincentsharon100% (3)
- Current Principles, Practices and Trends in Pediatric: Father of Pediatrics Because of His ManyDocument4 pagesCurrent Principles, Practices and Trends in Pediatric: Father of Pediatrics Because of His ManyDaffodil Angel100% (1)
- Nicu DoccumentationDocument17 pagesNicu Doccumentationchaarvi100% (1)
- Essential Care of NewbornDocument36 pagesEssential Care of Newbornvikas tak100% (2)
- Administration and Management of PICU - Design, Layout, Staffing, Equipment's and SuppliesDocument27 pagesAdministration and Management of PICU - Design, Layout, Staffing, Equipment's and SuppliesAbinaya RanganathanNo ratings yet
- Seminar ON: Birth InjuriesDocument38 pagesSeminar ON: Birth Injuriesvishnu100% (1)
- Practice Standards For Obstetric and Gynaecological UnitDocument27 pagesPractice Standards For Obstetric and Gynaecological UnitRDi J100% (1)
- High Power CommitteeDocument9 pagesHigh Power CommitteeNissy Biju Varghese67% (3)
- Assignment ON Identification, Classification & Nursing Management of High Risk NewbornDocument18 pagesAssignment ON Identification, Classification & Nursing Management of High Risk NewbornSanthosh.S.U100% (1)
- Topic Prensentation ON: Kangaroo Mother CareDocument15 pagesTopic Prensentation ON: Kangaroo Mother Careamit100% (1)
- 13 Assignment-on-PhototherapyDocument11 pages13 Assignment-on-Phototherapyamit100% (6)
- Effect of Drug During Pregnancy, Labour and PuerperiumDocument10 pagesEffect of Drug During Pregnancy, Labour and PuerperiumSabeethu Girija63% (16)
- NicuDocument35 pagesNicuJaya Prabha100% (2)
- Organization of NICU ServicesDocument46 pagesOrganization of NICU ServicesamitNo ratings yet
- NICU Final EditedDocument58 pagesNICU Final EditedGandimarei100% (2)
- Psychiatric Disorders During PregnancyDocument28 pagesPsychiatric Disorders During PregnancyLamnunnem Haokip100% (1)
- Presentation Aids and HivDocument27 pagesPresentation Aids and HivLamnunnem HaokipNo ratings yet
- Clinical Teaching ProgrammeDocument28 pagesClinical Teaching ProgrammeLamnunnem HaokipNo ratings yet
- Augmentation of LabourDocument45 pagesAugmentation of LabourLamnunnem HaokipNo ratings yet
- Quiz 3 Fin II - Parte 2Document3 pagesQuiz 3 Fin II - Parte 2RicardoNo ratings yet
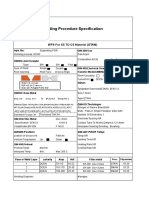
- Welding Procedure Specification: WPS For SS TO CS Material (GTAW)Document1 pageWelding Procedure Specification: WPS For SS TO CS Material (GTAW)Lipika GayenNo ratings yet
- Practical Examples On Database Management SystemsDocument9 pagesPractical Examples On Database Management SystemsReem Essam MohamedNo ratings yet
- Bar-Bench RelationDocument3 pagesBar-Bench RelationANJANA SHARMANo ratings yet
- Regional Rural BanksDocument6 pagesRegional Rural Banksdranita@yahoo.comNo ratings yet
- Negotiation Sub Process: Perception, Cognition and EmotionDocument4 pagesNegotiation Sub Process: Perception, Cognition and EmotionArti Das100% (1)
- Paging RRRDocument153 pagesPaging RRRMark EmakhuNo ratings yet
- ELS - Q1 - Week 4aDocument3 pagesELS - Q1 - Week 4apeterjo raveloNo ratings yet
- 2014-Db-Franck Pachot-Interpreting Awr Reports Straight To The Goal-ManuskriptDocument11 pages2014-Db-Franck Pachot-Interpreting Awr Reports Straight To The Goal-ManuskriptAnonymous OBPVTEuQLNo ratings yet
- 1St Business Strategy Assignment Brief 2018Document9 pages1St Business Strategy Assignment Brief 2018Quyên VũNo ratings yet
- IddqDocument66 pagesIddqRajasekharVenkataNo ratings yet
- United States v. Eric Millan, A/K/A Eric Millan Colon, A/K/A Eric Colon, A/K/A Luis Colon, A/K/A Ejay, A/K/A Moe Ralph Rivera, A/K/A Tj, A/K/A Rafael Rivera Vincent Basciano, A/K/A Vinnie Alfred v. Bottone, Sr., A/K/A Valentino A. Bottone, A/K/A Fat Al Alfred Bottone, Jr., A/K/A Alfie and Noel Melendez, Myles Coker Anthony Bottone Albert Biscaglio, A/K/A Allie John O'rourke, A/K/A Xyz Raimundo Hurdle, A/K/A Carlos Hurdly, A/K/A Panama William Mendoza, A/K/A Willie Porfipio Ortiz Mildred Hernandez Carmen Mendoza, A/K/A Belilo Samanta Torres and Larry Weinstein, A/K/A Larry Burns, 17 F.3d 14, 2d Cir. (1994)Document12 pagesUnited States v. Eric Millan, A/K/A Eric Millan Colon, A/K/A Eric Colon, A/K/A Luis Colon, A/K/A Ejay, A/K/A Moe Ralph Rivera, A/K/A Tj, A/K/A Rafael Rivera Vincent Basciano, A/K/A Vinnie Alfred v. Bottone, Sr., A/K/A Valentino A. Bottone, A/K/A Fat Al Alfred Bottone, Jr., A/K/A Alfie and Noel Melendez, Myles Coker Anthony Bottone Albert Biscaglio, A/K/A Allie John O'rourke, A/K/A Xyz Raimundo Hurdle, A/K/A Carlos Hurdly, A/K/A Panama William Mendoza, A/K/A Willie Porfipio Ortiz Mildred Hernandez Carmen Mendoza, A/K/A Belilo Samanta Torres and Larry Weinstein, A/K/A Larry Burns, 17 F.3d 14, 2d Cir. (1994)Scribd Government DocsNo ratings yet
- Carter Products Jet Bandsaw Guide Conversion Kit Installation InstructionsDocument2 pagesCarter Products Jet Bandsaw Guide Conversion Kit Installation Instructionstravis_gant3547No ratings yet
- Symex Security Services, Inc. vs. Rivera, JR., 844 SCRA 416, November 08, 2017Document28 pagesSymex Security Services, Inc. vs. Rivera, JR., 844 SCRA 416, November 08, 2017Catherine DimailigNo ratings yet
- 61 Spesifikasi PRIMAMED SCHWERT Dental Instrument Set For School-Kit UKGSDocument1 page61 Spesifikasi PRIMAMED SCHWERT Dental Instrument Set For School-Kit UKGSSarahNo ratings yet
- IRAS E-Tax Guide: Deductibility of "Keyman" Insurance PremiumsDocument8 pagesIRAS E-Tax Guide: Deductibility of "Keyman" Insurance PremiumsSampath VimalaNo ratings yet
- 8.building Analysis ModelDocument64 pages8.building Analysis ModeltierSargeNo ratings yet
- ChE 304 Exp 1Document20 pagesChE 304 Exp 1Sadia HasanNo ratings yet
- United States Court of Appeals For The Third CircuitDocument4 pagesUnited States Court of Appeals For The Third CircuitScribd Government DocsNo ratings yet
- Kellogg's New Product LaunchDocument4 pagesKellogg's New Product Launcharpita nayakNo ratings yet
- A Study On Employee Retention Strategies in Indian Manufacturing Industries - International Journal of Management Research and Social ScienceDocument5 pagesA Study On Employee Retention Strategies in Indian Manufacturing Industries - International Journal of Management Research and Social Sciencenandi durga98No ratings yet
- Central Bank v. Tolentino: 125 SCRA 122Document15 pagesCentral Bank v. Tolentino: 125 SCRA 122alyza burdeosNo ratings yet
- Values and Ethics BBA Unit 1Document23 pagesValues and Ethics BBA Unit 1Gayatri ChopraNo ratings yet
- ShockLog Essentials v10 4Document79 pagesShockLog Essentials v10 4William Rubio AvilaNo ratings yet
- Difference Betwn Gross Salary, CTCDocument8 pagesDifference Betwn Gross Salary, CTCabdulyunus_amirNo ratings yet
- Fundamentals of Information Systems PDFDocument164 pagesFundamentals of Information Systems PDFharshithaNo ratings yet