Download as pptx, pdf, or txt
You might also like
- Stroke LectureDocument48 pagesStroke Lecturebereket gashu71% (7)
- Atozet Slide Deck New-PresentationDocument49 pagesAtozet Slide Deck New-PresentationMustafa JaradatNo ratings yet
- ECG Rhythm Strip Interpretation Lesson 4Document5 pagesECG Rhythm Strip Interpretation Lesson 4phoebjaetanNo ratings yet
- Venous ThromboembolismDocument80 pagesVenous Thromboembolismtcj4bpj2pnNo ratings yet
- VTE SeminarDocument45 pagesVTE Seminarabotreka056No ratings yet
- DVT MatisseDocument31 pagesDVT MatisseMaretha Dyah AnggrainiNo ratings yet
- Deep Vein Thrombosis: Dr. Iman Haryana SPJPDocument29 pagesDeep Vein Thrombosis: Dr. Iman Haryana SPJPAuliyah SeptianiNo ratings yet
- Management of DVTDocument21 pagesManagement of DVTHaashveeni Jayan KumarNo ratings yet
- MEDIATRIXDocument67 pagesMEDIATRIXMaria Consuelo LingcasoNo ratings yet
- DVTDocument20 pagesDVTNachiket Vijay PotdarNo ratings yet
- Deep Venous Thrombosis: Farouq Muhammad 6-10-11Document59 pagesDeep Venous Thrombosis: Farouq Muhammad 6-10-11farouqmuhdNo ratings yet
- Deep Venous ThrombosisDocument56 pagesDeep Venous ThrombosisSrikant Konchada100% (1)
- +oleksandr Chaika Theme 16 Thrombosis of The Main VeinsDocument22 pages+oleksandr Chaika Theme 16 Thrombosis of The Main VeinsOussama ANo ratings yet
- Swelling in LegDocument3 pagesSwelling in LegNeeraj SethiNo ratings yet
- Deep Vein ThrombosisDocument42 pagesDeep Vein ThrombosisNsklm100% (7)
- Kuliah Thrombosis 2015 NNDocument39 pagesKuliah Thrombosis 2015 NNBeladiena Citra SiregarNo ratings yet
- Dvt. BPTDocument25 pagesDvt. BPTAanchal GuptaNo ratings yet
- Thrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Document39 pagesThrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Ericka SantosNo ratings yet
- Vein PathologyDocument44 pagesVein PathologyEma RadulescuNo ratings yet
- Did You Know?Document12 pagesDid You Know?ShilpaNo ratings yet
- DEEP VEIN Dr. Samira BelkheirDocument43 pagesDEEP VEIN Dr. Samira BelkheirkalfNo ratings yet
- Cardiovascular-Disorders Group4 3NFDocument10 pagesCardiovascular-Disorders Group4 3NFDarren RobertoNo ratings yet
- Irh Presentation DVT AssDocument52 pagesIrh Presentation DVT AssJoseph MuzabulaNo ratings yet
- Superficial Venous Thrombophlebitis: Presented by - Nader SaadDocument24 pagesSuperficial Venous Thrombophlebitis: Presented by - Nader SaadNader SaadNo ratings yet
- DEEP Vein ThrombosisDocument72 pagesDEEP Vein ThrombosisLevy Garcia SanchezNo ratings yet
- Wells Score For DVT ProbabilityDocument10 pagesWells Score For DVT ProbabilityrhomadianaNo ratings yet
- Venous ThromboembolismDocument11 pagesVenous ThromboembolismPindha Kurnia JatiNo ratings yet
- Varicose VeinsDocument4 pagesVaricose VeinsNur Hanani KhanNo ratings yet
- Deep Vein Thrombosis: P Resenter - Dr. SAMRAT SHRESTHADocument69 pagesDeep Vein Thrombosis: P Resenter - Dr. SAMRAT SHRESTHAUsmle GuyNo ratings yet
- Nursing Managment For DVTDocument23 pagesNursing Managment For DVTgvs5zdbcsfNo ratings yet
- Deep Vein ThrombosisDocument12 pagesDeep Vein ThrombosisJohn Jacob100% (1)
- Pulmonary EmbolismDocument28 pagesPulmonary EmbolismMohamedEzzNo ratings yet
- Venous Thromboembolic DiseaseDocument27 pagesVenous Thromboembolic DiseaseAndra BauerNo ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisGladys YaresNo ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisGladys YaresNo ratings yet
- Non Pharmacological Method For Prevention and Treatment ofDocument34 pagesNon Pharmacological Method For Prevention and Treatment ofBhaskar Borgohain100% (2)
- RT 255 14 Veno IVCDocument89 pagesRT 255 14 Veno IVCSusanti Shanty100% (1)
- Thromboembolitic Diseases in PregnancyDocument31 pagesThromboembolitic Diseases in PregnancyMuwanga faizoNo ratings yet
- Bleeding DisordersDocument56 pagesBleeding DisordersDina GamalNo ratings yet
- DVTDocument46 pagesDVTLuqman ArifNo ratings yet
- Bailey S1Document17 pagesBailey S1hazama kurroNo ratings yet
- Vascular RehabilitationDocument10 pagesVascular RehabilitationSuman DeyNo ratings yet
- Deep Vein ThrombosisDocument15 pagesDeep Vein ThrombosisAngela TenorioNo ratings yet
- DEEP Vein ThrombosisDocument72 pagesDEEP Vein ThrombosisRazib Alam100% (1)
- Deep Vein Thrombosis (DVT) : DisclaimerDocument9 pagesDeep Vein Thrombosis (DVT) : DisclaimerKaka FebriantoNo ratings yet
- Penyakit VenaDocument37 pagesPenyakit VenaSarah JR Nur AzizahNo ratings yet
- Deep Vein ThrombosisDocument43 pagesDeep Vein Thrombosisoctaviana_simbolonNo ratings yet
- Acute Limb IschemiaDocument16 pagesAcute Limb IschemiaMohammad Husni BanisalmanNo ratings yet
- ThrombosisDocument21 pagesThrombosisBEA RADANo ratings yet
- Hemo Dynamic DisDocument49 pagesHemo Dynamic Disjuna danadyaksaNo ratings yet
- DVT 141203103638 Conversion Gate01Document57 pagesDVT 141203103638 Conversion Gate01YantoNo ratings yet
- Varicose VeinsDocument7 pagesVaricose VeinsTarran PhagooNo ratings yet
- DVT and PEDocument56 pagesDVT and PEDefriyan RamziNo ratings yet
- ThrombosisDocument36 pagesThrombosisNAYEEMA JAMEEL ANUVANo ratings yet
- Deep Vein ThrombosisDocument16 pagesDeep Vein ThrombosisB1 TutorialNo ratings yet
- Презентация англDocument49 pagesПрезентация англRajveerNo ratings yet
- Unilateral Leg Swelling 1Document67 pagesUnilateral Leg Swelling 1maryam tariqNo ratings yet
- 2.4. Vena LimfeDocument28 pages2.4. Vena Limfeira citraNo ratings yet
- Peripheral Vascular Disease Arteries NHSDocument10 pagesPeripheral Vascular Disease Arteries NHSAdahl HetheringtonNo ratings yet
- Flow Chart For Pinsky-Vincent Protocol: Intensive Care UnitDocument5 pagesFlow Chart For Pinsky-Vincent Protocol: Intensive Care UnitRaditya Indah TofaniNo ratings yet
- Anatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, LudhianaDocument56 pagesAnatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, Ludhianapreet kaurNo ratings yet
- CLIX ECG Tutorial Part 3 Ischaemia EtcDocument97 pagesCLIX ECG Tutorial Part 3 Ischaemia Etcdragon66No ratings yet
- Copd Thesis 1Document81 pagesCopd Thesis 1arun sagarNo ratings yet
- NCM 118 L 3rd ExamDocument3 pagesNCM 118 L 3rd Examj UNo ratings yet
- PaedsDocument17 pagesPaedsmierahNo ratings yet
- Ehu 281Document62 pagesEhu 281rawahyudiNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- Evaluation of Chest Pain in The Pediatric PatientDocument21 pagesEvaluation of Chest Pain in The Pediatric PatientRoberto Delfin CotaNo ratings yet
- Pediatric-Intensive-Reviewer 240122 101724Document25 pagesPediatric-Intensive-Reviewer 240122 101724venuspiolopacan28No ratings yet
- Monitoring Hipertensi Andi NasirDocument6 pagesMonitoring Hipertensi Andi NasirBabay JamNo ratings yet
- Chapter 13 Drugs Used in Heart FailureDocument7 pagesChapter 13 Drugs Used in Heart FailureChristine Annmarie TapawanNo ratings yet
- NICE Prophylaxis Against Infective EndocarditisDocument5 pagesNICE Prophylaxis Against Infective EndocarditisNaomiAnneDomnicNo ratings yet
- Teaching Plan For HypertensionDocument6 pagesTeaching Plan For HypertensionKasey LacharonNo ratings yet
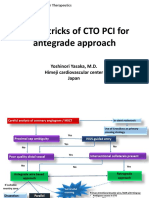
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocument21 pagesTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureNo ratings yet
- DKD and Sglt2iDocument61 pagesDKD and Sglt2iماكريلا المصريNo ratings yet
- Ascites of Cardiac Origin in A Dog - A Case StudyDocument3 pagesAscites of Cardiac Origin in A Dog - A Case StudyFaisal MohommadNo ratings yet
- 31st WECOC 2019 PDFDocument152 pages31st WECOC 2019 PDFgkats001No ratings yet
- .Pulse Oximetry..)Document7 pages.Pulse Oximetry..)Kristzel Peralta FerrerNo ratings yet
- Venous Intervention - GSV Ablation FINALDocument43 pagesVenous Intervention - GSV Ablation FINALaaaaaaNo ratings yet
- Accelerated Idioventricular RhythmDocument5 pagesAccelerated Idioventricular RhythmMed AmineNo ratings yet
- Defect (VSD) Occurs: Decreased Cardiac Output Related To IndependentDocument5 pagesDefect (VSD) Occurs: Decreased Cardiac Output Related To IndependentPrincess GarciaNo ratings yet
- Circulatory System Class 5Document20 pagesCirculatory System Class 5zoey9099747888No ratings yet
- 411 Lab 6Document9 pages411 Lab 6475pqfvvf8No ratings yet
- JZareh Coarctation Aorta Case PresDocument13 pagesJZareh Coarctation Aorta Case PresJesse Helmut Hansen-BartelNo ratings yet
- Pediatric AnesthesiaDocument2 pagesPediatric AnesthesiaPanhavatey0% (1)
- ECG Minesota CodeDocument7 pagesECG Minesota CodeIman AzrbjNo ratings yet