Download as pptx, pdf, or txt
You might also like
- Itrace 4 - 1 Users Manual - IFU 7.5-4-2 RevADocument76 pagesItrace 4 - 1 Users Manual - IFU 7.5-4-2 RevAbanklee010163.com75% (4)
- Malingering in Ophthalmology TestDocument7 pagesMalingering in Ophthalmology TestmasmedicaNo ratings yet
- Anatomi Dan Embriologi Mata: Setia PepetDocument31 pagesAnatomi Dan Embriologi Mata: Setia PepetDi Hati Alonelly SetiaPepetNo ratings yet
- Dme C1Document7 pagesDme C1taliya. shvetzNo ratings yet
- The Lens - Applied Anatomy and Embryology: Chapter - 1Document7 pagesThe Lens - Applied Anatomy and Embryology: Chapter - 1Reza AkbarNo ratings yet
- Physiology of Eye. Physiology of VisionDocument27 pagesPhysiology of Eye. Physiology of VisionSmartcool So100% (1)
- Final TouchDocument49 pagesFinal TouchmalathiNo ratings yet
- Marie Belen C. Tamayor, RNDocument42 pagesMarie Belen C. Tamayor, RNrein_seanNo ratings yet
- Structure of EyeDocument24 pagesStructure of Eyedipendrakumarkushawaha44No ratings yet
- Glaucoma 180813151731Document24 pagesGlaucoma 180813151731malathiNo ratings yet
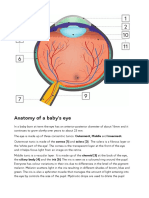
- Anatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orDocument2 pagesAnatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orSandor GyongyverNo ratings yet
- The Crystalline LensDocument22 pagesThe Crystalline LensSuhaila El MuzoghiNo ratings yet
- Lens's Physiology PDFDocument46 pagesLens's Physiology PDFamriashshiddieqNo ratings yet
- Abnormal Pupil, How To DoDocument8 pagesAbnormal Pupil, How To DoUNHAS OphthalmologyNo ratings yet
- The Anatomy & Physiology of Lens: DR Prabhjot SinghDocument76 pagesThe Anatomy & Physiology of Lens: DR Prabhjot SinghPrabhjot SinghNo ratings yet
- Si Kodhil - Lens AnatomyDocument26 pagesSi Kodhil - Lens AnatomyAndriati Nadhila100% (1)
- Eye, Ear, Nose and Throat Assessment and Disorders Final PPT, NursingDocument489 pagesEye, Ear, Nose and Throat Assessment and Disorders Final PPT, NursingFirifan Diriba100% (1)
- Eye and Ear Assessment and DisordersDocument374 pagesEye and Ear Assessment and DisordersFirifan DiribaNo ratings yet
- Examination of The EyeDocument16 pagesExamination of The EyeRoxana SurliuNo ratings yet
- OCULAR PHYSIOLOGY 2021 Section B 2Document46 pagesOCULAR PHYSIOLOGY 2021 Section B 2Divine OkolieNo ratings yet
- (L-2) - Eye - Nov 12, 2019Document54 pages(L-2) - Eye - Nov 12, 2019Sejal PrasadNo ratings yet
- Makalah Miopi Bahasa InggrisDocument16 pagesMakalah Miopi Bahasa InggrisDhewii Amelya MiissLoversNo ratings yet
- Organs of VisionDocument3 pagesOrgans of VisionNarasimha Murthy100% (1)
- The Eye and Its DiseasesDocument33 pagesThe Eye and Its DiseasesbeedgaiNo ratings yet
- SASDocument10 pagesSASNicole Ken AgdanaNo ratings yet
- Anatomy of Eye - WebinarDocument57 pagesAnatomy of Eye - Webinarvigneshvaraprabhu.ayothiNo ratings yet
- Dr. Sashwat RayDocument98 pagesDr. Sashwat RayDikshant DaswatNo ratings yet
- A Project On " Human Eye": Submitted To-Submitted byDocument13 pagesA Project On " Human Eye": Submitted To-Submitted byaman1990100% (1)
- Anatomi Dan Embriologi Mata: Julie D BarlianaDocument31 pagesAnatomi Dan Embriologi Mata: Julie D BarlianaAyunita PermataNo ratings yet
- Cataract Green Group A1Document58 pagesCataract Green Group A1Jerry GohNo ratings yet
- EYESSDocument43 pagesEYESSsalwanaseer9999No ratings yet
- Dr. Sashwat Ray IsmDocument98 pagesDr. Sashwat Ray IsmCastleKGNo ratings yet
- Anatomy of The Eye Physiology of The Visual FunctionsDocument27 pagesAnatomy of The Eye Physiology of The Visual Functionssomebody_maNo ratings yet
- Eyes Health AssessmenttDocument34 pagesEyes Health AssessmenttMhiaBuenafeNo ratings yet
- Anatomy and Uss Appearance of The EyeDocument53 pagesAnatomy and Uss Appearance of The EyeLoverage NyandoroNo ratings yet
- Visualimpairment 141110001816 Conversion Gate02Document44 pagesVisualimpairment 141110001816 Conversion Gate02jessajoy deslateNo ratings yet
- Pig EyeDocument6 pagesPig Eyeaims_sluNo ratings yet
- 04 The Uveal TractDocument8 pages04 The Uveal TractmoraadoreneNo ratings yet
- Anatomy-Physiology Eyeball 2023Document75 pagesAnatomy-Physiology Eyeball 2023debdeepbhattacharya411No ratings yet
- Asvs 04 0267Document7 pagesAsvs 04 0267T KNo ratings yet
- (L-1) - Eye - Nov 11, 2019Document37 pages(L-1) - Eye - Nov 11, 2019HanzalaNo ratings yet
- Jarvis: Physical Examination & Health Assessment, 3rd Canadian EditionDocument3 pagesJarvis: Physical Examination & Health Assessment, 3rd Canadian EditionkekeNo ratings yet
- Ibd Bio OptikDocument19 pagesIbd Bio Optik백이MOONNo ratings yet
- Sense Organs NotesDocument13 pagesSense Organs NotesVijay Laxmi MundhraNo ratings yet
- EyeballDocument14 pagesEyeballMirko BelanNo ratings yet
- Anatomy Physiology Visual System April 2014Document41 pagesAnatomy Physiology Visual System April 2014levianaNo ratings yet
- Case Study 1Document21 pagesCase Study 1Michel BalsoteNo ratings yet
- Chapter 5 Crystalline Lens - Abdelmonem Hamed EditionDocument16 pagesChapter 5 Crystalline Lens - Abdelmonem Hamed EditionAbdelmonem HamedNo ratings yet
- Topic Presentation CataractDocument11 pagesTopic Presentation Cataractjyoti singhNo ratings yet
- Special Senses: Dr. Salisu Ahmed Ibrahim MBBS, MSC, PHD Associate Prof of HUMAN Physiology Date: 7 September 2020Document14 pagesSpecial Senses: Dr. Salisu Ahmed Ibrahim MBBS, MSC, PHD Associate Prof of HUMAN Physiology Date: 7 September 2020Obansa JohnNo ratings yet
- 1 Anatomy & Physiology of Eye For Ophthalmic NursesDocument124 pages1 Anatomy & Physiology of Eye For Ophthalmic NursesSMEY204100% (1)
- Vision BPTDocument110 pagesVision BPTAkshay BadoreNo ratings yet
- PUPILDocument31 pagesPUPILHamza FarooqNo ratings yet
- Introduction To Ophthalmology: by DR - Bakhtiar Q. JafDocument41 pagesIntroduction To Ophthalmology: by DR - Bakhtiar Q. JafChristian JaraNo ratings yet
- UveaDocument83 pagesUveaShewit TeklehaymanotNo ratings yet
- Lecture 3 and 4 Special SensesDocument70 pagesLecture 3 and 4 Special SensesHope NdwandweNo ratings yet
- Anatomía Clínica de La Región Periocular PDFDocument10 pagesAnatomía Clínica de La Región Periocular PDFLizeth Conde OrozcoNo ratings yet
- Eye Disorder PeadsDocument51 pagesEye Disorder PeadsGrashiaNo ratings yet
- Binocular Single VisionDocument9 pagesBinocular Single VisionMarcelKorevaarNo ratings yet
- Anatomy of An EyeDocument12 pagesAnatomy of An EyeSuahniNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- Occupational Health Tips On Eye Protection For Good Visual HealthFrom EverandOccupational Health Tips On Eye Protection For Good Visual HealthNo ratings yet
- Hesi Med Surg Study GuideDocument1 pageHesi Med Surg Study GuideGeorgeNo ratings yet
- Evolution S Witness How Eyes Evolved, Ivan R .20Document1 pageEvolution S Witness How Eyes Evolved, Ivan R .20Mariana De Los Angeles Castillo RodriguezNo ratings yet
- Chapter 2 - Heterophoria, Pages 15-40Document26 pagesChapter 2 - Heterophoria, Pages 15-40blueice100% (1)
- Lighting SchemesDocument6 pagesLighting Schemespsahoo67% (3)
- Retinal Drawing: A Lost Art of MedicineDocument2 pagesRetinal Drawing: A Lost Art of MedicineManuel GallegosNo ratings yet
- Activity in Eyes ConceptDocument2 pagesActivity in Eyes ConceptWiljohn de la CruzNo ratings yet
- Biomedics Toric: Symbol DescriptionDocument2 pagesBiomedics Toric: Symbol DescriptionHemantNo ratings yet
- Dutta 2Document671 pagesDutta 2Jeel GaralaNo ratings yet
- Organizational Behavour Canadian 3rd Edition Colquitt Test BankDocument35 pagesOrganizational Behavour Canadian 3rd Edition Colquitt Test Bankconsignedurylic75hi100% (24)
- Nat Reviewer 1Document9 pagesNat Reviewer 1shiela andalNo ratings yet
- Wheel Chair Controller Using Eye Ball MovementDocument16 pagesWheel Chair Controller Using Eye Ball Movementananda kumar mNo ratings yet
- MCQ 1Document21 pagesMCQ 1rocky singhNo ratings yet
- November 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Document20 pagesNovember 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Chris SoksNo ratings yet
- SS Mu 3.1 Lores PDFDocument19 pagesSS Mu 3.1 Lores PDFThakurainChaudharyNo ratings yet
- Sense OrgansDocument8 pagesSense OrgansKeelah BennNo ratings yet
- Note-Human Eye and Colourfull WorldDocument6 pagesNote-Human Eye and Colourfull WorldjamaluddinNo ratings yet
- Optical Express Brochuresep18Document17 pagesOptical Express Brochuresep18Martin ClarkNo ratings yet
- Moorfields Referral FormDocument2 pagesMoorfields Referral Formmoiseancuta87No ratings yet
- Chapter 3: Visual Perception: Cognitive PsychologyDocument4 pagesChapter 3: Visual Perception: Cognitive PsychologyMicaella TrinidadNo ratings yet
- Complication IntraoperativeDocument5 pagesComplication IntraoperativeizzatulhasanahNo ratings yet
- Eyes and Ears DisordersDocument36 pagesEyes and Ears Disordersjeshema100% (4)
- Eye (4th Year) MCQs - Rana Haseeb 2020Document59 pagesEye (4th Year) MCQs - Rana Haseeb 2020boyziddi32No ratings yet
- اخطاء انكسار 4Document4 pagesاخطاء انكسار 4Hassan AljaberiNo ratings yet
- RetinaDocument12 pagesRetinagdudex118811No ratings yet
- Checklist Instrumen Baksos Update 28.05.23Document8 pagesChecklist Instrumen Baksos Update 28.05.23dr GheaNo ratings yet
- Retina SlidesDocument70 pagesRetina SlidesMariam QaisNo ratings yet
- Corneal DegenerationDocument1 pageCorneal Degenerationtgrrwccj98No ratings yet
- Rajvin Samuel PonrajDocument28 pagesRajvin Samuel PonrajPutri kartiniNo ratings yet