Download as pptx, pdf, or txt
You might also like
- EINC Checklist - DOHDocument2 pagesEINC Checklist - DOH2A - Nicole Marrie Honrado100% (4)
- MastitisDocument13 pagesMastitisapi-232713902No ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanJohann OrtizNo ratings yet
- Case Analysis RLE MODULE TEMPLATE Nursery 1 (One)Document7 pagesCase Analysis RLE MODULE TEMPLATE Nursery 1 (One)PanJan BalNo ratings yet
- Charting (Sample)Document9 pagesCharting (Sample)Zarah Joy Tabuyan100% (3)
- Thailand Traditions and BeliefsDocument6 pagesThailand Traditions and Beliefsapi-316342033100% (1)
- Health Teaching Plan Age 76Document2 pagesHealth Teaching Plan Age 76Mandy Martin100% (1)
- 52389924-IV-therapy NotesDocument57 pages52389924-IV-therapy Notesrye08No ratings yet
- TLG IV TherapyDocument10 pagesTLG IV TherapyStephanie Joy EscalaNo ratings yet
- Competency Appraisal 1Document30 pagesCompetency Appraisal 1mirai desuNo ratings yet
- Nursing Skills ChecklistDocument6 pagesNursing Skills Checklistapi-433883631No ratings yet
- NCP IcuDocument2 pagesNCP IcuDiana MuañaNo ratings yet
- 2nd Lecture Normal Phsiological Changes of Aging Final1.Ppt40-41Document85 pages2nd Lecture Normal Phsiological Changes of Aging Final1.Ppt40-41halayehiahNo ratings yet
- Multiple Choice Test QuestionsDocument6 pagesMultiple Choice Test QuestionsNicole MaeNo ratings yet
- Involving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialDocument10 pagesInvolving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialAngel MayNo ratings yet
- ProfadDocument53 pagesProfadtetmetrangmail.com tet101486No ratings yet
- Skills Mechanical Aids in WalkingDocument3 pagesSkills Mechanical Aids in WalkingEiichiro BertoNo ratings yet
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaNo ratings yet
- Nutrition Program: Common Nutritional Deficiencies 1. Vitamin A 2. Iron 3. IodineDocument26 pagesNutrition Program: Common Nutritional Deficiencies 1. Vitamin A 2. Iron 3. IodineKyla OcampoNo ratings yet
- Discharge PlanDocument1 pageDischarge PlanShop Dzubiri HereNo ratings yet
- Factors Affecting Mental HealthDocument4 pagesFactors Affecting Mental HealthGeorge BendanilloNo ratings yet
- Routes of Drug Students)Document5 pagesRoutes of Drug Students)yabaeve100% (1)
- NCM 119 Assignment Galutan Kimberly Erika FDocument5 pagesNCM 119 Assignment Galutan Kimberly Erika Faaron tabernaNo ratings yet
- Case Studies: Case Study 1: Youth and Sexual HealthDocument4 pagesCase Studies: Case Study 1: Youth and Sexual HealthVijay SharmaNo ratings yet
- ESSENTIAL INTRAPARTUM NEWBORN CARE (Assisting and Handling Delivery)Document4 pagesESSENTIAL INTRAPARTUM NEWBORN CARE (Assisting and Handling Delivery)Hannah Angelu CabadingNo ratings yet
- Clinical PaperDocument18 pagesClinical PaperlhhjklllNo ratings yet
- MCN 4th QuizDocument27 pagesMCN 4th Quizastraeax pandaNo ratings yet
- CHN 2 Session 5 SASDocument11 pagesCHN 2 Session 5 SASrica sebabillonesNo ratings yet
- Saint Louis University: School of NursingDocument1 pageSaint Louis University: School of NursingheatherNo ratings yet
- Foreign Body Airway ObstructionDocument15 pagesForeign Body Airway ObstructionKristine Anne SorianoNo ratings yet
- Integrated Management of Childhood Illness (IMCI) : Guide For Clinical PracticeDocument79 pagesIntegrated Management of Childhood Illness (IMCI) : Guide For Clinical PracticeCAREZAMBIA100% (1)
- MMDSTDocument1 pageMMDSTJaic Ealston D. TampusNo ratings yet
- Unit 6 Educational ApplicationsDocument10 pagesUnit 6 Educational ApplicationsBea Bianca CruzNo ratings yet
- Nursing Interview Guide To Collect Subjective Data From The Client Questions RationaleDocument19 pagesNursing Interview Guide To Collect Subjective Data From The Client Questions RationaleKent Rebong100% (1)
- CHN 2 Session 6 SASDocument10 pagesCHN 2 Session 6 SASrica sebabillonesNo ratings yet
- PointersDocument49 pagesPointersStephanie Villanueva AdvinculaNo ratings yet
- Home Visit: Barangay Health ServicesDocument32 pagesHome Visit: Barangay Health ServicesNessa Layos MorilloNo ratings yet
- Module 3 Responsibilities of A Beginning Nurse ResearcherDocument9 pagesModule 3 Responsibilities of A Beginning Nurse ResearcherCaitlynNo ratings yet
- Midterm Topics After Hygiene 1Document39 pagesMidterm Topics After Hygiene 1Budoy WashupapiNo ratings yet
- FDARDocument17 pagesFDARLylibette Anne CalimlimNo ratings yet
- Lesson 2: Different Fields of Community Health NursingDocument8 pagesLesson 2: Different Fields of Community Health NursingClare AlcoberNo ratings yet
- Family Nursing ProcessDocument4 pagesFamily Nursing ProcessAdri SinclaireNo ratings yet
- Ob QuestionsDocument7 pagesOb Questionslbordonada100% (1)
- NCM 112 E LEARNING AutosavedDocument7 pagesNCM 112 E LEARNING AutosavedMikko McDonie VeloriaNo ratings yet
- Maladaptive Patterns of BehaviorDocument97 pagesMaladaptive Patterns of BehaviorKimTot OctavianoNo ratings yet
- Heart and Neck VesselsDocument3 pagesHeart and Neck VesselsMark ElbenNo ratings yet
- Part 4. Gordons Functional PatternDocument4 pagesPart 4. Gordons Functional PatternStephNo ratings yet
- Assessment of The Ears - StudentDocument8 pagesAssessment of The Ears - StudentSherinne Jane CariazoNo ratings yet
- Basic Laparotomy InstrumentsDocument10 pagesBasic Laparotomy InstrumentsJordan Cruz100% (1)
- PNS Pain Management Guideline For Nursing CompetencyDocument10 pagesPNS Pain Management Guideline For Nursing Competencyvhon100% (1)
- Ineffective Tissue PerfussionDocument2 pagesIneffective Tissue Perfussionmonico39No ratings yet
- Computation For Medication and Iv RegulationDocument14 pagesComputation For Medication and Iv RegulationKarlo BallonNo ratings yet
- Applications LETTERDocument5 pagesApplications LETTERmichael ricafortNo ratings yet
- CHAPTER 4-Atty AliboghaDocument48 pagesCHAPTER 4-Atty AliboghaPaul EspinosaNo ratings yet
- CHN TopicsDocument19 pagesCHN TopicsKristine AnaenNo ratings yet
- Nurses NotesDocument2 pagesNurses NotesSVPSNo ratings yet
- Newborn AssessDocument19 pagesNewborn AssessMeredith Carroll McSwainNo ratings yet
- Nursing Resource Unit Taking Vital SignsDocument3 pagesNursing Resource Unit Taking Vital Signsdee_day_8No ratings yet
- Volvulus GROUP 4Document7 pagesVolvulus GROUP 41S VILLEGAS GabrielNo ratings yet
- Nursing DiagnosisDocument38 pagesNursing DiagnosisJR Rolf NeuqeletNo ratings yet
- Types of PlanningDocument3 pagesTypes of PlanningScribdTranslationsNo ratings yet
- Glasgow Coma Scale FormDocument1 pageGlasgow Coma Scale Form2A - Nicole Marrie HonradoNo ratings yet
- #6risks To CVDDocument27 pages#6risks To CVD2A - Nicole Marrie HonradoNo ratings yet
- Knowledge and Awareness Level of Contraceptive Usage Among Adolescents in Mankranso of Ahafo-Ano South DistrictDocument7 pagesKnowledge and Awareness Level of Contraceptive Usage Among Adolescents in Mankranso of Ahafo-Ano South District2A - Nicole Marrie HonradoNo ratings yet
- Knowledge, Awareness and Perception On Contraception Among Women of Reproductive Age Attending Senawang Health ClinicDocument7 pagesKnowledge, Awareness and Perception On Contraception Among Women of Reproductive Age Attending Senawang Health Clinic2A - Nicole Marrie Honrado100% (1)
- Gastroesophageal Reflux Disease (Gerd) & Hiatal Hernia: MedsurgicalDocument2 pagesGastroesophageal Reflux Disease (Gerd) & Hiatal Hernia: Medsurgical2A - Nicole Marrie HonradoNo ratings yet
- #7assess CV Function Physical ExamDocument27 pages#7assess CV Function Physical Exam2A - Nicole Marrie HonradoNo ratings yet
- Psychobiologic Bases of BehaviorDocument34 pagesPsychobiologic Bases of Behavior2A - Nicole Marrie HonradoNo ratings yet
- Group 3 - Community DiagnosisDocument91 pagesGroup 3 - Community Diagnosis2A - Nicole Marrie HonradoNo ratings yet
- Hiatal HerniaDocument15 pagesHiatal Hernia2A - Nicole Marrie HonradoNo ratings yet
- I. Community OrganizingDocument2 pagesI. Community Organizing2A - Nicole Marrie HonradoNo ratings yet
- #1anaphy HeartDocument19 pages#1anaphy Heart2A - Nicole Marrie HonradoNo ratings yet
- Concept of Family and The CommunityDocument3 pagesConcept of Family and The Community2A - Nicole Marrie HonradoNo ratings yet
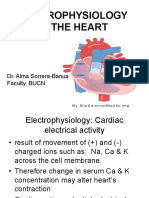
- #2electrophysiology of The HeartDocument8 pages#2electrophysiology of The Heart2A - Nicole Marrie HonradoNo ratings yet
- CHN ReviewerDocument2 pagesCHN Reviewer2A - Nicole Marrie HonradoNo ratings yet
- Promotive and Preventive Health Aspect in CHN & Facts On Healthcare in PHDocument2 pagesPromotive and Preventive Health Aspect in CHN & Facts On Healthcare in PH2A - Nicole Marrie HonradoNo ratings yet
- CHN Reviewer Topic 1Document1 pageCHN Reviewer Topic 12A - Nicole Marrie HonradoNo ratings yet
- CHN ReviewerDocument1 pageCHN Reviewer2A - Nicole Marrie HonradoNo ratings yet
- Focus Charting in Pediatric Ward: Medsurgical ClinicalDocument2 pagesFocus Charting in Pediatric Ward: Medsurgical Clinical2A - Nicole Marrie HonradoNo ratings yet
- HONRADO-Group 3 - Pedia NCPDocument7 pagesHONRADO-Group 3 - Pedia NCP2A - Nicole Marrie HonradoNo ratings yet
- (NOTES 2) Analysis and Interpretation of DataDocument2 pages(NOTES 2) Analysis and Interpretation of Data2A - Nicole Marrie HonradoNo ratings yet
- (NOTES 1) What Is HistoryDocument2 pages(NOTES 1) What Is History2A - Nicole Marrie HonradoNo ratings yet
- Program Implementation With The Health Team: Packages of Essential Services For Primary HealthcareDocument1 pageProgram Implementation With The Health Team: Packages of Essential Services For Primary Healthcare2A - Nicole Marrie HonradoNo ratings yet
- EINC Handout by Nicole Honrado BSN 2ADocument7 pagesEINC Handout by Nicole Honrado BSN 2A2A - Nicole Marrie HonradoNo ratings yet
- Introduction and Organization of USAPANDocument3 pagesIntroduction and Organization of USAPAN2A - Nicole Marrie HonradoNo ratings yet
- Checklist SummarizedDocument1 pageChecklist Summarized2A - Nicole Marrie HonradoNo ratings yet
- Surgical Management of Bowel ObstructionDocument2 pagesSurgical Management of Bowel Obstructionsnay axieNo ratings yet
- Daniel Owusu Ansah Bbas-Ed-173592Document10 pagesDaniel Owusu Ansah Bbas-Ed-173592Richmond AddisonNo ratings yet
- Home (/KB/) / Ophthalmia NeonatorumDocument8 pagesHome (/KB/) / Ophthalmia NeonatorumMohammed Shamiul ShahidNo ratings yet
- Health Promotion: Semester 1 2021Document43 pagesHealth Promotion: Semester 1 2021amisha kumarNo ratings yet
- Imbalance Nutrition Less Than Body RequirementsDocument4 pagesImbalance Nutrition Less Than Body Requirementshatred heartNo ratings yet
- MHS Profiles Uniformed Services UniversityDocument10 pagesMHS Profiles Uniformed Services UniversityMilitary Health SystemNo ratings yet
- Vaginitis and PID: Wanda Ronner, M.DDocument17 pagesVaginitis and PID: Wanda Ronner, M.DHervis FantiniNo ratings yet
- Lec.23 Congenital Abnormalities of Female Genital OrgansDocument5 pagesLec.23 Congenital Abnormalities of Female Genital Organsشريف محمد حسين شريف يوسفNo ratings yet
- Criminal Charges Swine Flu Edits v2 1Document112 pagesCriminal Charges Swine Flu Edits v2 1Kathlyn Stone100% (1)
- The Prevalence of Depression and Anxiety in Iranian Patients With Diabetes Mellitus: A Systematic Review and Meta-AnalysisDocument11 pagesThe Prevalence of Depression and Anxiety in Iranian Patients With Diabetes Mellitus: A Systematic Review and Meta-Analysisselamat parminNo ratings yet
- NCP - Impaired Urinary EliminationDocument3 pagesNCP - Impaired Urinary EliminationFretzgine Lou ManuelNo ratings yet
- ™ COVID-19 Ag Rapid Test Manufactured by Abbott Has Received WHODocument2 pages™ COVID-19 Ag Rapid Test Manufactured by Abbott Has Received WHOAnne Anne HernandezNo ratings yet
- Nutrition PDFDocument669 pagesNutrition PDFDr.Ammar Masood100% (2)
- Advocacy As A Registered NurseDocument3 pagesAdvocacy As A Registered Nurseapi-631170779No ratings yet
- About Cervical CancerDocument18 pagesAbout Cervical Canceramilaa.jNo ratings yet
- Assignment/Tugasan MPU2312 Health and Wellness 1 January Semester 2022Document12 pagesAssignment/Tugasan MPU2312 Health and Wellness 1 January Semester 2022Mohd Akmal Hadi Bin Abu SamahNo ratings yet
- CAPE Unit 2 Biology P2 2019Document17 pagesCAPE Unit 2 Biology P2 2019Ellie100% (1)
- Format of Case Study-121Document4 pagesFormat of Case Study-121Shaina OturdoNo ratings yet
- Rubella VirusDocument14 pagesRubella VirusLincy JohnyNo ratings yet
- Lyme Disease and Tick-Born Co-Infections: Emily Maiella N.D. Montague Integrative Health 413.230.4462Document79 pagesLyme Disease and Tick-Born Co-Infections: Emily Maiella N.D. Montague Integrative Health 413.230.4462Manasi PalavNo ratings yet
- Saida Hal 8-18 "Analisis Faktor Risiko Kejadian Hipertensi ... " Jurnal KeperawatanDocument11 pagesSaida Hal 8-18 "Analisis Faktor Risiko Kejadian Hipertensi ... " Jurnal KeperawatanYanti HarjonoNo ratings yet
- Podiatry Referral Form March 2018Document3 pagesPodiatry Referral Form March 2018HeyNo ratings yet
- Piedmont Medical Center RulingDocument40 pagesPiedmont Medical Center RulingHLMeditNo ratings yet
- JevaxDocument2 pagesJevaxjovedNo ratings yet
- Mego Afek Medical CatalogDocument24 pagesMego Afek Medical CatalogPedro KleinNo ratings yet
- Congenital Heart Disease Lecture NotesDocument8 pagesCongenital Heart Disease Lecture NotesNatukunda DianahNo ratings yet
- Freedom Is Therapeutic Prof John FootDocument2 pagesFreedom Is Therapeutic Prof John FootAna WongNo ratings yet
- Illinois' Medical Cannabis Law SummaryDocument2 pagesIllinois' Medical Cannabis Law SummaryMPPNo ratings yet
- Curriculum VitaeDocument2 pagesCurriculum Vitaebriton11No ratings yet