Download as pptx, pdf, or txt
You might also like
- Jansenkoh MRCP PacesDocument209 pagesJansenkoh MRCP PacesBob Yong83% (6)
- Rheumatic Heart DiseaseDocument39 pagesRheumatic Heart DiseaseRezwanul Hoque Bulbul100% (1)
- Valvular Heart Disease1Document80 pagesValvular Heart Disease1Abnet WondimuNo ratings yet
- Mitral StenosisDocument95 pagesMitral StenosisAbnet WondimuNo ratings yet
- Kuliah MITRAL STENOSISDocument19 pagesKuliah MITRAL STENOSISekaseptiani312No ratings yet
- Kuliah MITRAL STENOSISDocument19 pagesKuliah MITRAL STENOSISAdi TrisnoNo ratings yet
- Tricuspid, Pulmonic and Mixed Valve DisordersDocument112 pagesTricuspid, Pulmonic and Mixed Valve DisordersAbnet WondimuNo ratings yet
- Question: Ostium Secondum Type of ASD: PrevalenceDocument9 pagesQuestion: Ostium Secondum Type of ASD: Prevalencesharon victoria mendezNo ratings yet
- Penyakit Katup Jantung-Kuliah DR ErlinaDocument70 pagesPenyakit Katup Jantung-Kuliah DR ErlinaAdhiatma DotNo ratings yet
- Aortic Stenosis - LecturioDocument13 pagesAortic Stenosis - Lecturiokujtimepira2No ratings yet
- Rheumatic Heart Disease2Document61 pagesRheumatic Heart Disease2Puji Yunisyah RahayuNo ratings yet
- Mitral Stenosis, NicvdDocument33 pagesMitral Stenosis, NicvdNavojit ChowdhuryNo ratings yet
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNo ratings yet
- Auscultation of The HeartDocument84 pagesAuscultation of The HeartASTOASTONo ratings yet
- Ventricular Septal DefectDocument43 pagesVentricular Septal DefectmalekNo ratings yet
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Pathophys VHD-Final (Budi S. Pikir)Document155 pagesPathophys VHD-Final (Budi S. Pikir)Muhammad DaviqNo ratings yet
- 7 PENYAKIT JANTUNG BAWAAN DR - YusraDocument57 pages7 PENYAKIT JANTUNG BAWAAN DR - YusraSurya ArhNo ratings yet
- Heart Valve DiseaseDocument67 pagesHeart Valve DiseaseSaba SivaNo ratings yet
- Achd Ug OriginalDocument43 pagesAchd Ug OriginalchristyNo ratings yet
- Mitral Valve StenosisDocument5 pagesMitral Valve StenosisrroxanarrusuNo ratings yet
- Aortic StenosisDocument4 pagesAortic StenosisSukuria UsmanNo ratings yet
- PJB Pada Dewasa AASDocument54 pagesPJB Pada Dewasa AAS1e23e2ewNo ratings yet
- Rheumatic Heart Disease: Emmanuel Edafe Consultant Interventional Cardiologist, NduDocument36 pagesRheumatic Heart Disease: Emmanuel Edafe Consultant Interventional Cardiologist, NduPrincewill Seiyefa100% (1)
- Valvular Heart Disease: Bekele T. (MD)Document47 pagesValvular Heart Disease: Bekele T. (MD)alehegn beleteNo ratings yet
- Aortic RegurgitationDocument134 pagesAortic RegurgitationAbnet WondimuNo ratings yet
- Tiki Taka Notes Final PDFDocument104 pagesTiki Taka Notes Final PDFAditiSahak62No ratings yet
- Aortic StenosisDocument15 pagesAortic StenosisSanjeet SahNo ratings yet
- Rheumatic Heart DiseaseDocument47 pagesRheumatic Heart Diseaserichardkikondo5No ratings yet
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Document51 pagesDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Mitral Stenosis: Acute Rheumatic Fever (ARF) PancarditisDocument4 pagesMitral Stenosis: Acute Rheumatic Fever (ARF) PancarditisFitria HasyimNo ratings yet
- CONGENITAL HEART DISEASE Non DeptDocument47 pagesCONGENITAL HEART DISEASE Non DeptAkshaya MistryNo ratings yet
- Rheumatic Heart DiseaseDocument47 pagesRheumatic Heart DiseaseGideon K. MutaiNo ratings yet
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanNo ratings yet
- Congenital Heart Disease Acyanotic: Department of Cardiovascular Surgery St. George University General HospitalDocument81 pagesCongenital Heart Disease Acyanotic: Department of Cardiovascular Surgery St. George University General HospitalKonstantin DimitrovNo ratings yet
- Penyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaiDocument59 pagesPenyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaianisamayaNo ratings yet
- Congenital Heart DeseasesDocument54 pagesCongenital Heart DeseasesAntony100% (1)
- TUGAS Ventricular Septal DefectDocument8 pagesTUGAS Ventricular Septal DefectMohammad NafisNo ratings yet
- IVMS Heart and Lung Auscultation Sounds NotesDocument7 pagesIVMS Heart and Lung Auscultation Sounds NotesMarc Imhotep Cray, M.D.No ratings yet
- Valvular Heart Disease IM 8-12 NewDocument80 pagesValvular Heart Disease IM 8-12 NewRachilla Arandita SaraswatiNo ratings yet
- Case History - VSDDocument4 pagesCase History - VSDqayyum consultantfpscNo ratings yet
- Mid-Systolic Ejection: Time Condition DescriptionDocument3 pagesMid-Systolic Ejection: Time Condition DescriptionZahrosofi AhmadahNo ratings yet
- MitralStenosis in ChinaDocument12 pagesMitralStenosis in Chinaannis fathiaNo ratings yet
- USMLE General CardiologyDocument72 pagesUSMLE General CardiologyWidyo MahargoNo ratings yet
- Truncus Arteriosus TransletDocument11 pagesTruncus Arteriosus TransletHijaz Al-YamanNo ratings yet
- Aortic RegurgitationDocument16 pagesAortic Regurgitationrobby zayendraNo ratings yet
- Patho 1Document153 pagesPatho 1ademabdellaaleNo ratings yet
- Complete Transposition of Great ArteriesDocument85 pagesComplete Transposition of Great ArteriesRahul AgrawalNo ratings yet
- Pulmonary Valve StenosisDocument6 pagesPulmonary Valve StenosisKobby AmoahNo ratings yet
- Tetrology of FallotDocument55 pagesTetrology of FallotShravani ShagapuramNo ratings yet
- Valvular Heart DiseaseDocument32 pagesValvular Heart DiseasefallenczarNo ratings yet
- Mitral Stenosis: JONES Criteria - 2015 Modification Major CriteriaDocument13 pagesMitral Stenosis: JONES Criteria - 2015 Modification Major CriteriaBiswarup PurkayasthaNo ratings yet
- Research Paper On Heart MurmurDocument4 pagesResearch Paper On Heart Murmurnodahydomut2100% (1)
- 1 Mitral Stenosis: InstructionDocument8 pages1 Mitral Stenosis: Instructionrashid.scribdNo ratings yet
- 3 CRHD CMP and CHDDocument73 pages3 CRHD CMP and CHDDammaqsaa W BiyyanaaNo ratings yet
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDocument69 pagesValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaNo ratings yet
- Calixtro Narrative Aortic StenosisDocument2 pagesCalixtro Narrative Aortic StenosisKim SunooNo ratings yet
- Aortic StenosisDocument37 pagesAortic Stenosissarguss14No ratings yet
- Valvular Heart DiseaseDocument5 pagesValvular Heart DiseaseElyas MehdarNo ratings yet
- 5 ArrhythmiaDocument44 pages5 ArrhythmiaDanny DesuNo ratings yet
- 1 Rheumatic Fever and RHDDocument53 pages1 Rheumatic Fever and RHDDanny DesuNo ratings yet
- 4 CardiomyopathyDocument54 pages4 CardiomyopathyDanny DesuNo ratings yet
- 3 Ischemic Heart Disease - PPTX Year 3 2Document40 pages3 Ischemic Heart Disease - PPTX Year 3 2Danny DesuNo ratings yet
- Respiratory Physiology BudDocument69 pagesRespiratory Physiology BudGabriel Liberon P. JazonNo ratings yet
- So April 2023Document36 pagesSo April 2023elisantagrace brawijayalaboratoryNo ratings yet
- Topic 1 Endocrine SystemDocument140 pagesTopic 1 Endocrine SystemmasdfgNo ratings yet
- What Is Human Body Tissue PDFDocument3 pagesWhat Is Human Body Tissue PDFEng Abdulahi Haji100% (1)
- The Effects of STRESS On Your Body: Your Company Name/Logo HereDocument2 pagesThe Effects of STRESS On Your Body: Your Company Name/Logo HereIveta NikolovaNo ratings yet
- NCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMADocument5 pagesNCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMAMa. Elaine Carla Tating50% (2)
- Core CH 9 Nutrition and Gas Exchange in PlantsDocument6 pagesCore CH 9 Nutrition and Gas Exchange in PlantsommpNo ratings yet
- HematomaDocument2 pagesHematomaleonel ocanaNo ratings yet
- Training For Strength and Hypertrophy - An Evidence-Based ApproachDocument14 pagesTraining For Strength and Hypertrophy - An Evidence-Based ApproachPrecision Wellness Precision WellnessNo ratings yet
- Icd 9 TindakanDocument6 pagesIcd 9 TindakanmirnaNo ratings yet
- 0 Tips For Deep, Rejuvenating, Age-Reversing SleepDocument7 pages0 Tips For Deep, Rejuvenating, Age-Reversing SleepFlori MarcociNo ratings yet
- Photosynthesis & Respiration Worksheet - KeyDocument2 pagesPhotosynthesis & Respiration Worksheet - KeyCIARA HUGULEY100% (2)
- HypothalamusDocument5 pagesHypothalamusBoneGrissleNo ratings yet
- Unit 6 Flash Cards Hematology CoagulationDocument13 pagesUnit 6 Flash Cards Hematology CoagulationLois LipanovichNo ratings yet
- (ANAPHY) Introduction To Anatomy and PhysiologyDocument5 pages(ANAPHY) Introduction To Anatomy and PhysiologyPearl FllominNo ratings yet
- Vasquez NCP OB ROTATIONDocument10 pagesVasquez NCP OB ROTATIONKimberly Gonzaga VasquezNo ratings yet
- The Cardiovascular System: Heart, Blood Vessels, BloodDocument9 pagesThe Cardiovascular System: Heart, Blood Vessels, BloodKrishnendu WorkNo ratings yet
- Diagnostic SpirometerDocument3 pagesDiagnostic SpirometerseventhsensegroupNo ratings yet
- Diazoxide 50mg DatasheetDocument6 pagesDiazoxide 50mg DatasheetarifpharmjuNo ratings yet
- Blood Pressure Force That Drives Blood Through Arteries and Capillaries Highest in Aorta and Large Arteries Normal Adult BP at Rest 120/80 MM HGDocument4 pagesBlood Pressure Force That Drives Blood Through Arteries and Capillaries Highest in Aorta and Large Arteries Normal Adult BP at Rest 120/80 MM HGNur Hazwah WahidNo ratings yet
- CHAPTER 6 Muscular SystemDocument118 pagesCHAPTER 6 Muscular SystemPaul Jean MerinoNo ratings yet
- Xylem: A Vascular Tissue in Land PlantsDocument4 pagesXylem: A Vascular Tissue in Land PlantsJoshua-Jonai JulyeNo ratings yet
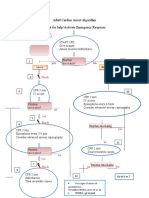
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocument1 pageAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMNo ratings yet
- Respiration LabDocument4 pagesRespiration LabLogan Parkison100% (1)
- Novada ACLS AHA 2015Document25 pagesNovada ACLS AHA 2015novada indraNo ratings yet
- Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument21 pagesDepartemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraFira TasyaNo ratings yet
- Performance Gains Following Resistance Breathing Exercises: Single Subject Case StudyDocument4 pagesPerformance Gains Following Resistance Breathing Exercises: Single Subject Case StudysdjuknicNo ratings yet
- Assignment No.1 OB High Risk Grp.1Document15 pagesAssignment No.1 OB High Risk Grp.1YongNo ratings yet
- اختبار مزاولة بكالوريوس تمريض 15 3 2023Document6 pagesاختبار مزاولة بكالوريوس تمريض 15 3 2023Hero StoreNo ratings yet
- General Anesthesia: Intravenous Induction Agents - UpToDateDocument47 pagesGeneral Anesthesia: Intravenous Induction Agents - UpToDateAhmet PinarbasiNo ratings yet