
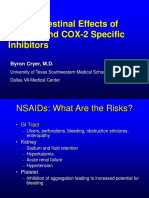
GI Effects of NSAIDs and COX-2 Specific Inhibitors - 2005-4090S1 - 02 - FDA - Cryer
GI Effects of NSAIDs and COX-2 Specific Inhibitors - 2005-4090S1 - 02 - FDA - Cryer
You might also like
- Business & Marketing PortfolioDocument28 pagesBusiness & Marketing PortfolioByng Sumague100% (3)
- 03 PsoriasisDocument28 pages03 PsoriasisGlen Lester ChiongNo ratings yet
- Bruxism Hypnosis Script No. 2Document12 pagesBruxism Hypnosis Script No. 2Eva Jacinto100% (2)
- Chapter 39 Pain Management in ChildrenDocument3 pagesChapter 39 Pain Management in ChildrenAllyssa Mackinnon0% (1)
- Care PlanningDocument14 pagesCare PlanningpriscellaNo ratings yet
- NCP Pain1Document4 pagesNCP Pain1java_biscocho12290% (1)
- Gastrointestinal Effects of Nsaids and Cox-2 Specific InhibitorsDocument43 pagesGastrointestinal Effects of Nsaids and Cox-2 Specific InhibitorsPutri WulandariNo ratings yet
- Management of Ibd - 15 March y MikhailDocument49 pagesManagement of Ibd - 15 March y Mikhailjordanmedics100% (1)
- Risks of Nsaids: Focus On Gi Risks of Over-The-Counter NsaidsDocument40 pagesRisks of Nsaids: Focus On Gi Risks of Over-The-Counter Nsaidspaul_calburean7899No ratings yet
- Lecture 16 GERDDocument44 pagesLecture 16 GERDSinthuNo ratings yet
- Raffaele Pezzilli, Lorenzo Fantini, Antonio Maria Morselli-LabateDocument51 pagesRaffaele Pezzilli, Lorenzo Fantini, Antonio Maria Morselli-LabateLeonNo ratings yet
- G I Toxicity of NSAIDsDocument59 pagesG I Toxicity of NSAIDsPann EiNo ratings yet
- Nonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Document32 pagesNonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Saad MotawéaNo ratings yet
- Inflammatory Bowel Disease RK2012Document212 pagesInflammatory Bowel Disease RK2012Nurul Kartika SariNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- NSAID Colon UlcersDocument5 pagesNSAID Colon UlcersFrederic IkkiNo ratings yet
- Stomach and Duodenum (Forsharing)Document79 pagesStomach and Duodenum (Forsharing)adversal8avrikNo ratings yet
- Effect of A Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease On Postoperative Nausea and VomitingDocument9 pagesEffect of A Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease On Postoperative Nausea and VomitingINICUOMNo ratings yet
- 3.a. Peptic Ulcer (DR - Fauzi Yusuf, SP - PD, KGEH)Document18 pages3.a. Peptic Ulcer (DR - Fauzi Yusuf, SP - PD, KGEH)Irfandy Chairi Sulaiman LubisNo ratings yet
- GERDDocument47 pagesGERDSutanto TanakaNo ratings yet
- Summary and Conclusions: Urinary Biomarkers in Experimental DiabetesDocument1 pageSummary and Conclusions: Urinary Biomarkers in Experimental DiabetesNikesh DoshiNo ratings yet
- CYP2C9 Polymorphism in Non-Steroidal Anti-Inflammatory Drugs-Induced GastropathyDocument6 pagesCYP2C9 Polymorphism in Non-Steroidal Anti-Inflammatory Drugs-Induced GastropathyFariz NurNo ratings yet
- Gerd - NCCP - Kppik 2011 (Hotel Shangri La)Document28 pagesGerd - NCCP - Kppik 2011 (Hotel Shangri La)Fatmala HaningtyasNo ratings yet
- CPD Januari 2013Document36 pagesCPD Januari 2013ledyNo ratings yet
- Iwamoto Et Al 2014 - DigestiveDocument7 pagesIwamoto Et Al 2014 - Digestivemattlight07No ratings yet
- Fever Cough and Fungal Infection (FARM)Document20 pagesFever Cough and Fungal Infection (FARM)Balamurugan KGNo ratings yet
- Crohns DiseaseDocument72 pagesCrohns Diseasea1savedNo ratings yet
- Case Presentation On Gut ObstructionDocument19 pagesCase Presentation On Gut Obstructionlakshitataneja1998No ratings yet
- Ge Reflux-MedDocument31 pagesGe Reflux-Medyour babysurgeonNo ratings yet
- Inflammatory DisturbancesDocument63 pagesInflammatory DisturbancesWang Ming YaNo ratings yet
- Enteral Nutrition Therapy For The Surgical PatientDocument52 pagesEnteral Nutrition Therapy For The Surgical PatientelenNo ratings yet
- Art 1 HT3Document3 pagesArt 1 HT3Glenda MaríaNo ratings yet
- Rheumatology Journal Club Gut Vasculitis: by DR Nur Hidayati Mohd SharifDocument36 pagesRheumatology Journal Club Gut Vasculitis: by DR Nur Hidayati Mohd SharifEida MohdNo ratings yet
- Gerd (Gastroesophageal Reflux DiseaseDocument43 pagesGerd (Gastroesophageal Reflux DiseaseRoselin Megasari MendrofaNo ratings yet
- Inflammatory Bowel Disease 5th YearDocument72 pagesInflammatory Bowel Disease 5th YearAi NurfaiziyahNo ratings yet
- Crohns DiseaseDocument72 pagesCrohns DiseaseFlavia CunhaNo ratings yet
- Usefulness of Vonoprazan, A Potassium Ion-Competitive Acid Blocker, For Primary Eradication of HelicobacterDocument8 pagesUsefulness of Vonoprazan, A Potassium Ion-Competitive Acid Blocker, For Primary Eradication of HelicobacterUlilta MuktadiraNo ratings yet
- GERD Med StudentsaaaasdDocument54 pagesGERD Med StudentsaaaasdAlifiyanFithriyanaNo ratings yet
- GERD PathophysiologyDocument35 pagesGERD PathophysiologyKathlea Noble-dc100% (1)
- Upper Gastrointestinal Bleeding: (UGIB)Document39 pagesUpper Gastrointestinal Bleeding: (UGIB)api-19916399No ratings yet
- A6. Tukak PeptikDocument31 pagesA6. Tukak PeptikSartika NapitupuluNo ratings yet
- Assignment: Applied MedicineDocument10 pagesAssignment: Applied MedicineKhadija BakhtawarNo ratings yet
- INTRO - Types: Chron'sDocument47 pagesINTRO - Types: Chron'sfadliNo ratings yet
- Cco Gi CR 2013 SlidesDocument48 pagesCco Gi CR 2013 SlidesArtemSakhnoNo ratings yet
- Care Plan SBO VomingDocument6 pagesCare Plan SBO Vomingstring44No ratings yet
- 1430 - Falk - GERD 222Document34 pages1430 - Falk - GERD 222Tengku Novia Eka PutriNo ratings yet
- The Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasDocument29 pagesThe Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallaskitsilcNo ratings yet
- CP ON PUD (1) ADocument20 pagesCP ON PUD (1) ADeekshitha DanthuluriNo ratings yet
- 1 Recently Approved AntibioticsDocument29 pages1 Recently Approved Antibioticslpa.ufmt.enfNo ratings yet
- Evidence-Based Nursing: Submitted By: de Guzman, Tammy S. de Leon, Jenalyn C. BSN113Document6 pagesEvidence-Based Nursing: Submitted By: de Guzman, Tammy S. de Leon, Jenalyn C. BSN113tammy_deguzman5223No ratings yet
- Cancer Gastrico AvancesDocument48 pagesCancer Gastrico AvancesSeal MachucaNo ratings yet
- Gastrointestinal Hemorrhage in The ICU: Doctor Chad Pulmonary & Critical Care MedicineDocument49 pagesGastrointestinal Hemorrhage in The ICU: Doctor Chad Pulmonary & Critical Care MedicinechadchimaNo ratings yet
- Exmd 509 Mcgill Stomach 2016Document36 pagesExmd 509 Mcgill Stomach 2016Sora OhNo ratings yet
- Pain Talk VipondDocument39 pagesPain Talk VipondHelmi IsmunandarNo ratings yet
- Case Presentation: Clostridium DifficileDocument35 pagesCase Presentation: Clostridium DifficileDnse LucidoNo ratings yet
- Molitch - Hot Topics Cushings Disease and AcromegalyDocument69 pagesMolitch - Hot Topics Cushings Disease and AcromegalyMaryONo ratings yet
- Empirical Treatment With PPI in Acid Related DiseaseDocument41 pagesEmpirical Treatment With PPI in Acid Related DiseaseAyu Yunita Jaury HRNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Engin AltınkayaNo ratings yet
- Acute Pancreatitis: Some Important Issues RevisitedDocument109 pagesAcute Pancreatitis: Some Important Issues RevisitedjlaguilarNo ratings yet
- 0830 - Ravi Esoph-Sm BWLDocument49 pages0830 - Ravi Esoph-Sm BWLAlejandro Kanito Alvarez SNo ratings yet
- Barb Melo SkyDocument17 pagesBarb Melo SkyAfiqah So JasmiNo ratings yet
- Acute Gastrointestinal Bleeding: Diagnosis and TreatmentFrom EverandAcute Gastrointestinal Bleeding: Diagnosis and TreatmentKaren E. KimNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- LidocaineDocument11 pagesLidocaineStanford AnesthesiaNo ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- 2019 Aiken County Accidental OverdosesDocument1 page2019 Aiken County Accidental OverdosesJeremy TurnageNo ratings yet
- Homeopathy and PainDocument9 pagesHomeopathy and Painoana777No ratings yet
- In Diagnosis and Therapy: More FreedomDocument7 pagesIn Diagnosis and Therapy: More FreedomHaydar Ali FidanNo ratings yet
- 13 NBNS1214 T9 PDFDocument17 pages13 NBNS1214 T9 PDFNur NazurahNo ratings yet
- NP1 - ToprankDocument16 pagesNP1 - ToprankAllaiza Cristille100% (1)
- TKR RehabilitationDocument1 pageTKR RehabilitationgursangeetNo ratings yet
- Respiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition Jane Cross All ChapterDocument68 pagesRespiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition Jane Cross All Chaptervincent.pathak166100% (14)
- Fluoxetina Medimart 20 MG 40 TabletasDocument51 pagesFluoxetina Medimart 20 MG 40 TabletasJose Manuel Rito GonzalezNo ratings yet
- Concept Map MgenoviaDocument5 pagesConcept Map Mgenoviaapi-302138606No ratings yet
- 01 - File List - Content Last Upload - 10.04.2019Document107 pages01 - File List - Content Last Upload - 10.04.2019FlorentinaDinNo ratings yet
- 2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINDocument5 pages2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINZahirah BudimanNo ratings yet
- Ef Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-AnalysisDocument7 pagesEf Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-Analysisxian karachiNo ratings yet
- Principles of Pain Management: Pediatric GuideDocument2 pagesPrinciples of Pain Management: Pediatric Guideblaziken123No ratings yet
- Mindfulness For Chronic Pain ManagementDocument4 pagesMindfulness For Chronic Pain Managementrasanka2014No ratings yet
- Clinical Guidelines For NarcoticsDocument4 pagesClinical Guidelines For NarcoticsClara VerlinaNo ratings yet
- That ApplyDocument7 pagesThat ApplyJona BartzNo ratings yet
- Music Therapy As A Post-OperatDocument33 pagesMusic Therapy As A Post-OperatLia octavianyNo ratings yet
- Clinical Practice Guidelines For The Sustained Use of Sedatives and Analgesics in The Critically Ill AdultDocument23 pagesClinical Practice Guidelines For The Sustained Use of Sedatives and Analgesics in The Critically Ill AdultMontse Gorchs MolistNo ratings yet
- Legal Aspects in PC HandbookDocument60 pagesLegal Aspects in PC Handbookike setiawanNo ratings yet
- Cambridge English For Nursing Medical Technology Intermediate Unit9 WorksheetDocument1 pageCambridge English For Nursing Medical Technology Intermediate Unit9 WorksheetJernej LapanjeNo ratings yet
- 2021 Update Management Pain (Dokter & Medical)Document30 pages2021 Update Management Pain (Dokter & Medical)Andri MuliaNo ratings yet
- House MD PDFDocument10 pagesHouse MD PDFMax1929No ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Expected Outcomes Interventions Rationale EvaluationDocument7 pagesNursing Care Plan Assessment Nursing Diagnosis Expected Outcomes Interventions Rationale Evaluationلمى الشهريNo ratings yet






















































































Download as ppt, pdf, or txt
You might also like
- Business & Marketing PortfolioDocument28 pagesBusiness & Marketing PortfolioByng Sumague100% (3)
- 03 PsoriasisDocument28 pages03 PsoriasisGlen Lester ChiongNo ratings yet
- Bruxism Hypnosis Script No. 2Document12 pagesBruxism Hypnosis Script No. 2Eva Jacinto100% (2)
- Chapter 39 Pain Management in ChildrenDocument3 pagesChapter 39 Pain Management in ChildrenAllyssa Mackinnon0% (1)
- Care PlanningDocument14 pagesCare PlanningpriscellaNo ratings yet
- NCP Pain1Document4 pagesNCP Pain1java_biscocho12290% (1)
- Gastrointestinal Effects of Nsaids and Cox-2 Specific InhibitorsDocument43 pagesGastrointestinal Effects of Nsaids and Cox-2 Specific InhibitorsPutri WulandariNo ratings yet
- Management of Ibd - 15 March y MikhailDocument49 pagesManagement of Ibd - 15 March y Mikhailjordanmedics100% (1)
- Risks of Nsaids: Focus On Gi Risks of Over-The-Counter NsaidsDocument40 pagesRisks of Nsaids: Focus On Gi Risks of Over-The-Counter Nsaidspaul_calburean7899No ratings yet
- Lecture 16 GERDDocument44 pagesLecture 16 GERDSinthuNo ratings yet
- Raffaele Pezzilli, Lorenzo Fantini, Antonio Maria Morselli-LabateDocument51 pagesRaffaele Pezzilli, Lorenzo Fantini, Antonio Maria Morselli-LabateLeonNo ratings yet
- G I Toxicity of NSAIDsDocument59 pagesG I Toxicity of NSAIDsPann EiNo ratings yet
- Nonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Document32 pagesNonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Saad MotawéaNo ratings yet
- Inflammatory Bowel Disease RK2012Document212 pagesInflammatory Bowel Disease RK2012Nurul Kartika SariNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- NSAID Colon UlcersDocument5 pagesNSAID Colon UlcersFrederic IkkiNo ratings yet
- Stomach and Duodenum (Forsharing)Document79 pagesStomach and Duodenum (Forsharing)adversal8avrikNo ratings yet
- Effect of A Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease On Postoperative Nausea and VomitingDocument9 pagesEffect of A Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease On Postoperative Nausea and VomitingINICUOMNo ratings yet
- 3.a. Peptic Ulcer (DR - Fauzi Yusuf, SP - PD, KGEH)Document18 pages3.a. Peptic Ulcer (DR - Fauzi Yusuf, SP - PD, KGEH)Irfandy Chairi Sulaiman LubisNo ratings yet
- GERDDocument47 pagesGERDSutanto TanakaNo ratings yet
- Summary and Conclusions: Urinary Biomarkers in Experimental DiabetesDocument1 pageSummary and Conclusions: Urinary Biomarkers in Experimental DiabetesNikesh DoshiNo ratings yet
- CYP2C9 Polymorphism in Non-Steroidal Anti-Inflammatory Drugs-Induced GastropathyDocument6 pagesCYP2C9 Polymorphism in Non-Steroidal Anti-Inflammatory Drugs-Induced GastropathyFariz NurNo ratings yet
- Gerd - NCCP - Kppik 2011 (Hotel Shangri La)Document28 pagesGerd - NCCP - Kppik 2011 (Hotel Shangri La)Fatmala HaningtyasNo ratings yet
- CPD Januari 2013Document36 pagesCPD Januari 2013ledyNo ratings yet
- Iwamoto Et Al 2014 - DigestiveDocument7 pagesIwamoto Et Al 2014 - Digestivemattlight07No ratings yet
- Fever Cough and Fungal Infection (FARM)Document20 pagesFever Cough and Fungal Infection (FARM)Balamurugan KGNo ratings yet
- Crohns DiseaseDocument72 pagesCrohns Diseasea1savedNo ratings yet
- Case Presentation On Gut ObstructionDocument19 pagesCase Presentation On Gut Obstructionlakshitataneja1998No ratings yet
- Ge Reflux-MedDocument31 pagesGe Reflux-Medyour babysurgeonNo ratings yet
- Inflammatory DisturbancesDocument63 pagesInflammatory DisturbancesWang Ming YaNo ratings yet
- Enteral Nutrition Therapy For The Surgical PatientDocument52 pagesEnteral Nutrition Therapy For The Surgical PatientelenNo ratings yet
- Art 1 HT3Document3 pagesArt 1 HT3Glenda MaríaNo ratings yet
- Rheumatology Journal Club Gut Vasculitis: by DR Nur Hidayati Mohd SharifDocument36 pagesRheumatology Journal Club Gut Vasculitis: by DR Nur Hidayati Mohd SharifEida MohdNo ratings yet
- Gerd (Gastroesophageal Reflux DiseaseDocument43 pagesGerd (Gastroesophageal Reflux DiseaseRoselin Megasari MendrofaNo ratings yet
- Inflammatory Bowel Disease 5th YearDocument72 pagesInflammatory Bowel Disease 5th YearAi NurfaiziyahNo ratings yet
- Crohns DiseaseDocument72 pagesCrohns DiseaseFlavia CunhaNo ratings yet
- Usefulness of Vonoprazan, A Potassium Ion-Competitive Acid Blocker, For Primary Eradication of HelicobacterDocument8 pagesUsefulness of Vonoprazan, A Potassium Ion-Competitive Acid Blocker, For Primary Eradication of HelicobacterUlilta MuktadiraNo ratings yet
- GERD Med StudentsaaaasdDocument54 pagesGERD Med StudentsaaaasdAlifiyanFithriyanaNo ratings yet
- GERD PathophysiologyDocument35 pagesGERD PathophysiologyKathlea Noble-dc100% (1)
- Upper Gastrointestinal Bleeding: (UGIB)Document39 pagesUpper Gastrointestinal Bleeding: (UGIB)api-19916399No ratings yet
- A6. Tukak PeptikDocument31 pagesA6. Tukak PeptikSartika NapitupuluNo ratings yet
- Assignment: Applied MedicineDocument10 pagesAssignment: Applied MedicineKhadija BakhtawarNo ratings yet
- INTRO - Types: Chron'sDocument47 pagesINTRO - Types: Chron'sfadliNo ratings yet
- Cco Gi CR 2013 SlidesDocument48 pagesCco Gi CR 2013 SlidesArtemSakhnoNo ratings yet
- Care Plan SBO VomingDocument6 pagesCare Plan SBO Vomingstring44No ratings yet
- 1430 - Falk - GERD 222Document34 pages1430 - Falk - GERD 222Tengku Novia Eka PutriNo ratings yet
- The Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasDocument29 pagesThe Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallaskitsilcNo ratings yet
- CP ON PUD (1) ADocument20 pagesCP ON PUD (1) ADeekshitha DanthuluriNo ratings yet
- 1 Recently Approved AntibioticsDocument29 pages1 Recently Approved Antibioticslpa.ufmt.enfNo ratings yet
- Evidence-Based Nursing: Submitted By: de Guzman, Tammy S. de Leon, Jenalyn C. BSN113Document6 pagesEvidence-Based Nursing: Submitted By: de Guzman, Tammy S. de Leon, Jenalyn C. BSN113tammy_deguzman5223No ratings yet
- Cancer Gastrico AvancesDocument48 pagesCancer Gastrico AvancesSeal MachucaNo ratings yet
- Gastrointestinal Hemorrhage in The ICU: Doctor Chad Pulmonary & Critical Care MedicineDocument49 pagesGastrointestinal Hemorrhage in The ICU: Doctor Chad Pulmonary & Critical Care MedicinechadchimaNo ratings yet
- Exmd 509 Mcgill Stomach 2016Document36 pagesExmd 509 Mcgill Stomach 2016Sora OhNo ratings yet
- Pain Talk VipondDocument39 pagesPain Talk VipondHelmi IsmunandarNo ratings yet
- Case Presentation: Clostridium DifficileDocument35 pagesCase Presentation: Clostridium DifficileDnse LucidoNo ratings yet
- Molitch - Hot Topics Cushings Disease and AcromegalyDocument69 pagesMolitch - Hot Topics Cushings Disease and AcromegalyMaryONo ratings yet
- Empirical Treatment With PPI in Acid Related DiseaseDocument41 pagesEmpirical Treatment With PPI in Acid Related DiseaseAyu Yunita Jaury HRNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Engin AltınkayaNo ratings yet
- Acute Pancreatitis: Some Important Issues RevisitedDocument109 pagesAcute Pancreatitis: Some Important Issues RevisitedjlaguilarNo ratings yet
- 0830 - Ravi Esoph-Sm BWLDocument49 pages0830 - Ravi Esoph-Sm BWLAlejandro Kanito Alvarez SNo ratings yet
- Barb Melo SkyDocument17 pagesBarb Melo SkyAfiqah So JasmiNo ratings yet
- Acute Gastrointestinal Bleeding: Diagnosis and TreatmentFrom EverandAcute Gastrointestinal Bleeding: Diagnosis and TreatmentKaren E. KimNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- LidocaineDocument11 pagesLidocaineStanford AnesthesiaNo ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- 2019 Aiken County Accidental OverdosesDocument1 page2019 Aiken County Accidental OverdosesJeremy TurnageNo ratings yet
- Homeopathy and PainDocument9 pagesHomeopathy and Painoana777No ratings yet
- In Diagnosis and Therapy: More FreedomDocument7 pagesIn Diagnosis and Therapy: More FreedomHaydar Ali FidanNo ratings yet
- 13 NBNS1214 T9 PDFDocument17 pages13 NBNS1214 T9 PDFNur NazurahNo ratings yet
- NP1 - ToprankDocument16 pagesNP1 - ToprankAllaiza Cristille100% (1)
- TKR RehabilitationDocument1 pageTKR RehabilitationgursangeetNo ratings yet
- Respiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition Jane Cross All ChapterDocument68 pagesRespiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition Jane Cross All Chaptervincent.pathak166100% (14)
- Fluoxetina Medimart 20 MG 40 TabletasDocument51 pagesFluoxetina Medimart 20 MG 40 TabletasJose Manuel Rito GonzalezNo ratings yet
- Concept Map MgenoviaDocument5 pagesConcept Map Mgenoviaapi-302138606No ratings yet
- 01 - File List - Content Last Upload - 10.04.2019Document107 pages01 - File List - Content Last Upload - 10.04.2019FlorentinaDinNo ratings yet
- 2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINDocument5 pages2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINZahirah BudimanNo ratings yet
- Ef Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-AnalysisDocument7 pagesEf Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-Analysisxian karachiNo ratings yet
- Principles of Pain Management: Pediatric GuideDocument2 pagesPrinciples of Pain Management: Pediatric Guideblaziken123No ratings yet
- Mindfulness For Chronic Pain ManagementDocument4 pagesMindfulness For Chronic Pain Managementrasanka2014No ratings yet
- Clinical Guidelines For NarcoticsDocument4 pagesClinical Guidelines For NarcoticsClara VerlinaNo ratings yet
- That ApplyDocument7 pagesThat ApplyJona BartzNo ratings yet
- Music Therapy As A Post-OperatDocument33 pagesMusic Therapy As A Post-OperatLia octavianyNo ratings yet
- Clinical Practice Guidelines For The Sustained Use of Sedatives and Analgesics in The Critically Ill AdultDocument23 pagesClinical Practice Guidelines For The Sustained Use of Sedatives and Analgesics in The Critically Ill AdultMontse Gorchs MolistNo ratings yet
- Legal Aspects in PC HandbookDocument60 pagesLegal Aspects in PC Handbookike setiawanNo ratings yet
- Cambridge English For Nursing Medical Technology Intermediate Unit9 WorksheetDocument1 pageCambridge English For Nursing Medical Technology Intermediate Unit9 WorksheetJernej LapanjeNo ratings yet
- 2021 Update Management Pain (Dokter & Medical)Document30 pages2021 Update Management Pain (Dokter & Medical)Andri MuliaNo ratings yet
- House MD PDFDocument10 pagesHouse MD PDFMax1929No ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Expected Outcomes Interventions Rationale EvaluationDocument7 pagesNursing Care Plan Assessment Nursing Diagnosis Expected Outcomes Interventions Rationale Evaluationلمى الشهريNo ratings yet