
MBBS - Blood Groups - 2020
MBBS - Blood Groups - 2020
You might also like
- RH and Abo IncompatibilityDocument10 pagesRH and Abo IncompatibilityamitNo ratings yet
- Guide To Fire Protection in MalaysiaDocument3 pagesGuide To Fire Protection in MalaysiaFadilah Ansari0% (2)
- Blood GroupsDocument38 pagesBlood GroupsVirendra JoshiNo ratings yet
- Lab 5Document22 pagesLab 5Aveen MustafaNo ratings yet
- RH IsoimmunizationDocument15 pagesRH Isoimmunizationgeorgeloto12No ratings yet
- Blood GroupDocument52 pagesBlood GroupShameena KnNo ratings yet
- Blood Types (Blood Groups) : Antigen (Agglutinogens)Document4 pagesBlood Types (Blood Groups) : Antigen (Agglutinogens)Khant Si ThuNo ratings yet
- Lecture10 - Blood Groups and TransfusionDocument28 pagesLecture10 - Blood Groups and Transfusionmohapatrarashmi050No ratings yet
- 12 - Blood GroupsDocument23 pages12 - Blood Groupsmohapatrarashmi050No ratings yet
- Blood BasicsDocument30 pagesBlood Basicskholoud220No ratings yet
- Blood Groups & CoagulationDocument12 pagesBlood Groups & CoagulationRAVI KANT PATELNo ratings yet
- ABO Grouping & RH FactorDocument3 pagesABO Grouping & RH FactorMadhurima PurkaitNo ratings yet
- BLOOD GROUPS MBBS.... MSK 3.9.18 LectureDocument37 pagesBLOOD GROUPS MBBS.... MSK 3.9.18 LectureJiyaa PatelNo ratings yet
- Bloodgroups 150424221954 Conversion Gate01Document38 pagesBloodgroups 150424221954 Conversion Gate01Endla SriniNo ratings yet
- Golongan Darah: Dr. Dr. Endang Sriwahyuni, MSDocument18 pagesGolongan Darah: Dr. Dr. Endang Sriwahyuni, MSDarma PutraNo ratings yet
- His 10Document2 pagesHis 10Kristin DouglasNo ratings yet
- 12 - Blood Groups and Blood Transfusion 2018Document27 pages12 - Blood Groups and Blood Transfusion 2018gimspath cme2022No ratings yet
- Blood GroubDocument21 pagesBlood Groubabdullahhassane299No ratings yet
- Blood GroupsDocument23 pagesBlood GroupsammarNo ratings yet
- Rhesus DiseaseDocument67 pagesRhesus DiseaseSalah EswaysiNo ratings yet
- Abo Blood RH GroupingDocument27 pagesAbo Blood RH GroupingJames Carbonell Dela PeñaNo ratings yet
- Abo Blood RH GroupingDocument22 pagesAbo Blood RH GroupingĐỗ Ngọc ÁnhNo ratings yet
- Hemolytic Diseases of The Fetus and NewbornDocument30 pagesHemolytic Diseases of The Fetus and Newbornkristine_camerinoNo ratings yet
- Blood Types & TransfusionDocument20 pagesBlood Types & TransfusionDr Imran AftabNo ratings yet
- BLOOD GROUPS TYPING - PowerpointDocument38 pagesBLOOD GROUPS TYPING - PowerpointJoy SNo ratings yet
- Blood TransfusionDocument28 pagesBlood Transfusionفيصل فهدNo ratings yet
- Blood TypingDocument11 pagesBlood Typingprakash gusainNo ratings yet
- The Blood Group Systems: Inheritance and GeneticsDocument34 pagesThe Blood Group Systems: Inheritance and GeneticsP Vinod Kumar100% (1)
- Genotype and Blood Group CompatibilityDocument5 pagesGenotype and Blood Group CompatibilityajayranjithNo ratings yet
- Blood Group NewDocument44 pagesBlood Group NewArpita SankhwarNo ratings yet
- RH Factor GeneticsDocument9 pagesRH Factor Geneticsbushra sajjadNo ratings yet
- Blood Group ND Transfusion - 231202 - 151259Document54 pagesBlood Group ND Transfusion - 231202 - 151259Archisman Mukherjee FAPSIANNo ratings yet
- Blood Group & RHDocument27 pagesBlood Group & RHfamtaluNo ratings yet
- TP Immunology English 2018 For StudentDocument83 pagesTP Immunology English 2018 For StudentKhaled Abo Al OyounNo ratings yet
- Blood Groups: Dr. Kenan GumustekinDocument43 pagesBlood Groups: Dr. Kenan Gumustekinsyed nomanshahNo ratings yet
- BBDocument6 pagesBBFrey Mary Dela PeñaNo ratings yet
- 1.blood GroupDocument38 pages1.blood GroupteraraNo ratings yet
- Bloog GroupDocument3 pagesBloog GroupChennai IbrahimNo ratings yet
- Blood Typing, Rhesus Factor, and BloodDocument40 pagesBlood Typing, Rhesus Factor, and BloodHalima IliyasuNo ratings yet
- Blood Grouping 1690574753Document30 pagesBlood Grouping 1690574753willowmaecayabyabNo ratings yet
- The Cardiovascular System 3Document17 pagesThe Cardiovascular System 3aboody62621No ratings yet
- ABO Blood Typing: Elrey L/ Navarro MD, DPCOMDocument42 pagesABO Blood Typing: Elrey L/ Navarro MD, DPCOMAnonymous 2TzM1Z100% (1)
- ABO and RH Blood Group SystemDocument31 pagesABO and RH Blood Group SystemKaab Ishaq100% (1)
- Blood GroupsDocument53 pagesBlood GroupsSneh KevadiyaNo ratings yet
- Blood Case 6Document12 pagesBlood Case 6إنعام الحفيانNo ratings yet
- Blood Groups and Blood Transfusion BioDocument23 pagesBlood Groups and Blood Transfusion BiowhyyoucareNo ratings yet
- Blood Group and Transfusion ReactionDocument15 pagesBlood Group and Transfusion ReactionAhmad KhanNo ratings yet
- RH SystemDocument22 pagesRH Systemhistorymonday10No ratings yet
- Abo and MN Blood Group SystemDocument54 pagesAbo and MN Blood Group SystemAkram chaudaryNo ratings yet
- Dr. Husnil Kadri, M.KesDocument44 pagesDr. Husnil Kadri, M.KesElsa Giatri SiradjNo ratings yet
- ABO Blood GroupsDocument18 pagesABO Blood GroupsRamadan PhysiologyNo ratings yet
- Abo Group.Document33 pagesAbo Group.R.KABILANNo ratings yet
- Blood Group Incompatibility PDFDocument7 pagesBlood Group Incompatibility PDFSekar MarzukiNo ratings yet
- Blood Grouping LAB ZZSDocument22 pagesBlood Grouping LAB ZZSRahul Banik888No ratings yet
- المحاضرة 4Document5 pagesالمحاضرة 4Shi no MeNo ratings yet
- Hemolytic Anemia IIDocument18 pagesHemolytic Anemia IIArif MaulanaNo ratings yet
- Blood Type - Wikipedia 08-26-2021Document14 pagesBlood Type - Wikipedia 08-26-2021michael_sr_44No ratings yet
- Blood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryDocument44 pagesBlood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryChaudhary Vishant MalikNo ratings yet
- Blood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryDocument44 pagesBlood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryChaudhary Vishant MalikNo ratings yet
- Blood Group Substances: Their Chemistry and ImmunochemistryFrom EverandBlood Group Substances: Their Chemistry and ImmunochemistryRating: 5 out of 5 stars5/5 (1)
- How To Reduce The Risk of Injury?Document2 pagesHow To Reduce The Risk of Injury?Abdullah AlthobaitiNo ratings yet
- Vagina - Google SearchDocument1 pageVagina - Google SearchAbdullah AlthobaitiNo ratings yet
- Right & Left Gastroepiploic Vessels - Google SearchDocument1 pageRight & Left Gastroepiploic Vessels - Google SearchAbdullah AlthobaitiNo ratings yet
- 2-LFT Case Report Key AnswerDocument5 pages2-LFT Case Report Key AnswerAbdullah AlthobaitiNo ratings yet
- Slide Presentation For Literature ReviewDocument8 pagesSlide Presentation For Literature Reviewfvg7vpte100% (1)
- Donau CarbonDocument2 pagesDonau CarbonLim Chee SiangNo ratings yet
- Poutrelles-Pieux Américaines À Larges Ailes: Dimensions: ASTM A6 - 05 Tolérances: ASTM A6 - 05Document2 pagesPoutrelles-Pieux Américaines À Larges Ailes: Dimensions: ASTM A6 - 05 Tolérances: ASTM A6 - 05Nazar Abdul KareemNo ratings yet
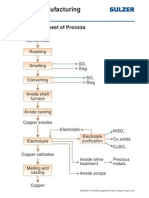
- Copper Manufacturing Process: General Flowsheet of ProcessDocument28 pagesCopper Manufacturing Process: General Flowsheet of ProcessflaviosazevedoNo ratings yet
- Branches of Forensic ScienceDocument19 pagesBranches of Forensic ScienceSriram ShirkeNo ratings yet
- Do You Have A Job Interview Coming UpDocument9 pagesDo You Have A Job Interview Coming UpLanie BermasNo ratings yet
- Quantity Estimate Store Room FinalDocument15 pagesQuantity Estimate Store Room FinalUjjwal ShresthaNo ratings yet
- 2020 ECO Topic 1 International Economic Integration Notes HannahDocument23 pages2020 ECO Topic 1 International Economic Integration Notes HannahJimmyNo ratings yet
- Ieee C37.20.3-2013Document70 pagesIeee C37.20.3-2013damaso taracena100% (2)
- Lesson 1.4 Literary Genres: Genres of Drama: Arellano UniversityDocument21 pagesLesson 1.4 Literary Genres: Genres of Drama: Arellano UniversityKing TadlasNo ratings yet
- U3A5 Practitioner's Handbook Organizing ChartDocument3 pagesU3A5 Practitioner's Handbook Organizing Chartkael9010 kael9010No ratings yet
- Learn-Html. - Various Jobs AvailableDocument19 pagesLearn-Html. - Various Jobs AvailableMichael GloverNo ratings yet
- The Arcgis BookDocument156 pagesThe Arcgis BookCristi Popa100% (2)
- An Overview of The Research of Psychological Entitlement. Definitions and Conceptual CharacteristicsDocument13 pagesAn Overview of The Research of Psychological Entitlement. Definitions and Conceptual CharacteristicsFarah AniaNo ratings yet
- 1 Quarter TLE 7 Week 7 Lesson: Hazard and Risk in The WorkplaceDocument15 pages1 Quarter TLE 7 Week 7 Lesson: Hazard and Risk in The WorkplaceNazzer NacuspagNo ratings yet
- SW 500Document28 pagesSW 500Sujit KumarNo ratings yet
- Joining Form IndigoDocument2 pagesJoining Form IndigodkasrvyNo ratings yet
- Spelling List Week 1-36Document38 pagesSpelling List Week 1-36Joel FernandezNo ratings yet
- Year 5 Maths Day 2 Two Way TablesDocument5 pagesYear 5 Maths Day 2 Two Way TablesvkumarNo ratings yet
- Critical Response Paper No.2Document4 pagesCritical Response Paper No.2Glenn SentesNo ratings yet
- High School JMarian 2012Document21 pagesHigh School JMarian 2012Jose Maria CollegeNo ratings yet
- A Progressive Christology and The MotifDocument43 pagesA Progressive Christology and The Motifmemra.travelNo ratings yet
- Chapter 5 Review AnswersDocument4 pagesChapter 5 Review AnswersMOHA DOOYOWNo ratings yet
- Top 10 PCB Assembly Companies in Thailand (Updated 2023)Document13 pagesTop 10 PCB Assembly Companies in Thailand (Updated 2023)jackNo ratings yet
- DHCP - DORA Process Call Flow WifiDocument18 pagesDHCP - DORA Process Call Flow WifiArjunAslekarNo ratings yet
- Standard Costing and Variance AnalysisDocument2 pagesStandard Costing and Variance AnalysisMISRET 2018 IEI JSCNo ratings yet
- Android - Architecture: Linux KernelDocument3 pagesAndroid - Architecture: Linux KernelMahnoor AslamNo ratings yet
- The Case Study of OliviaDocument2 pagesThe Case Study of Oliviabilly bongNo ratings yet
- FOR Approval Specification: Title 32.0" Wuxga TFT LCDDocument36 pagesFOR Approval Specification: Title 32.0" Wuxga TFT LCDСергій НестеровичNo ratings yet



























































































Download as pptx, pdf, or txt
You might also like
- RH and Abo IncompatibilityDocument10 pagesRH and Abo IncompatibilityamitNo ratings yet
- Guide To Fire Protection in MalaysiaDocument3 pagesGuide To Fire Protection in MalaysiaFadilah Ansari0% (2)
- Blood GroupsDocument38 pagesBlood GroupsVirendra JoshiNo ratings yet
- Lab 5Document22 pagesLab 5Aveen MustafaNo ratings yet
- RH IsoimmunizationDocument15 pagesRH Isoimmunizationgeorgeloto12No ratings yet
- Blood GroupDocument52 pagesBlood GroupShameena KnNo ratings yet
- Blood Types (Blood Groups) : Antigen (Agglutinogens)Document4 pagesBlood Types (Blood Groups) : Antigen (Agglutinogens)Khant Si ThuNo ratings yet
- Lecture10 - Blood Groups and TransfusionDocument28 pagesLecture10 - Blood Groups and Transfusionmohapatrarashmi050No ratings yet
- 12 - Blood GroupsDocument23 pages12 - Blood Groupsmohapatrarashmi050No ratings yet
- Blood BasicsDocument30 pagesBlood Basicskholoud220No ratings yet
- Blood Groups & CoagulationDocument12 pagesBlood Groups & CoagulationRAVI KANT PATELNo ratings yet
- ABO Grouping & RH FactorDocument3 pagesABO Grouping & RH FactorMadhurima PurkaitNo ratings yet
- BLOOD GROUPS MBBS.... MSK 3.9.18 LectureDocument37 pagesBLOOD GROUPS MBBS.... MSK 3.9.18 LectureJiyaa PatelNo ratings yet
- Bloodgroups 150424221954 Conversion Gate01Document38 pagesBloodgroups 150424221954 Conversion Gate01Endla SriniNo ratings yet
- Golongan Darah: Dr. Dr. Endang Sriwahyuni, MSDocument18 pagesGolongan Darah: Dr. Dr. Endang Sriwahyuni, MSDarma PutraNo ratings yet
- His 10Document2 pagesHis 10Kristin DouglasNo ratings yet
- 12 - Blood Groups and Blood Transfusion 2018Document27 pages12 - Blood Groups and Blood Transfusion 2018gimspath cme2022No ratings yet
- Blood GroubDocument21 pagesBlood Groubabdullahhassane299No ratings yet
- Blood GroupsDocument23 pagesBlood GroupsammarNo ratings yet
- Rhesus DiseaseDocument67 pagesRhesus DiseaseSalah EswaysiNo ratings yet
- Abo Blood RH GroupingDocument27 pagesAbo Blood RH GroupingJames Carbonell Dela PeñaNo ratings yet
- Abo Blood RH GroupingDocument22 pagesAbo Blood RH GroupingĐỗ Ngọc ÁnhNo ratings yet
- Hemolytic Diseases of The Fetus and NewbornDocument30 pagesHemolytic Diseases of The Fetus and Newbornkristine_camerinoNo ratings yet
- Blood Types & TransfusionDocument20 pagesBlood Types & TransfusionDr Imran AftabNo ratings yet
- BLOOD GROUPS TYPING - PowerpointDocument38 pagesBLOOD GROUPS TYPING - PowerpointJoy SNo ratings yet
- Blood TransfusionDocument28 pagesBlood Transfusionفيصل فهدNo ratings yet
- Blood TypingDocument11 pagesBlood Typingprakash gusainNo ratings yet
- The Blood Group Systems: Inheritance and GeneticsDocument34 pagesThe Blood Group Systems: Inheritance and GeneticsP Vinod Kumar100% (1)
- Genotype and Blood Group CompatibilityDocument5 pagesGenotype and Blood Group CompatibilityajayranjithNo ratings yet
- Blood Group NewDocument44 pagesBlood Group NewArpita SankhwarNo ratings yet
- RH Factor GeneticsDocument9 pagesRH Factor Geneticsbushra sajjadNo ratings yet
- Blood Group ND Transfusion - 231202 - 151259Document54 pagesBlood Group ND Transfusion - 231202 - 151259Archisman Mukherjee FAPSIANNo ratings yet
- Blood Group & RHDocument27 pagesBlood Group & RHfamtaluNo ratings yet
- TP Immunology English 2018 For StudentDocument83 pagesTP Immunology English 2018 For StudentKhaled Abo Al OyounNo ratings yet
- Blood Groups: Dr. Kenan GumustekinDocument43 pagesBlood Groups: Dr. Kenan Gumustekinsyed nomanshahNo ratings yet
- BBDocument6 pagesBBFrey Mary Dela PeñaNo ratings yet
- 1.blood GroupDocument38 pages1.blood GroupteraraNo ratings yet
- Bloog GroupDocument3 pagesBloog GroupChennai IbrahimNo ratings yet
- Blood Typing, Rhesus Factor, and BloodDocument40 pagesBlood Typing, Rhesus Factor, and BloodHalima IliyasuNo ratings yet
- Blood Grouping 1690574753Document30 pagesBlood Grouping 1690574753willowmaecayabyabNo ratings yet
- The Cardiovascular System 3Document17 pagesThe Cardiovascular System 3aboody62621No ratings yet
- ABO Blood Typing: Elrey L/ Navarro MD, DPCOMDocument42 pagesABO Blood Typing: Elrey L/ Navarro MD, DPCOMAnonymous 2TzM1Z100% (1)
- ABO and RH Blood Group SystemDocument31 pagesABO and RH Blood Group SystemKaab Ishaq100% (1)
- Blood GroupsDocument53 pagesBlood GroupsSneh KevadiyaNo ratings yet
- Blood Case 6Document12 pagesBlood Case 6إنعام الحفيانNo ratings yet
- Blood Groups and Blood Transfusion BioDocument23 pagesBlood Groups and Blood Transfusion BiowhyyoucareNo ratings yet
- Blood Group and Transfusion ReactionDocument15 pagesBlood Group and Transfusion ReactionAhmad KhanNo ratings yet
- RH SystemDocument22 pagesRH Systemhistorymonday10No ratings yet
- Abo and MN Blood Group SystemDocument54 pagesAbo and MN Blood Group SystemAkram chaudaryNo ratings yet
- Dr. Husnil Kadri, M.KesDocument44 pagesDr. Husnil Kadri, M.KesElsa Giatri SiradjNo ratings yet
- ABO Blood GroupsDocument18 pagesABO Blood GroupsRamadan PhysiologyNo ratings yet
- Abo Group.Document33 pagesAbo Group.R.KABILANNo ratings yet
- Blood Group Incompatibility PDFDocument7 pagesBlood Group Incompatibility PDFSekar MarzukiNo ratings yet
- Blood Grouping LAB ZZSDocument22 pagesBlood Grouping LAB ZZSRahul Banik888No ratings yet
- المحاضرة 4Document5 pagesالمحاضرة 4Shi no MeNo ratings yet
- Hemolytic Anemia IIDocument18 pagesHemolytic Anemia IIArif MaulanaNo ratings yet
- Blood Type - Wikipedia 08-26-2021Document14 pagesBlood Type - Wikipedia 08-26-2021michael_sr_44No ratings yet
- Blood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryDocument44 pagesBlood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryChaudhary Vishant MalikNo ratings yet
- Blood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryDocument44 pagesBlood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryChaudhary Vishant MalikNo ratings yet
- Blood Group Substances: Their Chemistry and ImmunochemistryFrom EverandBlood Group Substances: Their Chemistry and ImmunochemistryRating: 5 out of 5 stars5/5 (1)
- How To Reduce The Risk of Injury?Document2 pagesHow To Reduce The Risk of Injury?Abdullah AlthobaitiNo ratings yet
- Vagina - Google SearchDocument1 pageVagina - Google SearchAbdullah AlthobaitiNo ratings yet
- Right & Left Gastroepiploic Vessels - Google SearchDocument1 pageRight & Left Gastroepiploic Vessels - Google SearchAbdullah AlthobaitiNo ratings yet
- 2-LFT Case Report Key AnswerDocument5 pages2-LFT Case Report Key AnswerAbdullah AlthobaitiNo ratings yet
- Slide Presentation For Literature ReviewDocument8 pagesSlide Presentation For Literature Reviewfvg7vpte100% (1)
- Donau CarbonDocument2 pagesDonau CarbonLim Chee SiangNo ratings yet
- Poutrelles-Pieux Américaines À Larges Ailes: Dimensions: ASTM A6 - 05 Tolérances: ASTM A6 - 05Document2 pagesPoutrelles-Pieux Américaines À Larges Ailes: Dimensions: ASTM A6 - 05 Tolérances: ASTM A6 - 05Nazar Abdul KareemNo ratings yet
- Copper Manufacturing Process: General Flowsheet of ProcessDocument28 pagesCopper Manufacturing Process: General Flowsheet of ProcessflaviosazevedoNo ratings yet
- Branches of Forensic ScienceDocument19 pagesBranches of Forensic ScienceSriram ShirkeNo ratings yet
- Do You Have A Job Interview Coming UpDocument9 pagesDo You Have A Job Interview Coming UpLanie BermasNo ratings yet
- Quantity Estimate Store Room FinalDocument15 pagesQuantity Estimate Store Room FinalUjjwal ShresthaNo ratings yet
- 2020 ECO Topic 1 International Economic Integration Notes HannahDocument23 pages2020 ECO Topic 1 International Economic Integration Notes HannahJimmyNo ratings yet
- Ieee C37.20.3-2013Document70 pagesIeee C37.20.3-2013damaso taracena100% (2)
- Lesson 1.4 Literary Genres: Genres of Drama: Arellano UniversityDocument21 pagesLesson 1.4 Literary Genres: Genres of Drama: Arellano UniversityKing TadlasNo ratings yet
- U3A5 Practitioner's Handbook Organizing ChartDocument3 pagesU3A5 Practitioner's Handbook Organizing Chartkael9010 kael9010No ratings yet
- Learn-Html. - Various Jobs AvailableDocument19 pagesLearn-Html. - Various Jobs AvailableMichael GloverNo ratings yet
- The Arcgis BookDocument156 pagesThe Arcgis BookCristi Popa100% (2)
- An Overview of The Research of Psychological Entitlement. Definitions and Conceptual CharacteristicsDocument13 pagesAn Overview of The Research of Psychological Entitlement. Definitions and Conceptual CharacteristicsFarah AniaNo ratings yet
- 1 Quarter TLE 7 Week 7 Lesson: Hazard and Risk in The WorkplaceDocument15 pages1 Quarter TLE 7 Week 7 Lesson: Hazard and Risk in The WorkplaceNazzer NacuspagNo ratings yet
- SW 500Document28 pagesSW 500Sujit KumarNo ratings yet
- Joining Form IndigoDocument2 pagesJoining Form IndigodkasrvyNo ratings yet
- Spelling List Week 1-36Document38 pagesSpelling List Week 1-36Joel FernandezNo ratings yet
- Year 5 Maths Day 2 Two Way TablesDocument5 pagesYear 5 Maths Day 2 Two Way TablesvkumarNo ratings yet
- Critical Response Paper No.2Document4 pagesCritical Response Paper No.2Glenn SentesNo ratings yet
- High School JMarian 2012Document21 pagesHigh School JMarian 2012Jose Maria CollegeNo ratings yet
- A Progressive Christology and The MotifDocument43 pagesA Progressive Christology and The Motifmemra.travelNo ratings yet
- Chapter 5 Review AnswersDocument4 pagesChapter 5 Review AnswersMOHA DOOYOWNo ratings yet
- Top 10 PCB Assembly Companies in Thailand (Updated 2023)Document13 pagesTop 10 PCB Assembly Companies in Thailand (Updated 2023)jackNo ratings yet
- DHCP - DORA Process Call Flow WifiDocument18 pagesDHCP - DORA Process Call Flow WifiArjunAslekarNo ratings yet
- Standard Costing and Variance AnalysisDocument2 pagesStandard Costing and Variance AnalysisMISRET 2018 IEI JSCNo ratings yet
- Android - Architecture: Linux KernelDocument3 pagesAndroid - Architecture: Linux KernelMahnoor AslamNo ratings yet
- The Case Study of OliviaDocument2 pagesThe Case Study of Oliviabilly bongNo ratings yet
- FOR Approval Specification: Title 32.0" Wuxga TFT LCDDocument36 pagesFOR Approval Specification: Title 32.0" Wuxga TFT LCDСергій НестеровичNo ratings yet