Download as pptx, pdf, or txt
You might also like
- PhilPEN Plus Risk Assessment FormDocument2 pagesPhilPEN Plus Risk Assessment FormRhu Salay75% (4)
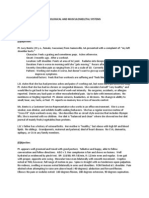
- Soap Note - Musculoskeletal and Nervous SystemsDocument2 pagesSoap Note - Musculoskeletal and Nervous SystemsSummer Keller88% (8)
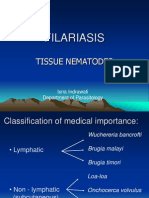
- FILARIASIS PPT FINALDocument39 pagesFILARIASIS PPT FINALBinita Shakya100% (2)
- PALS Study Guide: 2020 GuidelinesDocument3 pagesPALS Study Guide: 2020 GuidelinesVictoria Kidd100% (4)
- FILARIASISDocument57 pagesFILARIASISadekayo100% (6)
- Proceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964From EverandProceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964Augusto CorradettiNo ratings yet
- Surgery Nbme ReviewDocument3 pagesSurgery Nbme Reviewhannahylee71188% (8)
- Oxygenation Practice QuizDocument3 pagesOxygenation Practice QuizJoy Dunwan0% (1)
- 4.3. Blood and Tissue NematodesDocument89 pages4.3. Blood and Tissue NematodesRediat GossayeNo ratings yet
- Blood and Tissue Nematods 2015Document109 pagesBlood and Tissue Nematods 2015sinte beyuNo ratings yet
- Blood and Tissue NematodesDocument29 pagesBlood and Tissue Nematodesdeneke100% (2)
- Unit - 4-3 - Blood and Tissue NematodesDocument130 pagesUnit - 4-3 - Blood and Tissue NematodesDembalu NuguseNo ratings yet
- Blood & Tissue NematodesDocument96 pagesBlood & Tissue NematodesruthNo ratings yet
- BN Filarial WormDocument137 pagesBN Filarial WormCherenet TomaNo ratings yet
- 2019limphatic Filaria PDocument39 pages2019limphatic Filaria PFebbby Mutia SafiraNo ratings yet
- Revision: Types of Life Cycle in Trematoda and CestodaDocument54 pagesRevision: Types of Life Cycle in Trematoda and CestodaMicroscopeGeekNo ratings yet
- Wuchereria Bancrofti: Aby Elijah L. BernardinoDocument22 pagesWuchereria Bancrofti: Aby Elijah L. BernardinoAby Brr100% (1)
- Lymphatic Filariasis ClassDocument68 pagesLymphatic Filariasis ClassthehexhealthNo ratings yet
- Bancrofthian Lymphatic FilariasisDocument20 pagesBancrofthian Lymphatic FilariasisrahmiNo ratings yet
- Wuchereria BancroftiDocument46 pagesWuchereria BancroftiSolomon Fallah Foa SandyNo ratings yet
- Blood Nematodes, Cestode and TrematodeDocument63 pagesBlood Nematodes, Cestode and TrematodeChangkuoth Dak PuochNo ratings yet
- BIOLOGY PROJECTS CLASS 12 CBSE INVESTIGTORY Elephantiasis Causes Cures Prevention, Treatment, Causes and Case Studies..Document28 pagesBIOLOGY PROJECTS CLASS 12 CBSE INVESTIGTORY Elephantiasis Causes Cures Prevention, Treatment, Causes and Case Studies..Gaurav Kumar63% (19)
- Blood Tissue NematodesDocument27 pagesBlood Tissue NematodesAfif Mamen100% (1)
- Filariasis: Dr. Suhaemi, SPPD, FinasimDocument30 pagesFilariasis: Dr. Suhaemi, SPPD, FinasimErreli K. KhusumawerdanieNo ratings yet
- Blood and Tissue NematodesDocument60 pagesBlood and Tissue NematodesJefferson SorianoNo ratings yet
- Lymphatic FillairiasisDocument7 pagesLymphatic FillairiasisRitche DamasinNo ratings yet
- Filariasis 2015Document56 pagesFilariasis 2015ChandraNo ratings yet
- Blood Borne Helminths - Wucherelia BancroftiDocument15 pagesBlood Borne Helminths - Wucherelia BancroftiCLEMENTNo ratings yet
- Lecture 7 Nematodes Part 2 New 2023Document19 pagesLecture 7 Nematodes Part 2 New 2023ayaessam392002No ratings yet
- W - BancroftiDocument19 pagesW - BancroftiALLISON PAMITTANNo ratings yet
- FilariaDocument16 pagesFilariaJessa MayNo ratings yet
- Filaria-Limf 12Document30 pagesFilaria-Limf 12JuwitaNo ratings yet
- Filariasis in NepalDocument41 pagesFilariasis in NepalBinaya100% (1)
- Report PARA Lymphatic Filarial Nematodes Group 2 Adalid Asug AustriaDocument28 pagesReport PARA Lymphatic Filarial Nematodes Group 2 Adalid Asug AustriaDaniel AustriaNo ratings yet
- Parasitology - Blood & Tissue - W Bancrofti B Malayi - PresentationDocument43 pagesParasitology - Blood & Tissue - W Bancrofti B Malayi - PresentationNicole ManogNo ratings yet
- 28 Sept 2016 Kuliah Filariasis BaruDocument31 pages28 Sept 2016 Kuliah Filariasis BaruRafif AmirNo ratings yet
- Man Bahadur Rana BPH, Acas, NepalDocument34 pagesMan Bahadur Rana BPH, Acas, NepalDipankar NathNo ratings yet
- Filariasis: Dr.T.V.Rao MDDocument62 pagesFilariasis: Dr.T.V.Rao MDDipankar NathNo ratings yet
- Filarial NematodeDocument18 pagesFilarial NematodeHawre NajmaddinNo ratings yet
- Epidemiology of Lymphatic FilariasisDocument26 pagesEpidemiology of Lymphatic FilariasisvaishnaviNo ratings yet
- Yousif AlaaDocument7 pagesYousif AlaaYousif AlaaNo ratings yet
- Frequently Asked Quaestions (FAQs)Document22 pagesFrequently Asked Quaestions (FAQs)Drop Ur.questionNo ratings yet
- L-5 Arthropod Borne InfectionDocument7 pagesL-5 Arthropod Borne InfectionAnisha KuriakoseNo ratings yet
- Tissue NematodesDocument27 pagesTissue Nematodesadenijidamilola88No ratings yet
- The Filariae: Lymphatic System, Subcutaneous and Deep Connective TissueDocument17 pagesThe Filariae: Lymphatic System, Subcutaneous and Deep Connective TissueKaranja GitauNo ratings yet
- Filaria - A Comprehensive StudyDocument63 pagesFilaria - A Comprehensive StudyDayledaniel SorvetoNo ratings yet
- Wuchereria BancroftiDocument13 pagesWuchereria Bancroftiumeshchandralenka09No ratings yet
- FilariasisDocument13 pagesFilariasissarguss14100% (3)
- 7 BIO3243 ElephantiasisDocument11 pages7 BIO3243 ElephantiasisNGOGA NISINGIZWE NESTORNo ratings yet
- Man Bahadur Rana BPH, Acas, NepalDocument34 pagesMan Bahadur Rana BPH, Acas, NepalDipankar NathNo ratings yet
- 9 BIO3243 Lecturer4 RiverblindnessDocument18 pages9 BIO3243 Lecturer4 RiverblindnessNGOGA NISINGIZWE NESTORNo ratings yet
- 1) FilariasisDocument25 pages1) FilariasisNorbatNo ratings yet
- Blood and Tissue NematodesDocument37 pagesBlood and Tissue NematodesjelenaNo ratings yet
- Filariasis LYMPHATIC FILARIASISDocument8 pagesFilariasis LYMPHATIC FILARIASISapih_2629No ratings yet
- 1 MalariaDocument94 pages1 MalariaAbdurahman TainyNo ratings yet
- General Parasitology L6Document13 pagesGeneral Parasitology L6kayse abtidoonNo ratings yet
- Blood &lymphatic System 2015Document30 pagesBlood &lymphatic System 2015nur annisyaNo ratings yet
- Blood and Tissue Flagellates BSCDocument27 pagesBlood and Tissue Flagellates BSCSisay FentaNo ratings yet
- Guidelines Filariasis Elimination IndiaDocument108 pagesGuidelines Filariasis Elimination IndiaegalivanNo ratings yet
- Blood and Tissue NematodesDocument60 pagesBlood and Tissue NematodesDanielle Pecson100% (1)
- MalariaDocument57 pagesMalariaDawit g/kidanNo ratings yet
- Filarial and Extra Intestinal Nematodes 1Document102 pagesFilarial and Extra Intestinal Nematodes 1Brenda OctavioNo ratings yet
- Helemnth ReportDocument15 pagesHelemnth ReportHawre NajmaddinNo ratings yet
- Filariasis: Causes, Tests, and Treatment OptionsFrom EverandFilariasis: Causes, Tests, and Treatment OptionsRating: 5 out of 5 stars5/5 (2)
- Mental Status ExaminationDocument19 pagesMental Status ExaminationAgrave Mikhael JamesNo ratings yet
- Neonatal Acute Abdomen. 7th YrDocument54 pagesNeonatal Acute Abdomen. 7th YrFreeburn SimunchembuNo ratings yet
- Fdocuments - in Kangen Water SamirDocument24 pagesFdocuments - in Kangen Water SamirNitin MhatreNo ratings yet
- NCM 116 Endocrine DisordersDocument106 pagesNCM 116 Endocrine DisordersAnthony Seth AguilandoNo ratings yet
- Bloodborne Pathogens TrainingDocument28 pagesBloodborne Pathogens TrainingPeter GolanskiNo ratings yet
- MetoclopramideDocument3 pagesMetoclopramideMatt Reyes Del CastilloNo ratings yet
- Review of Related LiteratureDocument11 pagesReview of Related LiteratureLunel John RuazaNo ratings yet
- Prevalence and Pattern of Menstrual Disorders IJARDocument3 pagesPrevalence and Pattern of Menstrual Disorders IJARWilson ThomasNo ratings yet
- History and Neck HistoryDocument4 pagesHistory and Neck HistoryAzria John DemetriNo ratings yet
- Plab 2 Recall 4Document134 pagesPlab 2 Recall 4Sadiya IslamNo ratings yet
- Evaluation of Low Back Pain in Adults - UpToDateDocument25 pagesEvaluation of Low Back Pain in Adults - UpToDateJeissonPargaSalasNo ratings yet
- NCM 114 Rle Midterm ReviewerDocument4 pagesNCM 114 Rle Midterm ReviewerDanica NuevaexcijaNo ratings yet
- Tan Teaching-PlanDocument2 pagesTan Teaching-PlanPatrick Ray TanNo ratings yet
- Thiamine Tetrahydrofurfuryl Disulfi De: A Little Known Therapeutic AgentDocument6 pagesThiamine Tetrahydrofurfuryl Disulfi De: A Little Known Therapeutic AgentPrima DimalouwNo ratings yet
- Haematological StudiesDocument100 pagesHaematological StudiesDebabrata KarmakarNo ratings yet
- Carolyn O'Neal ComplaintDocument42 pagesCarolyn O'Neal ComplaintLaw&Crime100% (1)
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- Oral Biopsy: Oral Pathologist's Perspective: Review ArticleDocument7 pagesOral Biopsy: Oral Pathologist's Perspective: Review ArticleRafa LopezNo ratings yet
- LP 02 - HeadacheDocument29 pagesLP 02 - HeadacheIoana CozmaNo ratings yet
- Topic - 5 - Mers - Cov - (7) FINALDocument12 pagesTopic - 5 - Mers - Cov - (7) FINALApril FlorendoNo ratings yet
- PREPUMASTERKEY (Repaired)Document2,031 pagesPREPUMASTERKEY (Repaired)surviving nursing schoolNo ratings yet
- Anatomy Head Neck EMRCS MCQDocument23 pagesAnatomy Head Neck EMRCS MCQTowhid HasanNo ratings yet
- Reviewer 116 Rle Midterm ExamDocument25 pagesReviewer 116 Rle Midterm ExamMark Nathaniel ValerioNo ratings yet
- Functional Syndrome in NeurologyDocument11 pagesFunctional Syndrome in Neurologyidno1008No ratings yet
- Metronidazole Drug StudyDocument3 pagesMetronidazole Drug StudySiafei RabeNo ratings yet