Download as pptx, pdf, or txt
You might also like
- Hesi Psych Study GuideDocument16 pagesHesi Psych Study GuideR100% (17)
- Chapter 29: Hematologic System Introduction Linton: Medical-Surgical Nursing, 7th EditionDocument5 pagesChapter 29: Hematologic System Introduction Linton: Medical-Surgical Nursing, 7th EditionStacey100% (1)
- Sabiston Biliary System NotesDocument5 pagesSabiston Biliary System NotessvidrillionNo ratings yet
- Calculous Biliary DiseaseDocument71 pagesCalculous Biliary DiseaseMinnossNo ratings yet
- Non Viral HepatitisDocument40 pagesNon Viral Hepatitisostaz2000100% (1)
- Overview of Lower GastroIntestinal Bleeding 1.1Document42 pagesOverview of Lower GastroIntestinal Bleeding 1.1Raja Ain100% (1)
- Dr. Rabi Dhakal 1 Year MD Resident Department of PediatricDocument29 pagesDr. Rabi Dhakal 1 Year MD Resident Department of PediatricRabi Dhakal100% (1)
- CH 20 Manter Gatz S Essentials of Clinical Neuroanatomy and NeurophysiologyDocument27 pagesCH 20 Manter Gatz S Essentials of Clinical Neuroanatomy and Neurophysiologyasarg214100% (1)
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Jaundice: Seminar Under The Guidance Of-Dr. Shiva NarangDocument47 pagesJaundice: Seminar Under The Guidance Of-Dr. Shiva NarangMiguel MansillaNo ratings yet
- 17 - Gallbladder StonesDocument71 pages17 - Gallbladder StonesRashed Shatnawi100% (1)
- Disease of The Biliary TractDocument7 pagesDisease of The Biliary TractMae DoctoleroNo ratings yet
- Inflammatory Bowel DiseaseDocument51 pagesInflammatory Bowel DiseaseTeena Chandran100% (1)
- Acute AbdomenDocument19 pagesAcute AbdomenNazmi Z. MehmetiNo ratings yet
- 2-Acute Abdominal PainDocument24 pages2-Acute Abdominal Painabdalmajeed alshammaryNo ratings yet
- Cholecystitis: Bonoan, Camille Grace Chua, ManilynDocument29 pagesCholecystitis: Bonoan, Camille Grace Chua, ManilynCams BonoanNo ratings yet
- Surgical JaundiceDocument40 pagesSurgical JaundiceAbdulsalam DostNo ratings yet
- Per Rectal Bleeding CompiledDocument33 pagesPer Rectal Bleeding CompiledRajhmuniran Kandasamy100% (1)
- Abdominal History TakingDocument33 pagesAbdominal History TakingGazi Shahinur Akter ShampaNo ratings yet
- Large Bowel Obstruction by Nic MDocument42 pagesLarge Bowel Obstruction by Nic MRisky OpponentNo ratings yet
- Malignant Liver Tumors Undergrad 6th Year Students SharaanDocument56 pagesMalignant Liver Tumors Undergrad 6th Year Students SharaanMohamed AhmedNo ratings yet
- Acute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHDocument45 pagesAcute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHWaleed MaboodNo ratings yet
- 5 Mesenteric IschemiaDocument39 pages5 Mesenteric IschemiaFahd Abdullah Al-refaiNo ratings yet
- The Acute AbdomenDocument174 pagesThe Acute AbdomenHabibHusseinJasmanNo ratings yet
- Acute Cholecystitis SMT IV 2021Document43 pagesAcute Cholecystitis SMT IV 2021Dandi PremaNo ratings yet
- Portal HypertensionDocument4 pagesPortal HypertensiondrstalamNo ratings yet
- Jaundice: DR: Ramy A. SamyDocument42 pagesJaundice: DR: Ramy A. Samyoscar3spurgeonNo ratings yet
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995No ratings yet
- CHOLEDOCHOLITHIASISDocument8 pagesCHOLEDOCHOLITHIASISkuncupcupu1368No ratings yet
- Pancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011Document18 pagesPancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011mywifenoor1983No ratings yet
- Acute PancreatitisDocument46 pagesAcute PancreatitisLew NianNo ratings yet
- Upper and Lower GI Bleeding DR LC 21 May 2019Document36 pagesUpper and Lower GI Bleeding DR LC 21 May 2019jialeongNo ratings yet
- Carcinoma Penis: Pravin NarkhedeDocument36 pagesCarcinoma Penis: Pravin Narkhedepravin narkhede100% (1)
- Approach To Patient With GI BleedDocument22 pagesApproach To Patient With GI BleedZaidatul Atiqah Mustafa100% (1)
- PR BleedDocument20 pagesPR BleedCathy KayNo ratings yet
- Inflammatory Bowel Disease: DefinitionDocument4 pagesInflammatory Bowel Disease: Definitionkarl abiaadNo ratings yet
- EdemaDocument3 pagesEdemaUdaya SreeNo ratings yet
- Blunt AbdominalDocument39 pagesBlunt AbdominalIgnatius JesinNo ratings yet
- Abdominal PainDocument23 pagesAbdominal PainC Dimacali100% (1)
- Liver Abscess Clinical Presentation - History, Physical Examination, ComplicationsDocument2 pagesLiver Abscess Clinical Presentation - History, Physical Examination, ComplicationsAdi Kurnia100% (1)
- Carcinoma Pancreas: Risk Factors: (A) Demographic FactorsDocument4 pagesCarcinoma Pancreas: Risk Factors: (A) Demographic FactorsSakthi Annamalai.cNo ratings yet
- The Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument19 pagesThe Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PAAnonymous D29e00No ratings yet
- Gallbladder HydropsDocument6 pagesGallbladder HydropsSaifulAnamNo ratings yet
- Approach To The Patient With Hematuria: Paul D. Simmons, MD St. Mary's Family Medicine Residency Grand JunctionDocument41 pagesApproach To The Patient With Hematuria: Paul D. Simmons, MD St. Mary's Family Medicine Residency Grand JunctionMichael Spica RampangileiNo ratings yet
- Kholesistis & Kholelitiasis 30-11-14Document67 pagesKholesistis & Kholelitiasis 30-11-14Dian AzhariaNo ratings yet
- Liver Function Tests (Sem)Document6 pagesLiver Function Tests (Sem)Francisco NiegasNo ratings yet
- Urinary Tract CalculiDocument34 pagesUrinary Tract CalculiOnkar SinghNo ratings yet
- Acute AbdomenDocument8 pagesAcute Abdomenarum1992No ratings yet
- Clinical Science Section Acute Abdomen: Preseptor: Dr. Liza Nursanty, SPB, Mkes, FinacsDocument40 pagesClinical Science Section Acute Abdomen: Preseptor: Dr. Liza Nursanty, SPB, Mkes, FinacsPraluki HerliawanNo ratings yet
- Nephritic Syndrome - Armando HasudunganDocument14 pagesNephritic Syndrome - Armando HasudunganzahraaNo ratings yet
- Case of Obstructive JaundiceDocument38 pagesCase of Obstructive JaundiceadiNo ratings yet
- Kerosene PoisoningDocument12 pagesKerosene PoisoningTheRHIC21No ratings yet
- Carcinoma StomachDocument43 pagesCarcinoma StomachRukman Mecca100% (1)
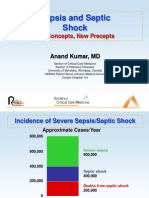
- Sepsis and Septic Shock: Old Concepts, New PreceptsDocument44 pagesSepsis and Septic Shock: Old Concepts, New PreceptsEllagEszNo ratings yet
- Pancreatic Cancer: Pathophysiologic EtiologyDocument2 pagesPancreatic Cancer: Pathophysiologic EtiologyCharissa Magistrado De LeonNo ratings yet
- Liver AbscessDocument19 pagesLiver AbscessAdi TrisnoNo ratings yet
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDocument21 pagesCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasNo ratings yet
- Presentation JaundiceDocument49 pagesPresentation JaundiceVinoth KumarNo ratings yet
- Acute Abdomen &peritonitisDocument63 pagesAcute Abdomen &peritonitisSamar Ahmad100% (1)
- 54.the Gallbladder and Bile DuctsDocument19 pages54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondNo ratings yet
- Peptic Ulcer DiseaseDocument18 pagesPeptic Ulcer DiseasechetankumarbhumireddyNo ratings yet
- Swellings ExaminationDocument3 pagesSwellings ExaminationParthik PatelNo ratings yet
- 6 Kuliah Liver CirrhosisDocument55 pages6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Validation InstrumentsDocument71 pagesValidation InstrumentsJetco LawNo ratings yet
- Case Report: Guillain - Barré Syndrome Associated With Zika Virus Infection in A Traveler Returning From GuyanaDocument5 pagesCase Report: Guillain - Barré Syndrome Associated With Zika Virus Infection in A Traveler Returning From GuyanaMuhamad RockystankiNo ratings yet
- Carski RezDocument56 pagesCarski RezArmin KoraćNo ratings yet
- Module 2 Report Priority Diseases, Conditions and Events Aug11th 2020Document52 pagesModule 2 Report Priority Diseases, Conditions and Events Aug11th 2020Solomon Fallah Foa SandyNo ratings yet
- Dietary Protein Supplementation in The Elderly For Limiting Muscle Mass LossDocument15 pagesDietary Protein Supplementation in The Elderly For Limiting Muscle Mass LossAndres Felipe Quimbayo CifuentesNo ratings yet
- Diversity of AntibodiesDocument6 pagesDiversity of AntibodiesStudiomisttNo ratings yet
- Government Policies and Initiatives ForDocument7 pagesGovernment Policies and Initiatives ForrahulNo ratings yet
- Coran - PS, 7th - Chapter 77 - Undescended Testis, Torsion, and VaricoceleDocument17 pagesCoran - PS, 7th - Chapter 77 - Undescended Testis, Torsion, and VaricoceleJessyMomoNo ratings yet
- A Review On Nutraceuticals: Classification and Its Role in Various DiseaseDocument10 pagesA Review On Nutraceuticals: Classification and Its Role in Various DiseasePrakash RoyNo ratings yet
- Triangulation of Breast Lesions: Review and Clinical ApplicationsDocument14 pagesTriangulation of Breast Lesions: Review and Clinical ApplicationsMuriloNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSherree Hayes100% (3)
- Venus EffectDocument5 pagesVenus Effectshailendra100% (1)
- IugrDocument5 pagesIugrvincentsharonNo ratings yet
- Hand Cleaning and Sanitizing: Sanitation TechnologiesDocument2 pagesHand Cleaning and Sanitizing: Sanitation Technologiesmdlc6878No ratings yet
- Grade 5 Daily Lesson Log: ST STDocument3 pagesGrade 5 Daily Lesson Log: ST STangela u bizNo ratings yet
- Mandagni Is The Root Cause For All Diseases According To Ayurvedic & Allopathic ViewsDocument8 pagesMandagni Is The Root Cause For All Diseases According To Ayurvedic & Allopathic ViewsmasdfgNo ratings yet
- Skin Structure and FunctionsDocument31 pagesSkin Structure and FunctionsAfifa Prima Gitta100% (2)
- HNF 41 - A Case Study On A 1 Year and 8 Month Old Infant Diagnosed With Acute Gastroenteritis With Moderate Dehydration and Intestinal ParasitismDocument25 pagesHNF 41 - A Case Study On A 1 Year and 8 Month Old Infant Diagnosed With Acute Gastroenteritis With Moderate Dehydration and Intestinal ParasitismIna KalawNo ratings yet
- 18 - Management of Bone and Soft Tissue Tumors 2Document18 pages18 - Management of Bone and Soft Tissue Tumors 2reeem1 alshehri2No ratings yet
- Sex Doll Porn ReviewDocument3 pagesSex Doll Porn ReviewWeb MasterNo ratings yet
- Pharmacology of Drugs Acting On Uterus - MBBSDocument23 pagesPharmacology of Drugs Acting On Uterus - MBBSDr.U.P.Rathnakar.MD.DIH.PGDHM100% (5)
- Opt Halm OlogyDocument87 pagesOpt Halm OlogyAya MahmoudNo ratings yet
- Children Ethical Marketing Issue-2Document8 pagesChildren Ethical Marketing Issue-2Muhammad Imran MustafaNo ratings yet
- Applications of MicrobiologyDocument5 pagesApplications of MicrobiologyLloyd LozanoNo ratings yet
- IVIG RateDocument2 pagesIVIG RatelydiasusantiNo ratings yet
- Hardy-Weinberg Principle WebquestDocument6 pagesHardy-Weinberg Principle Webquestapi-232072092No ratings yet
- Mandibulasr Truma ManagementDocument18 pagesMandibulasr Truma Managementjoal510No ratings yet